
Abstract
Quality management is for providing better resources to the customers. It is applicable for hospitals for giving best services. QM has an initiative i.e. FMEA, which is applicable in the purchasing process of the hospital (PPH) for calculating the RPN, which determines the risks linked with the problems occurring in purchasing the particular equipment for the hospital. RPN is conquered from past experience and engineering decisions which leads to errors and discrepancies. In this study, Neuro-Fuzzy approach based technique is applied to improve the purchasing process in Indian private hospitals. Neuro-Fuzzy approach eliminates insufficiencies in the assessment of the RPN, resulting in saving of time. PPH in India has never been improved before by applying neuro-fuzzy scheme based FMEA technique. Analyzed results show that the applied neuro-fuzzy method is able to solve the problems which arise from conventional FMEA approach and will effectively find out RPN. Proposed method provides quality assurance in the process.
Introduction
Today, the health industry has to be improved. Health managers are trying to utilize advance equipments and advanced scientific methods [1]. Conditions such as increasing costs, restricted budget and strong competition can be improved by proper planning supervision, which affects the hospitals.
Hospitals are working with minimum number of resources, which is a fundamental defect in health care [2]. When there is a need of equipment in the hospital, hospital management should evaluate its requirement in the hospital, which leads to effective purchasing process [3]. Therefore this process of purchasing is important in every hospital.
The tool used commonly in the improvement process are, brain storming, process flow charting, FMEA, DRIVE (define, review, identify, verify, execute),process mapping etc.
Here FMEA based neuro-fuzzy approach is applied for the very first time for improving purchasing process in hospitals.
Different investigations have been performed to increase the effectiveness of FMEA based AI techniques [4–6]. Some research has been done for FMEA based AI technique for purchasing process improvement in hospitals but no research in India.
This paper is organized in eight sections, section 1 presents the introduction of the study, purchasing procedure in a hospital along with its problems and failure modes are described in section 2. Conventional FMEA and proposed approach is introduced in section 3 and 4 respectively. Purchasing process in hospitals by using neuro-fuzzy scheme is discussed in section 5 and 6. Section 7 presents the valuable results and discussions. Section 8 provides some important conclusions drawn from this study.
Purchasing procedure in the hospital
The purchasing process in the hospital is described as given Fig. 1 [4]. Stages of purchasing process in hospital.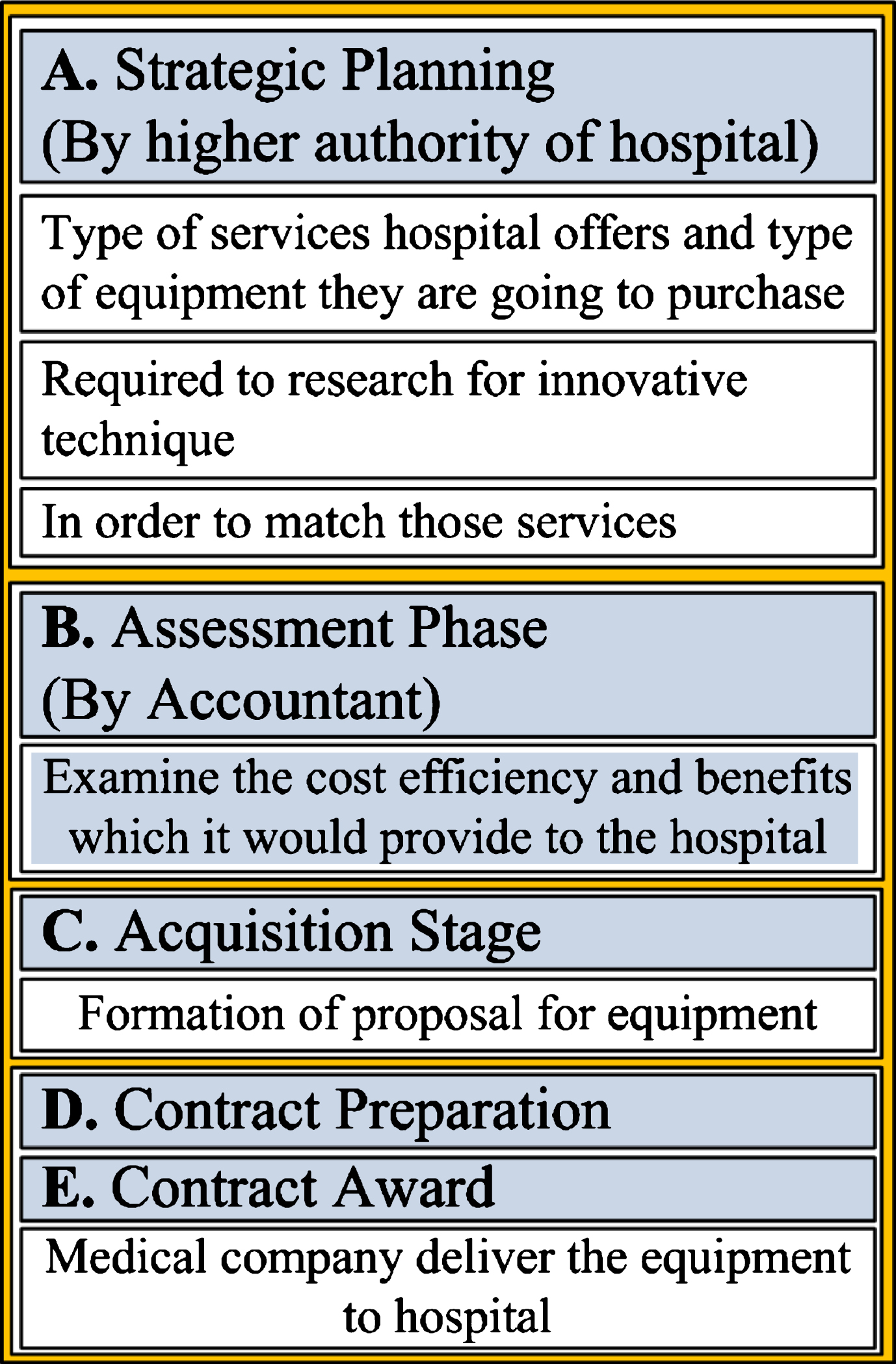
Hospital staff should make note of the thing that the equipment will not only helping them in providing effective and up to date services but also cost effective for hospital and patients [5].
Hospital can go for different procurement methods which are: 1) micro-purchases, 2) bids 3) sole sources [6].
The process of direct procurement and/or tender of medical equipment is shown in Fig. 2 [4], in which there are several problems as listed in Table 1 [4]. Flow chart of medical equipments purchasing process. FM, FE and failure causes [4]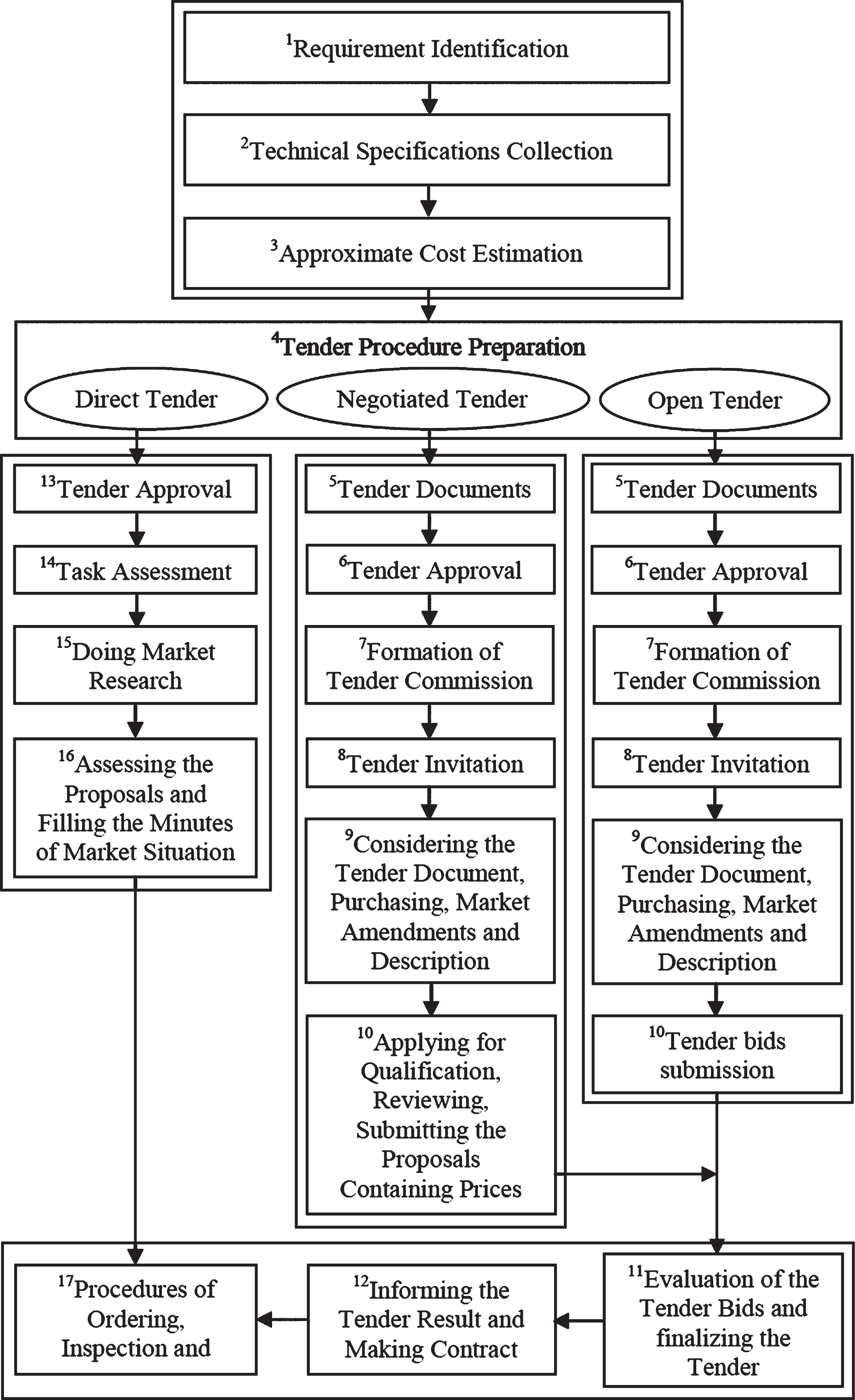
The PPH is not functioning properly. Most of the times, failures were observed at various level of process and were in fact not positive outputs for the health industry. Stages of identification and calculation of different failures are discussed in the next section.
All failure modes delay the purchasing process. The hospital management should have skills to find out various solutions. Increase in time will affect the score. The time wasted in cancelling the contract will differ the score. There is no control on failures for the purchasing process, which is regulated by person. This control exists at every stage of process so there is no any different point of control. Control points are the supervisor’s approval and contractors looking at the tender documents and giving notice to the tender results to every bidder.
It is recommended to eliminate all possible number of failures for improving the purchasing process. When the purchasing process is improved, there is decrease in the cost of purchased products, decrease in cost of purchasing process, better services provided to patients, decrease in investment in inventory.
By applying FMEA to failure, the above mentioned objectives were attained.
Brief detail of FMEA
Failure Mode and Effect Analysis (FMEA) is practiced in hospital in different stages of product life cycle. It is an analytical technique with the combination of technology and vast experiences of people for recognizing the failure mode of a product and trying to remove it [5, 6].
Conventional FMEA utilizes a RPN (risk priority number) to estimate level of risk of a process or a component. RPN is calculated through product of available 3 factors (i.e., D-probability of not detecting the failure, S-severity of the failure and O-probability/occurrence of failure), which is represented mathematically as,
Conventional FMEA utilizes 5 scales and scores of 1 to 10 for measuring the O, S and D. The ranking system of RPN is being utilized for the O, S and D. This is simple but has numerous drawbacks such as: 1) it is assumed that the components of RPN are uniformly weighted [6]. It avoids the relative importance among the O, S and D; 2) The RPN has many replicate numbers [8]. The FMEA make use of risk ranking which is crucially argued [9]; 3) scale of RPN is not intuitive and has not statistical which is achieved by three variables with regards of protection; and traditional RPN has no direct relationship between these variables [6].
While calculating FMEA, exactness is not achieved where data is not reliable and limited. When expertise puts scores from 1 to 10 (performed in the RPN calculation) for the three factors may generate a wrong impersonation, which clarifies the computational work, making a scoring system from probability, arising problems. Relationship between the probabilities and three factors are absolutely non-identical type.
To improve the conventional RPN ranking system, neuro-fuzzy approach is used here for RPN evaluation as explained in sections 4–6.
RPN w.r.t. O, S, and D by Failure Modes [2]
RPN w.r.t. O, S, and D by Failure Modes [2]
The assessment of the FM is done by means of sores to the particular risk factors of O, S, D. 10-level scales are utilized. While giving scores to the risk factors different statistical methods and skilled outlook is proposed. Here, all the risk factors taken were skilled based because there was lack of data of risk factors, and few factors were uncertain.
In identical RPN value situation for different events, proposed approach will compute the risk implication without wastage of time and resources and makes high- risk noticed.
The proposed approach is based on the combination of different artificial intelligence (AI) techniques in single prototype model. Figure 3 shows the proposed approach implementation’s basic steps which uses the results of classical FMEA analysis of purchasing department. Proposed Neuro-fuzzy scheme for purchasing process in a hospital.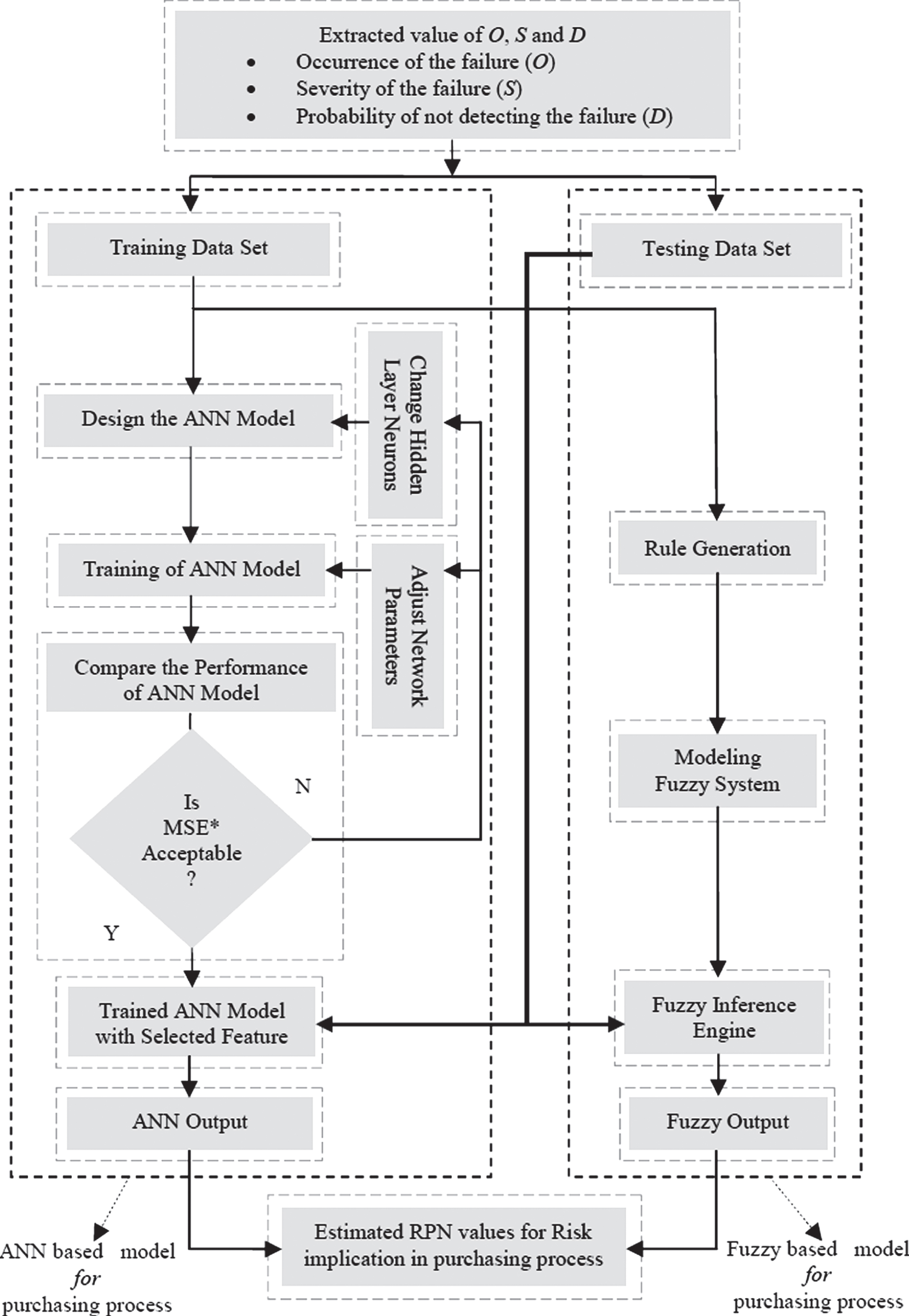
Developed neuro-fuzzy scheme was implemented in purchasing department of a private hospital situated in New Delhi, India. The main objective of this study was to ameliorate PPH by investigating procedure and through evaluating the method which decreases procurement times, expenses and eradicate overloaded needless work. For fair validation purpose of proposed approach, radial basis function (RBF) and generalized regression neural network (GRNN) approach has also been implemented instead of BPNN on the same problem to find out PPH.
Fuzzy logic (FL) is a multi-value logy for dealing with interpretation which is rough not accurate [7–9]. Variables of FL shows a membership value of not 0 nor 1, however a value ranging from 0 and 1. In this the level of a declaration ranges within 0 and 1 and is without guard of two truth values ie true (1), false (0) as in typical logic [7]. Therefore FL gives base of interpretation of not precise in nature. It provides for human reasoning better than the two-valued conventional logic template.
The steps for constructing a fuzzy-logic purchasing system are given in Fig. 4. The Baseline structure of a fuzzy logic control system of purchasing system is shown in Fig. 5. Procedure for Designing a Fuzzy-Logic Model. General scheme of FLPP.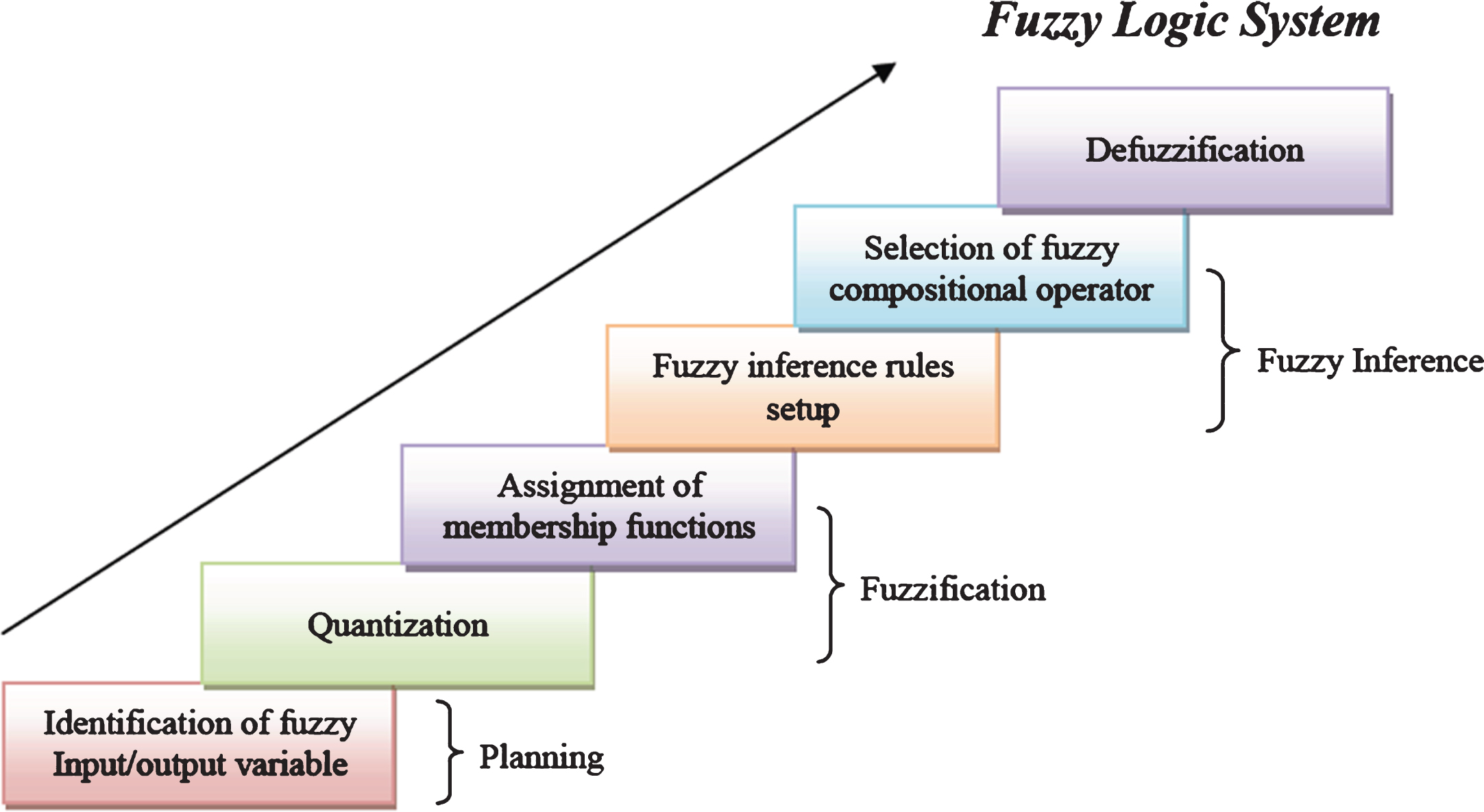

Fuzzy inference utilized for PPH has been studied by various researchers. The steps for constructing a fuzzy-logic model are given in Fig. 4. The schematic diagram of FL based PPH (FLPP) to estimate the RPN values is shown in Fig. 5. FLPP is a new fuzzy-based system which is promiscuous data numeric and linguistic types. The FL purchasing process shows a FL-based complete purchasing process technique comprising the following three phases [8]: selection of
A schematic representation of FLPP of 2nd phase is given in Fig. 5.
Input and output of fuzzy-logic system
O, S and D in FMEA is useful for finding out the risk level of purchasing process based on RPN values of each event so as to compensate the conflict between same RPN value of different events and reduces the wastage of resources, time or entail in some cases a high-risk event going unnoticed.
Although conventional FMEA method is broadly utilized for solving the purchasing process problem in the hospital, but in the many cases, it is very hard to determine the correct risk level of the event especially when the product of O, S and D value for more than one event are identical. For example, consider two set of examples having values of 6, 5, 1 and 5, 6, 1 for O, S and D, respectively. Both these examples will have a total RPN (RPN1 = 6×5×1 = 30 and RPN2 = 5×6×1 = 30), however, risk associated of two events will not be identical. The fuzzy logic technique has more advantages in solving this problem.
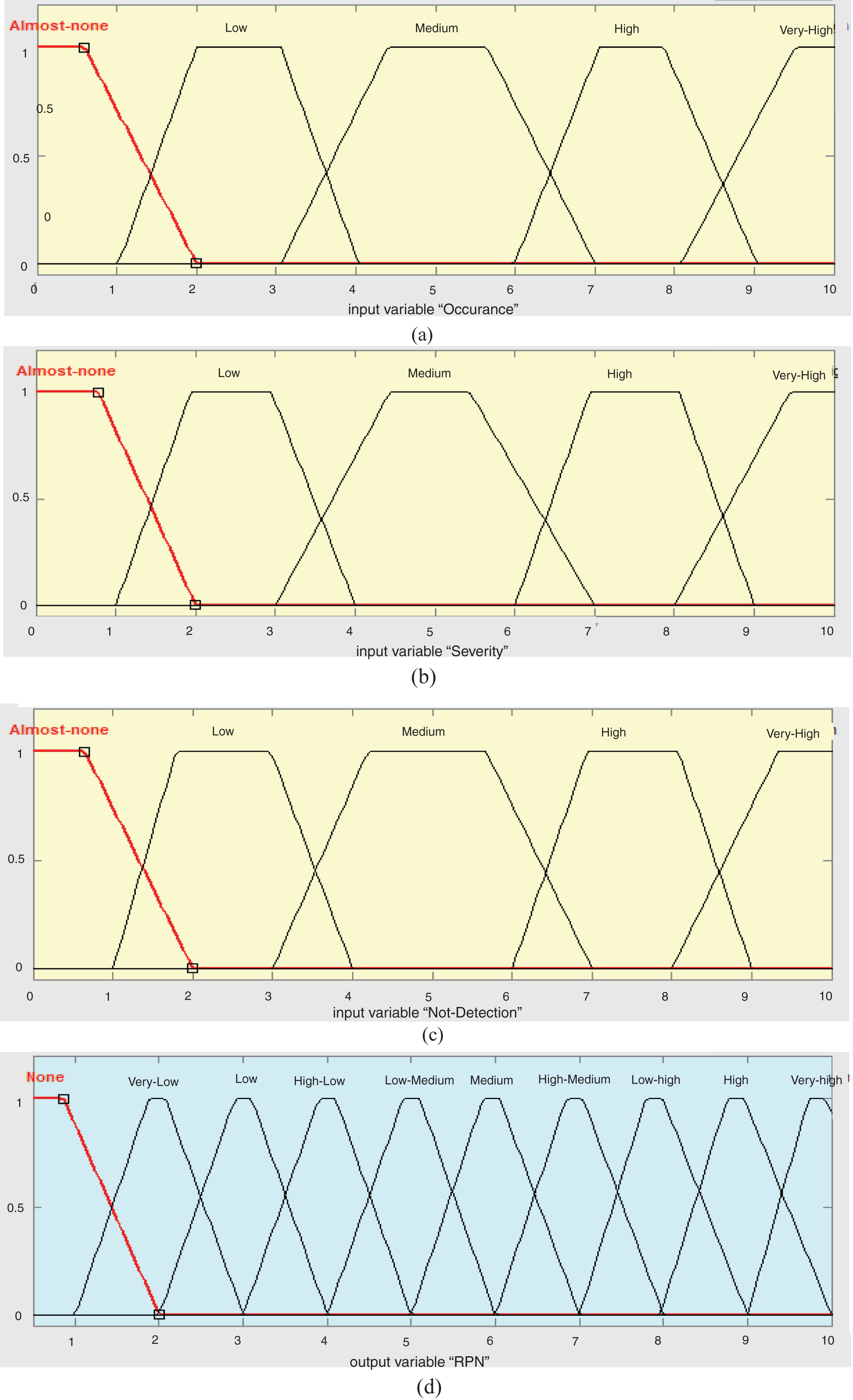
For implementation of FLPP method, MFs for input variables are designed based on the variation of O, S and D as represented in Figs. 6(a-c), 7(a-c) and 8(a-c). The MFs for the output variables (expected RPN value) are represented in (d) part of Figs. 6–8. Triangular MFs (Trimf) of (a) O; (b) S; (c) D and (d) Output variable of RPN. Trapezoidal MFs (Trapmf) of (a) O; (b) S; (c) D and (d) Output variable of RPN. Gaussian MFs (Gaussmf) of (a) O; (b) S; (c) D and (d) Output variable of RPN.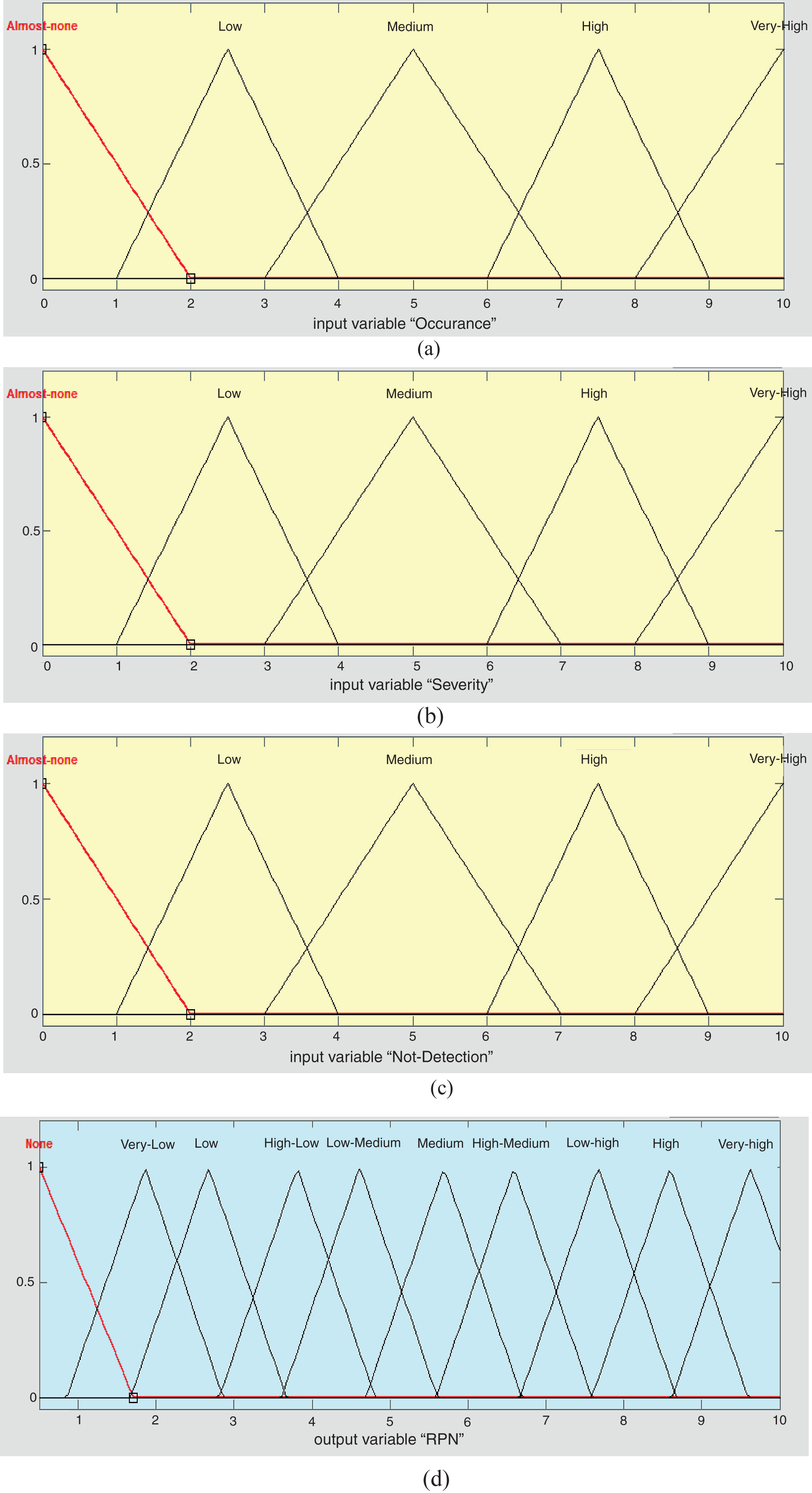

Rule viewer’s rules for estimated output variable of RPN
Where; Occurrence of the failure-O (O1 to O5), Severity of failure-S (S1 to S5) and Probability of not detecting the failure-D (D1 to D5) are the fuzzy input variables and output variables are RPN values (None(N), Very low(VL), Low(L), High low(HL), Low medium(LM), Medium(M), High medium(HM), Low high(LH), High(H), Very high(VH)).
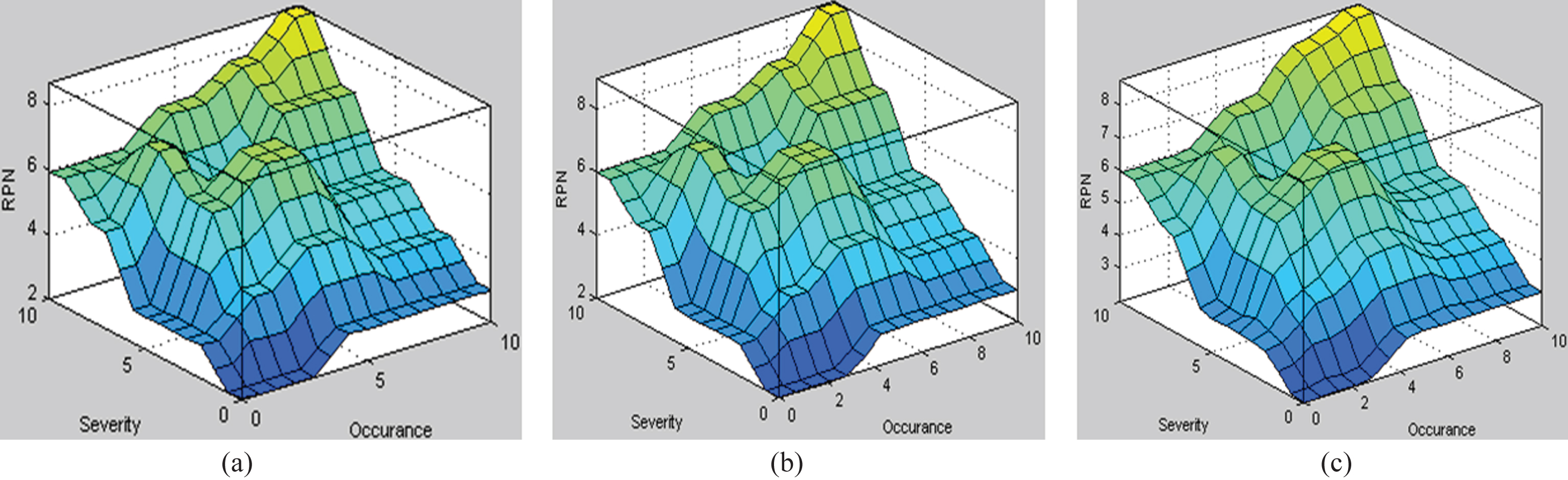
Spectrum of Surface graph for RPN calculation with (a) trimf; (b) trapmf; and (c) gaussmf.
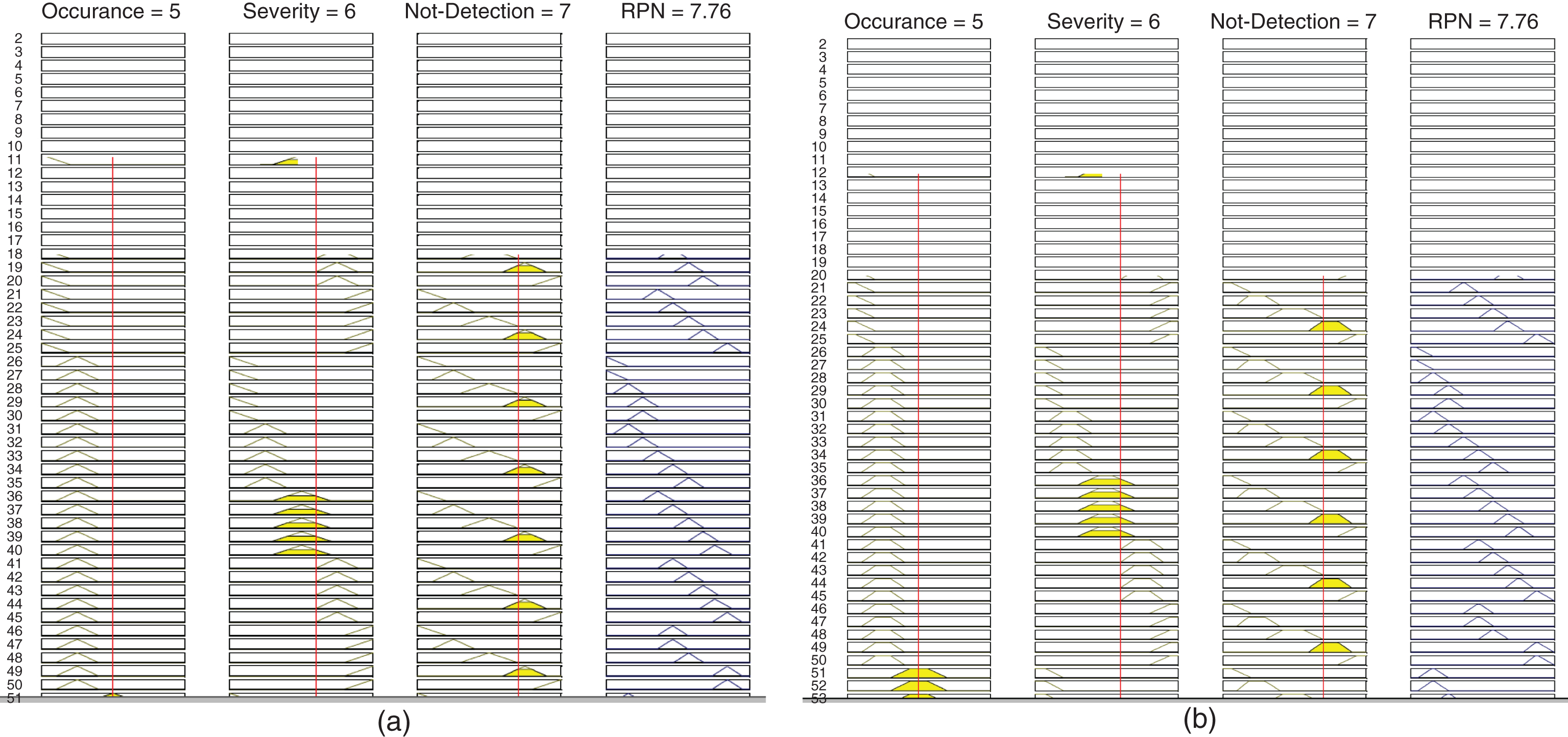
Spectrum of Rule Viewer for RPN calculation with (a) trimf; and (b) trapmf.
Knowledge based RPN evaluation in PPH becomes important because of its simplicity, but requires skills. Most of the time, this involves an immense evaluation of S, O, D and compares the results of different methods. This section describes the three distinct NN based methods for RPN evaluation. RPN evaluation is non-linear mapping of input and outputs. Back propagation based artificial neural network (BPNN), Radial Basis Function (RBF) and Generalized Regression Neural Network are used to evaluate the RPN to calculate the RPN level in PPH in its initial stage.
Basic concepts of propagation neural network
A three layer BPNN includes several neurons that are connected with each other through connecting weight (W) [10–17].
Figure 11 represents the structure of BPNN [15]. The total count of neurons in input and output layers depend on the functional problem, whereas the count of neurons in the hidden layer is random and is determined by trial-and-error [10]. BPNN architect.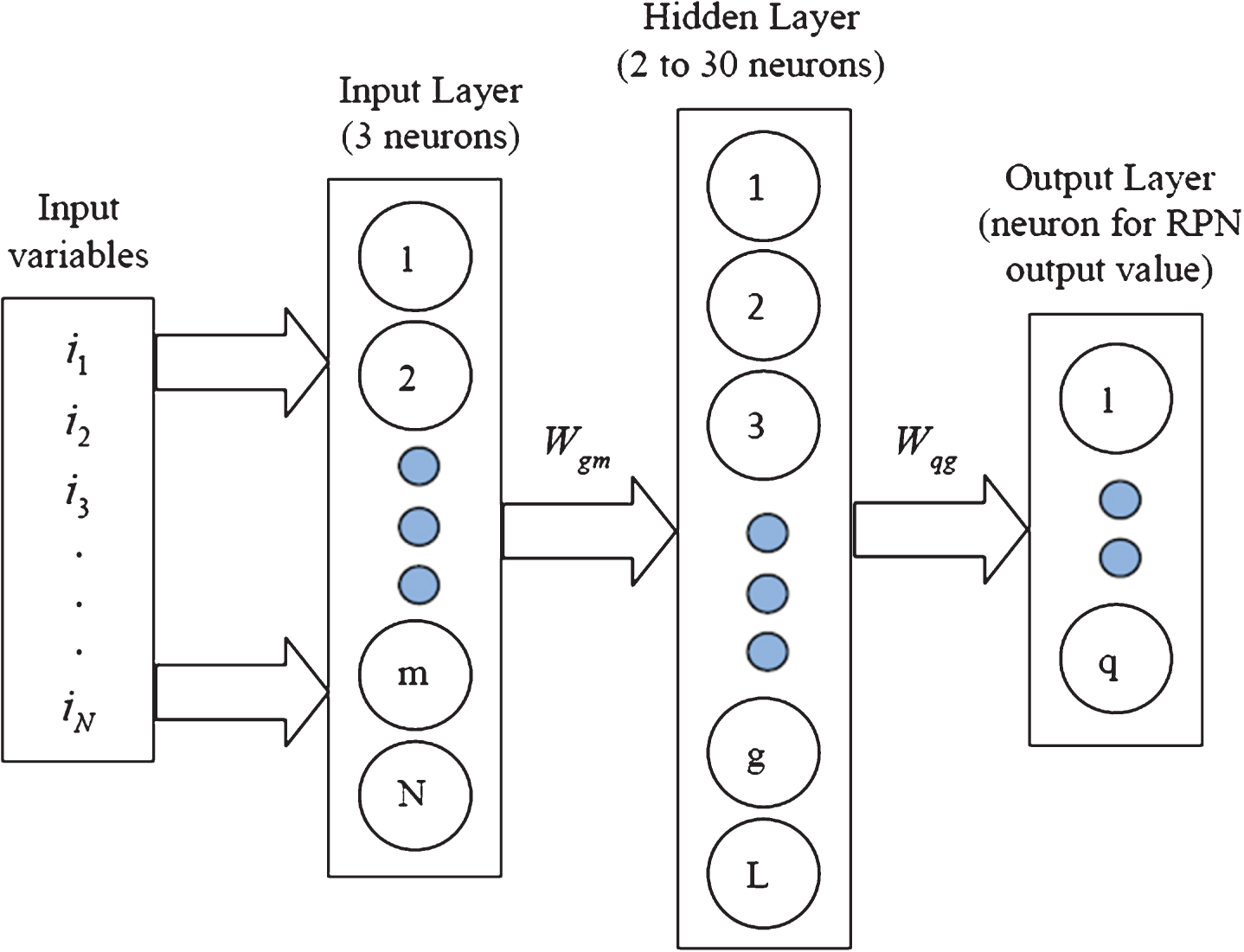
The output for every single neuron of hidden layer is computed by Equation (2):
Where, i m = m th input for net; i N · w mg = weight value of input neuron m to hidden neuron g; θ g = bias of the g th hidden neuron and f (·)= activation function of the neuron.
The output for each neuron in the output layer is calculated by using equation number (3):
Where, O q = q th output of the net; w qg = weight of the connection from hidden neuron to output neuron q; θ q = bias of the q th output neuron and f2 (·)= activation function of the neurons.
Figure 3 (proposed approach) represents BPNN design process. The corresponding essentials of the networks are also determined in the process.
A BPNN includes choice of inputs, outputs, network topology and weighed connecting node. O, S and D are chosen as inputs. Ten output nodes representing different RPN value such as N, VL, L, HL, LM, M, HM, LH, H and VH condition are considered.
In this case, the optimal network parameters for BPNN are chosen by using hidden and trial method. Network parameters are: gradient = 9.9512e-006, Mu = 0.0001, at epoch 53, learning rate = 0.024; momentum factor = 0.79; no of hidden layer neurons = 21; tolerance = 0.0009.
BPNN based Graphical results for RPN values estimation by using Matlab are represented in Figs. 12-13. (a) Error Histogram, (b) Training State, (c) Performance graph based on Mean Square Error (mse) algorithm, (d) Fit plot.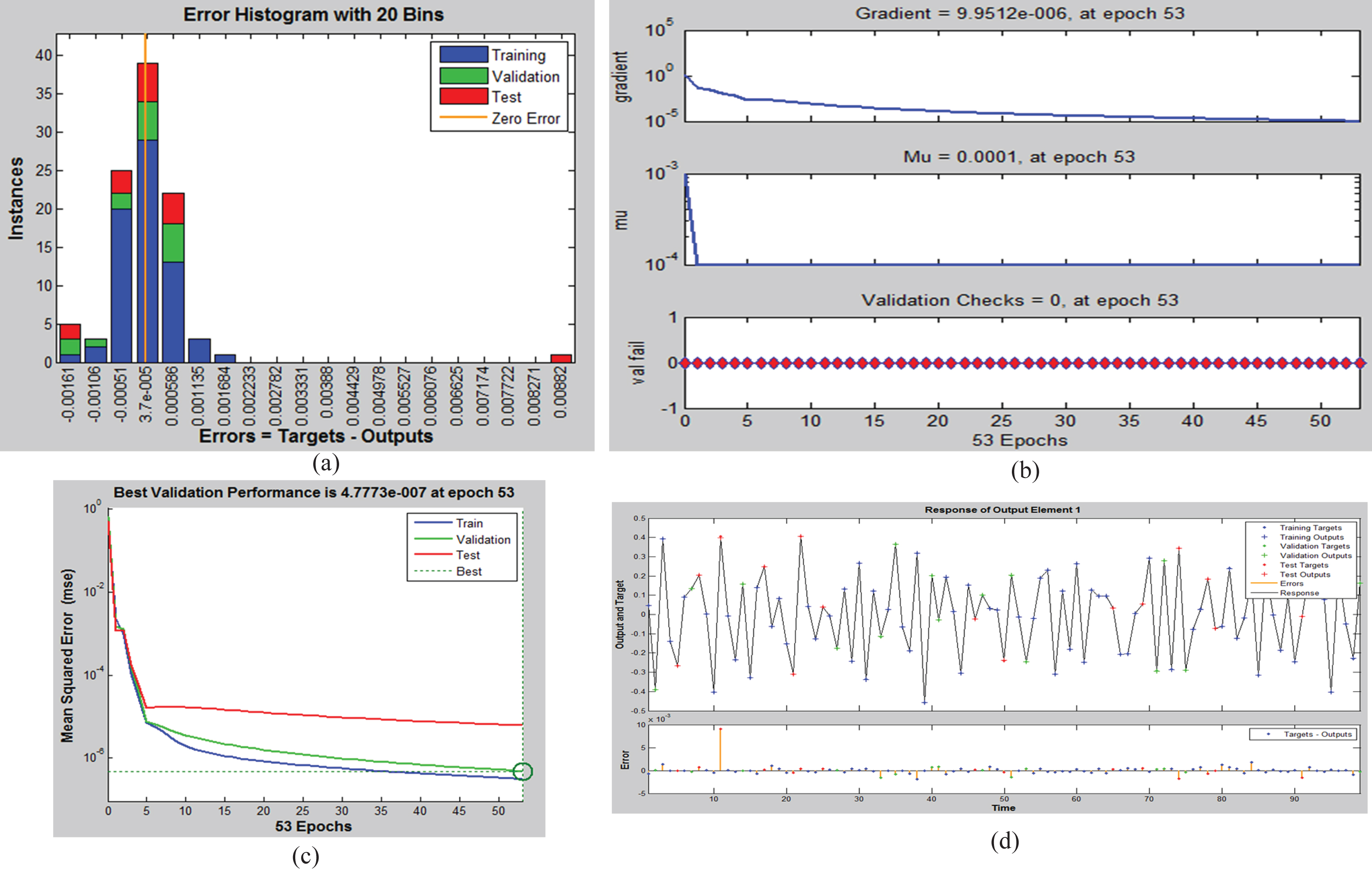
Error plot is shown in Fig. 12(a), which represents the additional validation of the model which shows the train, test and validation phase error magnitude. Performance plot shows the validation error which includes training errors, validation errors, and test errors as represented in Fig. 12(c). Plot fit and regression plots are represented in Figs. 12(d) and 13(a-d) respectively, overall regression is 0.99999, very nearer to unity. Prediction of RPN during (a) training phase, (b) test phase, (c) validation phase, (d) over all Regression plot.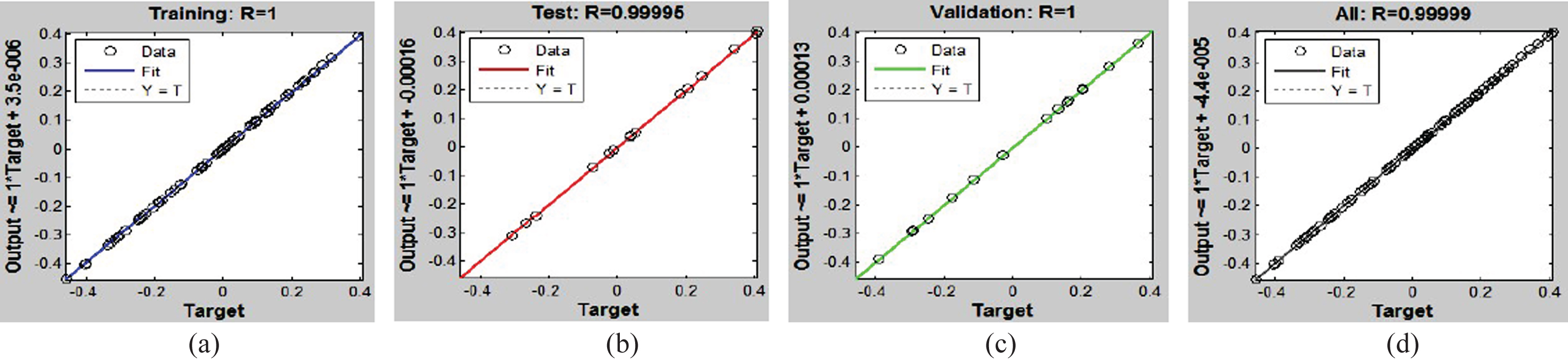
The utilization of RBF is function approximation, classification, time series prediction which is formulated first in 1988 by two researchers (Lowe and Broomhead). RBF network generally utilized for activation function in ANN and output is linear combination of RB functions of inputs and neuron’s parameters. The mathematical architect of RBF NN is given below:
Where, N = no. of hidden layer neuron, c
k
= center vector of kth neuron, α
k
= weight of kth output linear neuron. RBF is generally used Gaussian as:
The α
k
, c
k
and β
k
parameters are optimized and found as per fit between out put RBF Based R Representation of RPN Calculation for (a) Training phase and (b) Testing Phase.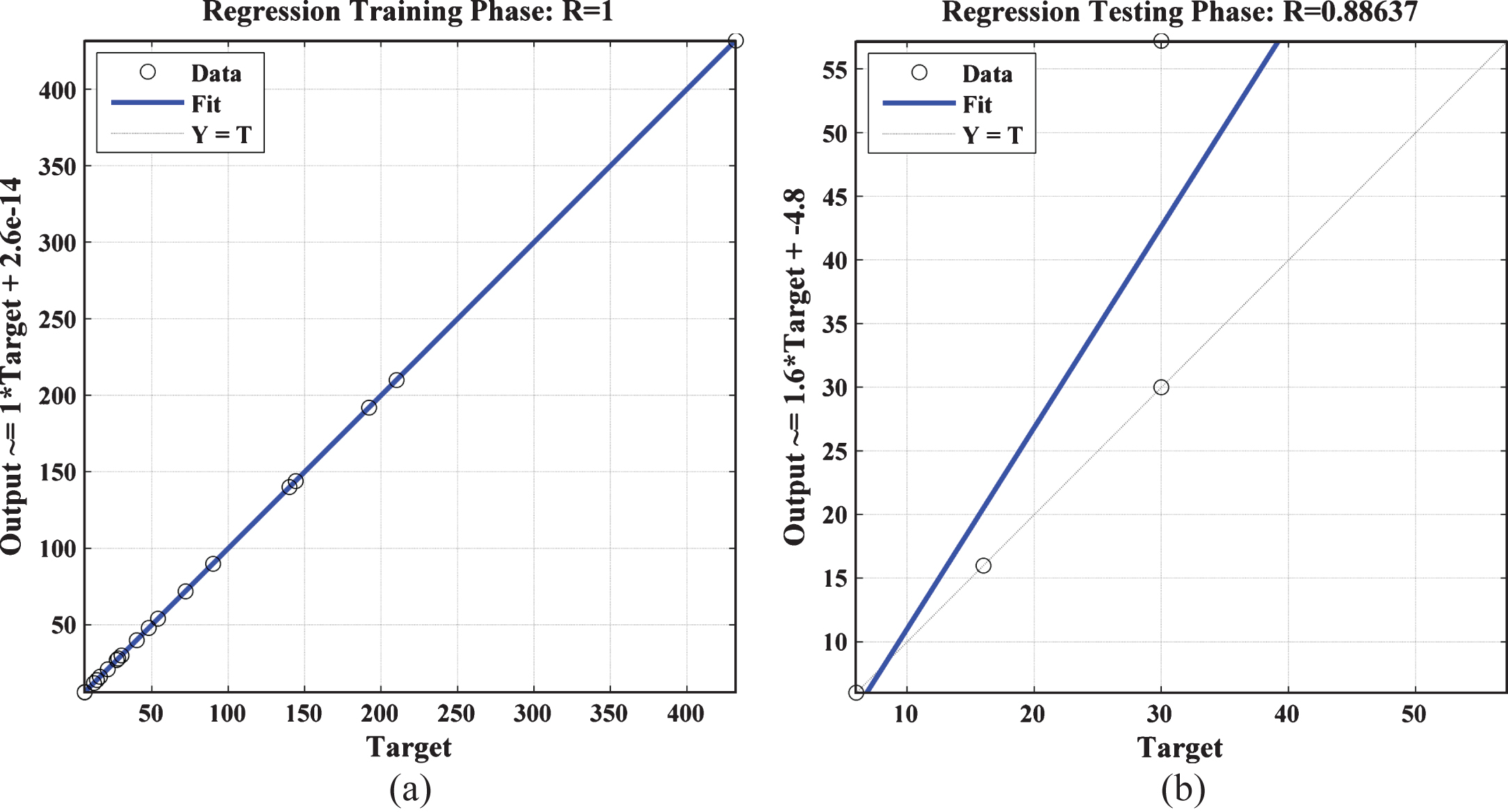
GRNN is a variant of radial basis NN which was introduced in 1991 by D.F. Specht. GRNN is applicable for classification and prediction other than regression. GRNN is advanced approach in NN based on non-parametric regression and each training specimen presents a average of radial basis neuron. Mathematically GRNN is representedby [12]:
Where, Z (y)= prediction value of y, z k = activation weight of pattern layer neuron k, and K (y, y k )= Gaussian (radial basis function) kernel.
Gaussian Kernel, K (y, y k ) = e-d k /-2σ2
where, d k = squared euclidean distance between input (y) and training sample (y k ) and d k = (y - y k ) T (y - y k ).
The Matlab coding based regression plot for training and testing phase are represented in Fig. 15 which shows testing results better as compared with RBF and BPNN. GRNN Based R Representation of RPN Calculation for (a) Training phase and (b) Testing Phase. Fuzzy-Logic Based Degree of MFs for RPN Calculation Neuro-Fuzzy Scheme Based Result Comparison of Various Samples for Prioritization of failure modes P = Prioritization; MF = Membership function actual condition RPN = ANN Based RPN. Recommendation for failure number as per prioritization of failure mode By using the Neuro-Fuzzy scheme, 28 number of failure conditions during purchasing process were calculated as per the value of three factors (O, S and D) of FMEA and results are shown in Table 5. Here, RPN values are calculated by selecting the highest membership value achieved by fuzzy rules and by MSE in BPNN. The prioritization number of failure mode is assigned into the variable depended on the degree of MF as represented in Table 4. It can be seen from failure mode numbers 1, 2, 4, 6, 18 and 28 that proposed scheme is relation with conventional FMEA approach for prioritization number assignment of RPN value. Compared with conventional FMEA method, the proposed scheme has few advantages i.e., due to same value of RPN of the events, misuse of resources, waste of time or in few cases event with high risk is unnoticed by FMEA approach but can be concluded by proposed scheme (shown in Table 5). The risk implication can be completely different for same value of RPN as shown in failure number 5 and 8 where RPN value is same with different risk implication. Few recommendations are proposed by the study given in Table 6. Conventional FMEA calculates RPN by multiplying factor scores achieved from the probability or degree of problem occurrence by considering the relative impact of all factors. Here, Neuro-Fuzzy scheme eliminates the conversion method by evaluating the linguistic assessment of factor for calculating RPN by putting relative weighing coefficient. By applying neuro-fuzzy scheme for the PPH equipment, different counteractive methods are recommended. 20 out of 28 failures, few suggestions were made and for 8 failures no suggestion was advised. With the implementation of all methods, it is about to get a decrease of 15% of time spent and 20% in lead time. Proposed Neuro-Fuzzy application can solve the problems that have raised by using conventional FMEA approach and can detect the causes of failure modes and effects. Proposed approach may furnish the stability and constancy services in hospital. It is the first study of neuro-fuzzy based for the hospital management for purchasing process.
Conclusion
References