
Abstract
Background:
Physical exercise improves neurological conditions, but adherence is hard to establish. Dance might be a promising alternative; however, since patients with Huntington’s disease (HD) suffer from rhythmic movement execution deficits, any metric dance practice must be avoided.
Objective:
Here we asked, if contemporary dance, a lyrical dance form, practiced for two hours per week over five months, might improve motor function, neuropsychiatric variables, cognition and brain volume of HD patients.
Methods:
Nineteen patients aged between 43 and 78 years with mild to moderate HD (TFC range 7–13, UHDRS motor score range 3–58) participated in this randomized, controlled pilot study (NCT 01842919). The primary outcome measure was total motor score. Secondary outcome measures were differences in brain structure, cognitive function, neuropsychiatric variables, apathy and quality of life. A semi-structured interview assessed participants’ experiences.
Results:
Adherence to dance classes was very good. All participants completed 5 months of dance practice. Motor impairment (median [IQR] decreased from 28[6–51] to 27[7–33] for the dance group compared to an increase of 19[13–35] - 25[14–42] for usual care, Z = –2.44, p = 0.015). No other behavioral measures showed any changes.
Brain volume increased in the medial superior parietal and paracentral lobule, in line with compensatory structural brain changes in areas supporting spatial and somatosensory processing. These changes were also reflected in patients’ reports that contemporary dance altered the way they “felt and lived in their bodies”.
Conclusions:
Contemporary dance practice, through work on spatial and bodily representations, helps improve motor function in HD patients.
INTRODUCTION
Nothing new lies in the idea that physical exercise improves behavior and brain function [1]. Animal models [2] followed by trials in elderly humans [3, 4] have demonstrated that physical exercise leads to specific increases—namely hippocampal volume, motor and sometimes cognitive [5] function. However, adherence to regular exercise is notoriously difficult to maintain [6, 7]. In one study, the participation rate for two to six months of physical exercise, such as jogging or aerobics was approximately 90%, but this number dropped to 44% afterwards [8]. Other authors observed that only 78% of elderly participants with memory problems adhered to the prescribed physical activity [5]. Attitudes toward physical activity in general, such as lack of interest and self-confidence in the ability to maintain an activity program are important challenges to long-term involvement [6]. In addition, only moderate improvements have been reported, so subtle that neither patients nor family members reported any noticeable change [5, 9]. The absence of improvement perceived by participants might further reinforce drop-out phenomena [9].
These challenges have increased the interest in dance intervention trials to counter the effects of aging and neurodegenerative disease [10, 11]. Furthermore, dance intervention resembles ‘multimodal therapies’ [12], simultaneously stimulating motor and cognitive function, thereby maximizing neurogenesis in animals and humans [13, 14]. Consequently, reports on dance intervention trials have flourished in recent years [12]. In summary, some evidence has been found that dance enhances physical fitness, cognitive, motor and brain function. However, physical practices as diverse as aerobic exercise and argentine tango dancing have been subsumed, even though they must be expected to have rather different cognitive and physical demands and effects on brain and behavior. In consequence, their accessibility and suitability might vary largely according to patient group. The one common factor is the execution of movements to music. Apart from cardiorespiratory demands, what differs greatly from one dance form to another is a) whether dancers practice in interaction with one another or focused on themselves, b) whether movement sequences are repetitive or free, and c) whether the execution of the movement to music is metric or non-metric [15, 16]. Little is known about how dance practice changes the normal brain, since most studies on dance worked with subjects who already had some previous training [17–20] or were already proficient dancers. However, one functional neuroimaging study has measured brain activity of live dancing in a PET scanner [15]. It found superior parietal activity underlying awareness of body positioning in space, and paracentral lobule activity underlying somato-sensory processing, common to different dance conditions. By contrast, metric dancing involved the basal ganglia, whereas non-metric dancing relied on the thalamus and cerebellum [15, 16]. Interestingly, several clinical trials have shown argentine tango to improve motor function in Parkinson’s Disease [20], a highly metric dance form in which a particularly entraining first beat of the bar might help patients overcome movement initiation difficulty. By contrast, this dance form might be particularly unsuitable for patients with Huntington’s disease (HD), for whom the execution of regular, rhythmic movement is particularly difficult, even in early stages [21].
Contemporary dance, rooted in “Freier Tanz” (“free dance”), is based on a sensorial movement experience and there is no learning of precise movement sequences, as opposed to ballet [22]. Dance teachers provide themes at various levels of abstraction, which serve as inspiration for dance improvisation [23]. Participants, departing from their own movement and movement capacities [23], explore and make use of organic roots of bodily movement such as gravity, breathing, momentum and tension-relaxation [22]. Participants are further led to work not only with self perception but also perception of their fellow participants, which makes the experience highly social [23].
Here, we sought to measure the effects of five months of contemporary dance practice on motor function, neuropsychiatric variables, cognition and brain volume of patients with HD. Our study was based on a pre-existing dance workshop which had been created for patients with HD and their caregivers at the Pitié-Salpêtrière University Hospital in Paris by two choreographers in 2003 [23]. We expected the practice of contemporary dance to improve motor and cognitive function [12]. Further, we hypothesized that it may lead to structural changes in areas of somatosensory and spatial body processing, such as the somatosensory cortices [24, 25] and superior parietal cortex [15, 26], due to its focus on sensorial movement experiences.
MATERIALS AND METHODS
Participant recruitment and study design
This was a single site randomized, single blind, controlled trial of a contemporary dance intervention compared to usual care. Patients were recruited at the genetics department of the Pitié-Salpêtrière University Hospital. The protocol was approved by the local ethics committee. Recruitment ran from October 2013 to September 2014. Inclusion criteria were genetically confirmed HD, UHDRS (Unified Huntington’s Disease Rating scale) motor score >5, age 18 or above, and motivation to participate. Exclusion criteria were IRM incompatibility, any physical or psychiatric condition that would prohibit the participant from completing the intervention, and previous or concurrent experience with dance practice. All patients gave informed consent before the first assessment. Trial registration number NCT01842919.
At baseline (t1), we assigned patients to either five months of contemporary dance practice (group 1) or to awaiting list receiving usual care (group 2). Assignment was made on an incoming basis, as a function of a previously established random order of 22 originally planned recruitments. All subjects were seen for a second evaluation (t2) after five months. Subsequently, in a continuation phase group 2 also received five months of dance intervention and was reassessed 5 months later (t3), (Fig. 1), permitting additional within-subject analyses. However, we deemed it more ethical to not take away dance practice from group 1 at the end of 5 months, therefore only one group crossed over.
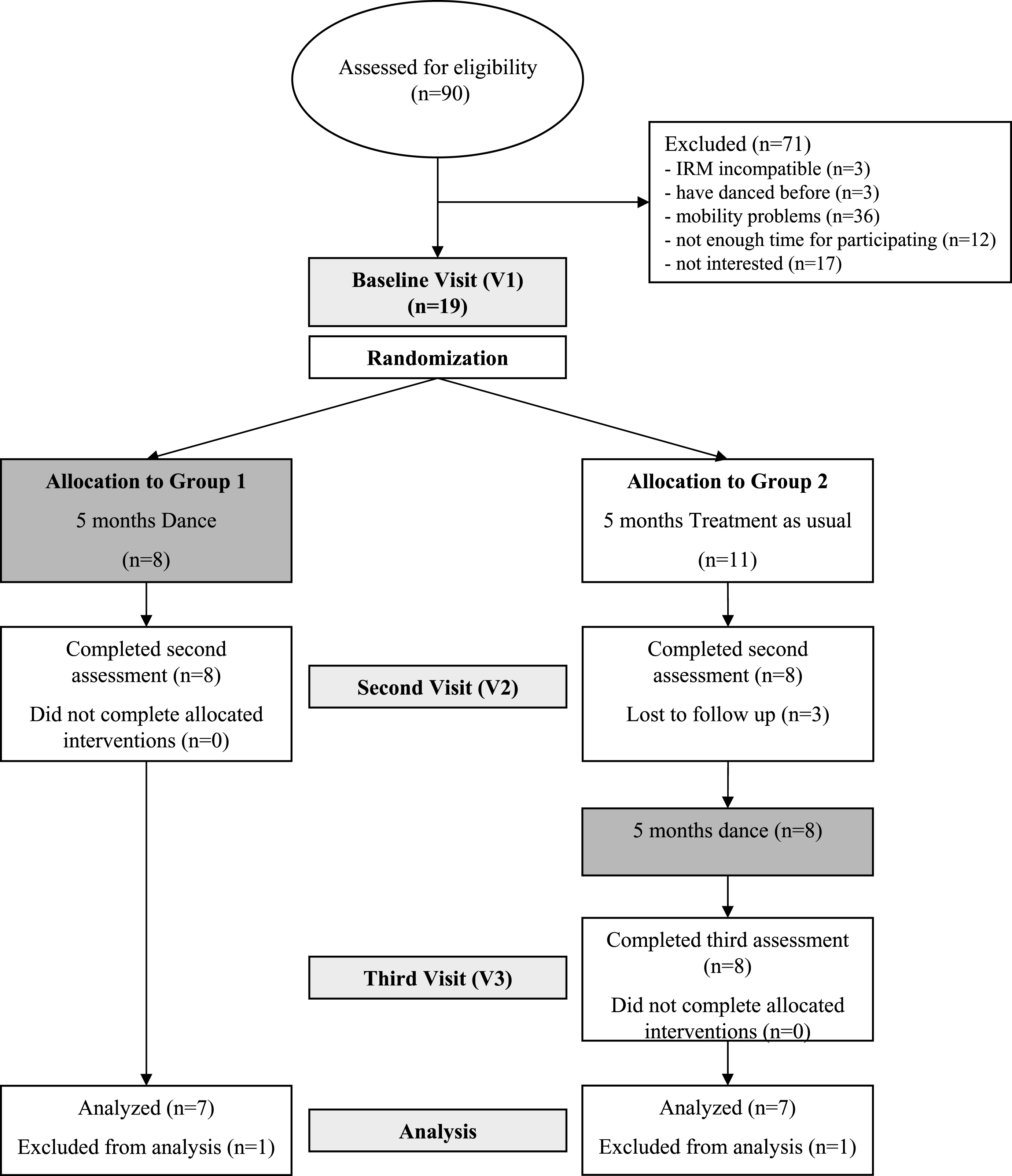
CONSORT Flow chart.
Further, we recruited an age- and education matched control group from non- HD family or friends, in order to compare patients’ behavioral and brain data at baseline.
Intervention
Dancing took place at a contemporary dance studio in downtown Paris. Participants received a calendar with at least one, and up to three dance class options per week from which to choose. They were instructed to take part in at least one two- hour dance class per week. Two professional dancers/choreographers with 10 years of experience teaching contemporary dance to patients with movement disorders ran the intervention sessions. Each workshop consisted of four parts: 1) a warm-up session, including relaxation techniques and body consciousness exercises, followed by part 2) in which participants explored their personal way of moving (with and without music) to a particular theme, e.g., “machines”, “ocean”, “neck”, etc. In part 3) they then improvised dance movements together, using the same theme. Part 4) with auto- and one to one massage exercises on the floor closed each workshop. See Fig. 2 for sketches illustrating participants during a dance workshop.

Sketches taken during a dance class © Renaud Chabrier.
Group 2 participants were asked not to change their everyday life habits during the first five months of participation.
Outcome measures
The UHDRS motor score was the primary outcome measure. Participants were examined at t1, t2, and t3 by a neurologist blinded to group. The secondary outcome measures included the UHDRS cognitive score (including literal fluency, the Stroop task and the Symbol Digit Code [27]), the Mattis Dementia Rating Scale (MDRS [28]), and the Trail Making Test (TMT [29, 30]) for cognitive measurements. Apathy (LARS [31]), problem behavior (PBA-S [32, 33]) and quality of life (QLI, [34]) were also assessed.
Data analysis of clinical measures
Not assuming normal distribution given our relatively modest sample size, we used non-parametric tests, Mann-Whitney U for between subject and Wilcoxon Signed Ranks for within subject comparisons. Differences between controls and patients were assessed at baseline, differences (consecutively referred to as Δ) between t1 and t2 were compared between group 1 and group 2. Furthermore, we ran a within-subject analysis of differences t1-t2 versus t2-t3 of group 2. Finally, we compared the pooled data of all patients’ before (t1 for group 1 and t2 for group 2) and after (t2 for group 1 and t3 for group 2) dance practice. Analyses were performed using SPSS 16.0 (© SPSS Inc.). For PBA-S scores, we limited the analysis to items for which more than one in four patients scored greater than 1 (meaning that problem behavior occurred more than rarely and/or was more than very light) at least one time point, in order not to inflate the analysis with floor effects.
Structural MRI (sMRI) acquisition and voxel-based morphometry (VBM) analysis
Whole-brain three-dimensional (3D) T1-weighted magnetization-prepared two rapid acquisition gradient echo (MP2RAGE) images were acquired on a three Tesla (Siemens) scanner with sequence parameters TR = 5 s; TE = 1.94 ms; TI1 = 700 ms; TI2 = 2500 ms; flip angle (FA)1 = 4°; FA2 = 5°; slice thickness = 1 mm. A parallel imaging (GRAPPA) reconstruction factor of two was used in the phase-encoding direction (antero-posterior, A-P). VBM was performed using Statistical Parametric Mapping version 12 (http://www.fil.ion.ucl.ac.uk/spm). Three analyses were conducted: 1) “CONTROL”, comparing GM volumes between patients and controls; 2) “BETWEEN”: comparing GM differences between t1 and t2 in group 1 (dance) with GM differences between t1 and t2 in group 2 (usual care); 3) “WITHIN”: comparing GM differences between t1 and t2 (usual care) with GM differences between t2 and t3 (dance) in group 2. For CONTROL, initial tissue classification was performed using the unified segmentation process with rigid alignment. For BETWEEN and WITHIN, we first used longitudinal realignment [35], to create an average image and obtain the resulting divergence (dv) data. Segmentation was then performed on these average images. Next, DARTEL [36] was used on the GM images to create a data-specific template for each comparison, which was further registered to the Montreal Neurological Institute (MNI) space using affine transformation. This transformation and the DARTEL flow-fields were used to warp the GM/dv images respectively in a way that preserved their local tissue volumes. Finally, images were smoothed with a 6 mm full width at half maximum kernel. For the CONTROL analysis, we compared GM volumes using a between subjects t-test, additionally entering total intracranial volume as a covariate of no interest. A between subjects t-test on dv images (group 1 t2 > t1 > group 2 t2 > t1) was run for BETWEEN and a within subjects t-test on dv images (group 2 t3 > t2 > group 2 t2 > t1) for WITHIN. In all cases, an explicit binary mask was applied to the statistical model, generated using the optimal thresholding technique [37]. We report significant grey matter in MNI space [x,y,z] at P < 0.001, with a minimum cluster size (k)>6 voxels, without correcting for multiple comparisons. Therefore, we restricted our interpretations to areas for which we had a priori hypotheses based on pre-existing literature. Anatomical localizations were based on Duvernoy’s brain atlas [38].
Semi-structured interview
Participants were asked to freely associate what came to their mind in response to the key word “atelier de danse” (“the dance class”). Answers were recorded and transcribed. In a second step, statements were classified into keywords and quantified.
RESULTS
Baseline characteristics
We were able to recruit nineteen HD patients (11 women and 8 men) and 12 controls (eight women and four men) for participation within the limited recruitment period. The patients’ ages ranged from 43 to 78 years with a median of 53 years, and formal education was 15 (13–16.25) years. The controls’ ages ranged from 44 to 72 years with a median of 53 years, and formal education was 15.5 (12.8–17.3) years. Patients and controls were matched for gender (Fisher’s exact test, p = 0.717), age (Z = –0.689, p = 0.49), and years of formal education (Z = –0.571, p = 0.568). The median expanded CAG repeat length was 43 [39–41], median disease burden, calculated as ([age at testing - 35.5] * CAG repeat length), 398 (344.5–433.5)) and patients’ Total Functional Capacity (max = 13) 11 (10.5–12). Six patients and two controls were on selective serotonin reuptake inhibitors (SSRI), three patients were on serotonin- and noradrenalin reuptake inhibitors (SRI/NARI), three on olanzapines and two on benzodiazepines.
Drop outs
Three patients in group 2 were lost to follow up, before returning to t2. Data of one patient in group 1 and one patient in group 2 had to be excluded from the analysis because treatment changed with the addition of tetrabenazine during the course of the trial.
Intervention
A total of 125 dance classes were taught with a median of six [4–7] classes per month. The number of participants per dance class varied from one to ten with a median of four [3–5]. The number of dance classes taken during the five- month interval ranged from 11 to 21 in group 1 with a median of 12 [12–15], corresponding to 0.63 times per week (0.50–0.76), and from 1 to 24 in group 2 with a median of 14 [7–20], corresponding to 0.58 times per week (0.43–0.94), p = 0.85.
Comparison with controls (Table 1)
Patients scored significantly worse than controls on the primary outcome measure UHDRS motor scale. For secondary outcome measures, patients scored significantly worse than controls only on the cognitive test-scores MDRS, Stroop, and TMTA, in line with their general high TFC. For neuropsychiatric variables, only PBA ‘Irritability’ and ‘Lack of initiative’ scores were significantly different between patients and controls. Apathy scores did not differ between patients and controls. Quality of life ratings were also not different between patients and controls.
Behavioral measures, patients versus controls
shown are medians and 25th and 75th percentiles. †Problem Behaviour Assessment, items for which at least 25% of patients scored >0. ‡LARS: Lille Apathy Rating Scale (Sockeel et al., [31]). §QLI (Ferrans & Powers, [34]).
Primary outcome measure UHDRS motor score (Table 2a, Fig. 3a)
Δt2-t1 was significantly different between group 1 (dance) and group 2 (care as usual) (mediangroup1 - t1 28 [6–49], mediangroup1 - t2 27 [7–33], mediangroup2 - t1 19 [13–35], mediangroup2 - t2 25 [14–40], Z = –2.44, p = 0.015). Δt3-t2 (care as usual) was not significantly different from Δt2-t1 (dance) in group 2 (mediangroup2 - t3 18 [12–35], Z = –1.52, p = 0.128). Δafter-before dance was significantly different, when all patients were pooled together (medianbefore 26.5 (12.75–43.75), medianafter 24.5 (11.75–35.5), Z =–1.97, p = 0.05).
Behavioral measures, patient group and before-after comparisons
shown are medians and 25th and 75th percentiles. †Problem Behaviour Assessment, items for which at least 25% of patients scored >0. ‡LARS: Lille Apathy Rating Scale (Sockeel et al., [31]). §QLI (Ferrans & Powers, [34]).
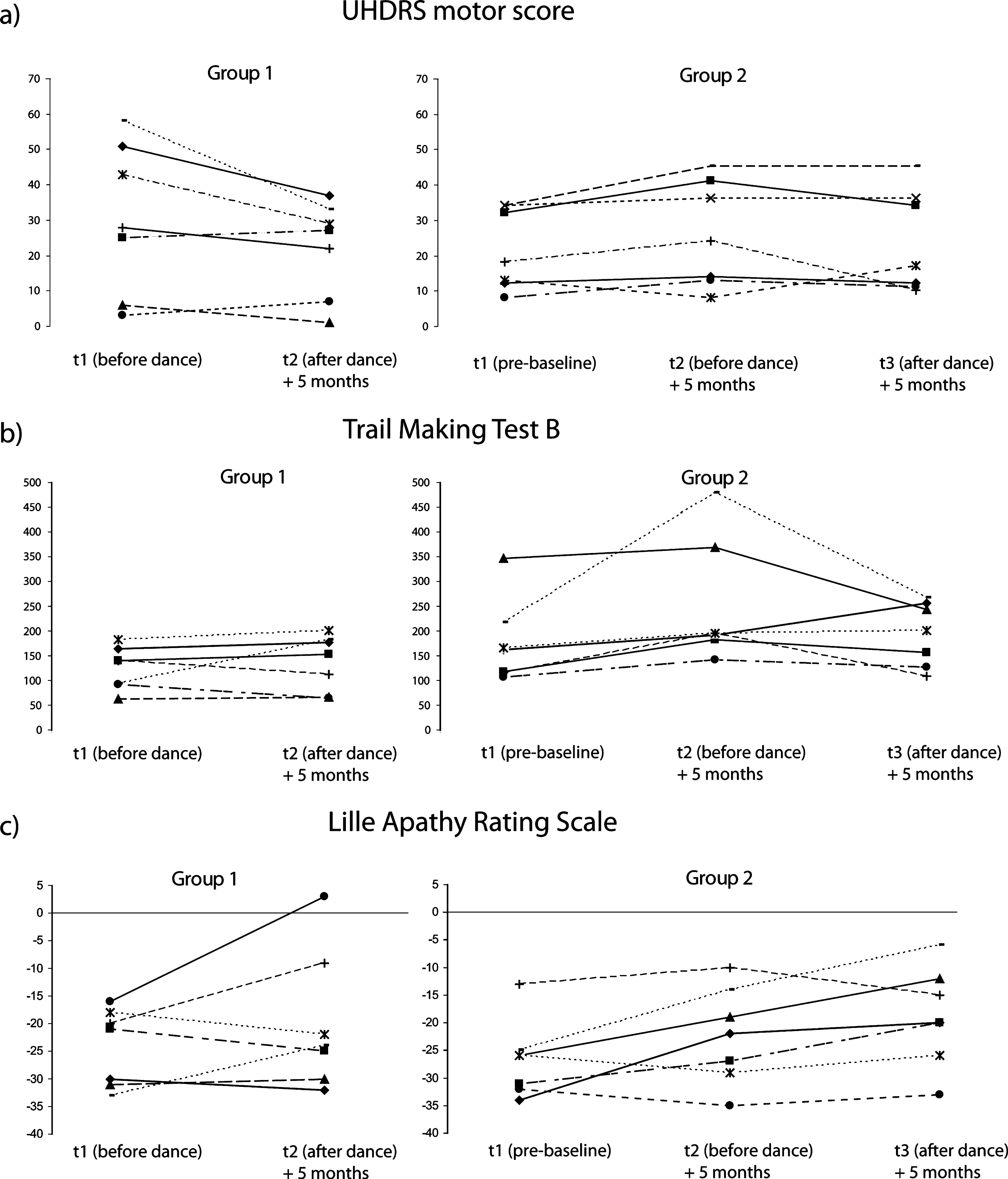
Behavioral outcome measures. Line diagrams displays of before-after dance for Group 1 and baseline-before-after dance for Group 2. A) Motor scores improve significantly with dance. B) Executive function as measured by Trail Making Test B. TMT B scores worsen significantly without dance. C) Apathy scores increase across time, regardless of dance practice.
Secondary outcome measures (Table 2b, Fig. 3b, 3c)
Cognitive test scores
The only significant Δt2-t1 difference between group 1 and group 2 was for the TMTB. Δt3-t2 was also different for the TMTB from t2-t1 in group 2. No after-before Δdifference was observed over all patients pooled together.
Neuropsychiatric variables
There were no Δt2-t1 differences between group 1 and group 2 for any PBA-S variables, none between t2-t1 and t3-t2 in group 2, and none between after-before dance for all patients pooled together. There was however a trend for apathy scores to worsen over time, regardless of dance.
Quality of life
There was a trend towards a higher t2-t1 difference in group 2 compared to group 1, thus for the interval in which they did not dance.
VBM results (Fig. 4)
Comparison with controls
Patients had significantly less grey matter in the striatum bilaterally than controls (caudate and putamen: [–9, 9, 5], T = 6.17, p = 0.000002, k = 1411; [20, –2, 17], T = 6.07, p = 0.000003, k = 654; [26, 2, 8], T = 4.78, p = 0.00006, k = 438; [–30, –14, –8], T = 4.69, p = 0.00007, k = 58), as well as in the right superior temporal gyrus ([41, –63, –14], T = 4.75, p = 0.00006, k = 40).
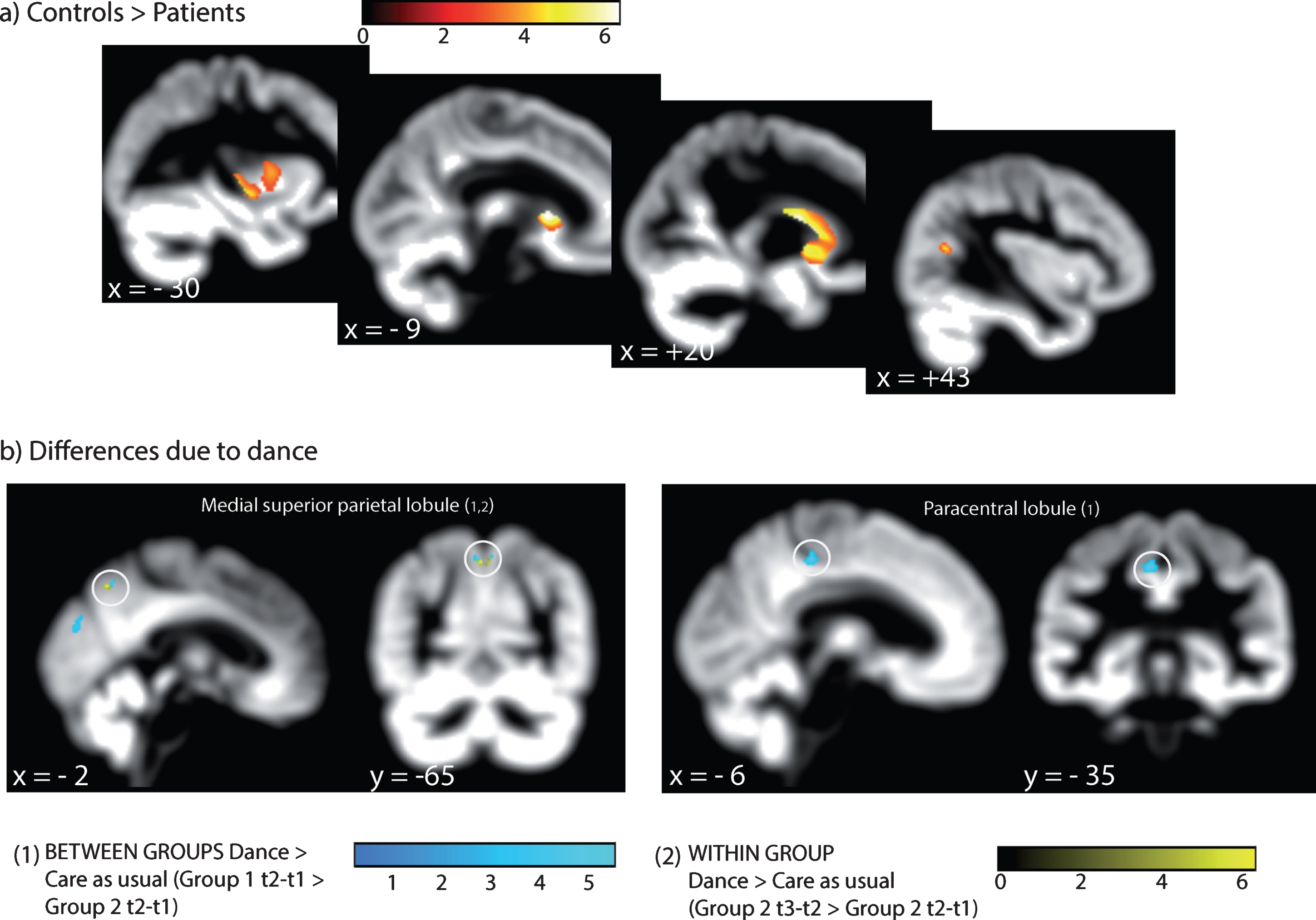
Structural brain differences i) between patients and controls and ii) due to dance. A) Δdifferences between t1 and t2 in group 1 (dance) and t1 and t2 in group 2 (usual care). B) Δdifferences between t1 and t2 (usual care) and t2 and t3 (dance) in group 2. Displayed on the DARTEL transformed average 3DT1 image at p < 0.005, uncorrected, for better visibility.
Differences with dance
The Δdifferences between dance (group 1) and usual care (group 2) yielded significant GM voxels in the left medial superior parietal lobule ([–3, –65, 51], T = 5.66, p = 0.00005, k = 7), left paracentral lobule ([–6, –35, 48], T = 4.96, p = 0.00017, k = 18) and medial superior occipital gyrus ([0, –80, 29], T = 4.43, p = 0.0004, k = 9). We found no significant voxels for the within group comparison before (group 2 t2 > t1) and after dance (group 2 t3 > t2) at the set threshold, but there was one significant voxel in the medial superior parietal lobule ([–2, –65, 50], T = 6.33, p = 0.0004), when inclusive masking with group 1 t2-t1 > group 2 t2-t1 was applied.
Semi-structured interview results
The most frequently mentioned keyword was “body” (e.g., “learning about my body”, “re-appreciating my body”, “learning to live in my body”, “communicate through my body”, n = 9), followed by “encounter” (e.g., “meeting others”, “connect with people”, n = 8). Related to this phrase, four participants mentioned “get to go out again”, thus a feeling of improved societal partaking. Furthermore, five participants mentioned “space” (“having space”, “using space”, “be conscious of space”, “be aware of space”, “be in the space bodily”). Five participants each mentioned “relaxation” and “joy”.
Dance class adherence post intervention
We were able to obtain follow up information on dance class adherence after the end of the study for 10 months for all 14 participants and for 15 months for 13 participants. 13 of 14 participants (93%) continued 10 months post protocol for a median of 11 [9–14] classes in the first five months post protocol, and a median of 7 [5–10] classes in the five to 10 months post protocol. 11 of 13 participants (85%) continued 15 months post protocol for a median of 6 [2–7] classes.
DISCUSSION
Improved motor function
Five months of contemporary dance significantly improved motor function of HD participants. As can be seen in Fig. 3, the effect is composed of a visible worsening of motor function over five months in the care as usual group, and a flattening or reversal of the UHDRS motor curve with dance practice. These promising findings are consistent with the observation that people who have danced habitually throughout lives have better balance and less variable gait than non-dancers [39, 40]. It is further compatible with the motor improvements seen in elderly participants of a dance step sequences training program [41] and with motor improvements in Parkinson’s Disease after tango dance training [20]. However, not all dance is the same, and it is perhaps surprising that an apparently gentle and highly accessible exercise form such as contemporary dance can yield similar results to a tailored one-to-one physical exercise program [7]. These promising findings notwithstanding, we are not claiming as of yet that dance intervention could be considered as disease modifying [58]. Our study design aimed to show a treatment effect rather than a disease modifying effect. For the latter, a greater number of participants would be required and observation would have to be over a longer period.
As can also be seen from Fig. 3a, motor impairment of the patients taking part in this study initially varied from hardly noticeable up to nearly 60 on the UHDRS motor scale. Interestingly, improvements can be observed throughout the range, suggesting that contemporary dance practice might be an interesting remedy for people with HD from presymptomatic to advanced stages. Note that this study only included patients with a relatively high functional score, in line with the requirement that they travel to the contemporary dance studio in downtown Paris by themselves every week and that they are found able to partake in group practice (absence of problem behavior). However, because this dance form decidedly adapts to each person’s movement capacities, it would be feasible to conceive of a form of this type of workshop for more impaired patients, for example in specialized care centers. Future studies should investigate contemporary dance practice in people with HD of all stages. A further interesting point of future investigation in larger cohorts concerns the possibility of differential development of the UHDRS motor subscores such as postural, chorea and voluntary movement impairment with contemporary dance practice.
Brain changes
We provide preliminary evidence that contemporary dance induced brain volume changes in the superior parietal and somatosensory cortices. Even though we used a highly sensitive within-subject longitudinal realignment procedure [35], these findings will need to be replicated in a bigger sample size. However, they are in accordance with the idea that contemporary dance, focusing strongly on sensorial movement experience, would solicit these brain areas, related to spatial and body representations. A functional implication for the superior parietal cortex was previously demonstrated for dance movement compared to muscle contractions [15]. This area is part of the sensorimotor integration network, supporting externally guided movement in general [26], thus observed brain changes are in keeping with general motor learning. It contains a kinesthetic map that supports bodily awareness in space [16], which Haggard & Wolpert [42] refer to as “body scheme” (see also 43, 44). Furthermore, the area of somatosensory cortex we identified here lies within 10 mm of dance-related brain activation reported previously [15, 18], pointing to its motor- sensory role, that supports bodily perceptual changes linked to motor learning [25]. Such somatosensory change further occurred as a consequence of observed motor learning in others [45–47], suggesting that dance could be a particularly useful intervention tool (when practiced in a group), because it simultaneously stimulates brain function via both observation and execution of actions.
In contrast, we found no dance-related changes in the basal ganglia. This might also be linked to the fact that basal ganglia are preferentially activated in the execution of motor activities with regular, predictable rhythm, whereas unpredictable unfamiliar temporal patterns recruit other pathways [15, 16]. Alternatively, this may be evidence that areas strongly affected by neural degeneration typical of HD [21], do not profit from this training. Thus, brain changes might be compensatory rather than reparatory [48, 49]. Previous work in premanifest HD discovered compensatory mechanisms in resilient and less affected brain areas and no compensatory activity in motor areas [50]. As these authors argued, the basal ganglia may take a “basic, fundamental role in movement sequencing and postural adjustments in anticipation of volitional movements that can neither be replaced nor compensated for once damaged beyond a certain threshold” (p. 1427).
(No) observed effects on cognitive function and neuropsychiatric variables
We found cognitive changes only in one motor-based executive function task. Again, this might be due to lack of power and the finding should be replicated in a bigger sample. Trends pointed in the right direction and were in accordance with previously found cognitive improvement linked to contemporary dance practice in normal elderly subjects [51]. Concerning neuropsychiatric variables, we largely observed floor effects consistent with relatively unimpaired participants. However, importantly, we observed a trend for slight, but steady increase in apathy, despite dance practice, and in the absence of depression. This adds evidence to the argument that it is clinically relevant to disentangle depression from apathy [31, 52]. Further, for dance or other physical activity teachers, this means that they must develop strategies to overcome the challenge that increasing apathy might come to interfere with long-term adherence.
Subjective impressions for participants
Strikingly congruent with the observed structural brain changes in areas supporting the “body scheme” [42–44], participants reported that dance altered the way they perceived their own body. Further, they highlighted the importance of “meeting others”, improved societal interaction, and expressed joy and pleasure in taking part, which have similarly been reported by dancers with PD [53, 54]. Finally, unlike previous physical exercise intervention programs [5], participants here reported that contemporary dance practice affected their lives positively. Such improvement was not reflected consistently in quality of life scores, which might, however, been because of generally high ratings at baseline (patients did not rate their quality of life different from controls).
Adherence and recommended dose
In contrast to other recent physical exercise trials in HD [7], contemporary dance practice yielded a high adherence rate: no participant dropped out during the five-months contemporary dance practice in either group. Further, all but one (93%) continued for 10 months, 85% continued for at least 15 months after the trial. This is well above the 50% found for self-monitored physical exercise programs [55], and on an equivalent level with reported 86-93% found for two to six months of physical exercise, such as jogging or aerobics, in healthy elderly [8]. High adherence might be tied to high accessibility and enjoyability [10, 11], as well as with its perceived sociability and subjective impression of positive change related to the trial [56].
Despite high overall adherence, though, we observed that weekly participation was lower than instructed during the trial. This might explain the absence of any correlation between motor improvement and number of dance classes taken. Mobility difficulties are likely the underlying problem, which also hampered participant recruitment at the start of the study (see Flow chart, Fig. 1). Practice in a dance center adds to societal integration and a feeling of regained citizenship for patients, but accessibility for disabled people remains an important issue for public policy makers.
Finally, in terms of recommended dose, complementing previous findings in Parkinson’s disease [57], we showed here that effective practice of 120 minutes of contemporary dance practice at least once every two weeks over five months was effective to improve motor function in HD. Other than tango dance, contemporary dance practice is less susceptible to effects of fatigue and can be practiced for two hours per intervention.
Conclusions
Regular contemporary dance practice over five months improved motor function in HD. This was accompanied by preliminary evidence of structural changes in brain areas supporting “body scheme”, namely superior parietal and somatosensory cortices, but not basal ganglia, suggesting compensatory rather than reparatory mechanisms. Together with participants’ own reports, we conclude that contemporary dance might have a specific potential for reducing motor impairment in Huntington’s Disease, by working on bodily and spatial awareness. A particular benefit might come from practicing in a group, which makes it possible to jointly observe and execute actions, simultaneously.
Over and above Huntington’s disease, this form of poetic physical activity might profit many other patient group with reduced mobility and motor impairments.
Adherence rate in our study was high, likely due the perceived sociability. Patients themselves mention the impact of new encounters and renewed participation in social activities and citizenship as central to their better-being. By contrast, the important - public health - challenge remains, how to provide accessibility to dance practice for people with reduced mobility.
CONFLICT OF INTEREST
The authors have no conflict of interest to report.
Footnotes
ACKNOWLEDGMENTS
The authors wish to extend their gratitude to the study participants. They thank Damien Justo for help with neuropsychological battery choices, Coralie Rastel, Hugo Bismuth and Hélène Francisque for neuropsychological testing, Bogdan Draganski and Stéphane Lehéricy for advice in sMRI parameter choices, Romain Valabregue and Cécile Galléa for help with the sMRI data analysis, Philippe Angell for his sensitive English corrections and Renaud Chabrier for his dance class drawings.
This work was supported by the Gossweiler Foundation (Switzerland) and COSSEC, INSERM (France).