
Abstract
Ultrasound image quality management and assessment are an important stage in clinical diagnosis. This operation is often carried out manually, which has several issues, including reliance on the operator’s experience, lengthy labor, and considerable intra-observer variance. As a result, automatic quality evaluation of Ultrasound images is particularly desirable in medical applications. This research work plans to perform the fetal heart chamber segmentation and classification using the novel intelligent technology named as hybrid optimization algorithm Tunicate Swarm-based Grey Wolf Algorithm (TS-GWA). Initially, the US fetal images data is collected and data undergoes the preprocessing using the total variation technique. From the preprocessed images, the optimal features are extracted using the TF-IDF approach. Then, Segmentation is processed on optimally selected features using Spatially Regularized Discriminative Correlation Filters (SRDCF) method. In the final step, the classification of fetal images is done using the Modified Long Short-Term Memory (MLSTM) Network. The fitness function behind the optimal feature selection as well as the hidden neuron optimization of MLSTM is the maximization of PSNR and minimization of MSE. The PSNR value is improved from 3.1 to 9.8 in the proposed method and accuracy of the proposed classification algorithm is improved from 1.9 to 12.13 compared to other existing techniques. The generalization ability and the adaptability of proposed TS-GWA method are described by conducting the various performance analysis. Extensive performance result shows that proposed intelligent techniques performs better than the existing segmentation methods.
Keywords
Introduction
Fetal heart defect (FHD) is a abnormalities with a baby’s heart that arise while the infant is still growing. It is a major frequent and dangerous birth abnormalities in the present situation [1, 2]. Asia has the greatest rate of FHD birth defects, with 9.3%. (95 percent CI: 8.9-9.7). FHD has the highest incidence and fatality in China for the previous 12 years, and it is the leading cause of children death [3]. Despite substantial breakthroughs in diagnosis and care, FHD is still the leading cause of mortality in newborns during their first year. To reduce birth malformations and death, efficient prevention method and control techniques are required [4]. An efficient tool for identifying foetal cardiac abnormality is still foetal echocardiography. Standard foetal heart US slices are still challenging to obtain since the foetal position inside the mother fluctuates [5]. An echocardiogram is a comprehensive US test of the baby’s heart performed before the delivery. As a consequence of the pathophysiological variations in the foetal heart at distinct stages of pregnancy, the two-dimensional structure and hemodynamics of the foetal heart are constantly varying, necessitating practitioners with substantial knowledge in development and disease cognition. Hence, The evaluation is performed by hand, which is labor-intensive and time-consuming, and so may be clinically ineffective [6]. It is challenging for radiologists, particularly inexperienced sonographers, to perform an adequate US sweep for complicated structures like the embryonic heart in clinical practice.
Furthermore, competent radiologists are still in low supply in poor areas. As a result, there exists a great demand for a completely automated quality control system for foetal US images [7]. We should first develop a quantitative quality control methodology for the target planes in great detail. One or multiple networks are used to attain quantitative evaluation of the protocol’s elements on the basis of the protocol [8]. Generally, all US planes’ procedures (e.g., cranial, cardiac, and abdominal views) should include the following three portions. To begin, we must establish whether a scanned image is the target plane (for example, foetal Cardiac Four-chamber Plane (CFP). If that’s the case, we’ll go on to the target plane’s next step [9]. Few significant characteristics of US imaging, including as gain and zoom, as well as numerous key anatomical features on the target plane, should be considered further on the basis of the preceding phase. Gain and zoom have typically been disregarded in prior investigations [10].
The Convolutional Neural Networks (CNN) has been frequently utilized to evaluate medical images since the invention of deep learning. Generative adversarial network (GAN) describes a new unsupervised form of learning network that was recently suggested [11]. It’s a form of neural network method where two networks are trained at the same time, one for image production and the other for discriminating. It enables the learning of deep representations without the need for significant labeled training material. Owing to their tolerance to overfitting as well as capability to capture data distributions, GANs have attracted interest in both business and academics, making image generating jobs easier [12].
FHD images during the end-systolic stage are complex to collect, and training a stable method from foetal FCH images is more challenging than training a stable method from adult FHD images [13], there has been little study on detecting FHD utilizing deep learning. The images of a foetus and an adult have two major variances. The initial is that various foetal placements inside the mother’s body make it harder to register. The other is that depending on the gestational week, the form of the FCH images varies dramatically. As a result, reliably training a network to identify FHD is tough. According to recent research, the identification rate of FHD ranges from 65 percent to 81 percent. Inadequate data of foetal FHD images, on the other hand, may diminish the model’s robustness and lead to overfitting; indeed, this training is difficult for most of the large networks suggested in the computer vision area [14]. Overfitting may be addressed and accuracy increased by using transfer learning, a training strategy that integrates and transfers information between various tasks. Deep learning has already been shown to be beneficial for transfer learning tasks since the features learnt by Deep Neural Networks (DNN)s capture the majority of the important information needed for categorization [15]. Yet, owing to large distribution mismatches among the target (medical images) and source (natural images) domains, traditional transfer learning can decrease classification results in the medical image domain. Furthermore, video slices are used to boost the robustness of transfer learning, although accuracy ratings are rarely published.
The main contribution of this paper are. Fetal heart chamber segmentation and classification process using the novel intelligent technology. To accomplish the optimal feature selection, where the features are tuned with an objective concept. To perform the classification by MLSTM, network, where the hidden neurons of LSTM are tuned with the consideration of PSNR maximization and MSE minimization. To propose a novel form of optimization algorithm called TS-GWA for enhancing the optimal feature selection and the classification phases of the introduced fetal heart chamber segmentation and classification and to compare the developed method with existing algorithms
The rest of the article describes as follows, Section 2 describes the fatal image segmentation related work and its feature. The proposed model and pre-processing for the fetal heart chamber segmentation and is presented in Section 3. Section 4 describes the feature extraction and segmentation of fetal heart chamber. Optimization process and MLSTM network for the fetal heart chamber classification is elaborated in Section 5. The detailed performance analysis is presented in Section 6. Section 7 concludes this research work.
Related works
In this section, we present related work of Fetal Heart Chamber Segmentation and Classification. Also this section describes the various research methods adopted for US fetal segmentation.
Chen et al. [16] suggested a novel method called DGACNN that performed best in identifying FHD, with an accuracy rate of 85 percent. The goal of this network to address the issue of inadequate training datasets for building a strong model. There were numerous unlabeled video slices, but annotating them was difficult and time-consuming. As a result, understanding how to employ these un-annotated video slices to increase the DGACNN capabilities for detecting FHD with respect to both robustness and recognition accuracy was crucial for FHD screening. The DGACNN surpassed various existing networks by 1 percent to 20% in identifying FHD, according to the testing. A comparative experiment demonstrated that this network already surpasses professional cardiologists in detecting FHD, with an accuracy rate of 84 percent in one test. As a result, the suggested design has a strong chance of assisting cardiologists in completing early FHD tests.
Yagel et al. [17] have developed a general deep learning architecture for foetal US CFP quality control. The suggested framework was composed of three networks: (1) a basic CNN (B-CNN), which roughly classified four-chamber views from raw data; (2) a Deeper CNN (D-CNN), which determined the gain as well as zoom of the target images using multi-task learning; and (3) the ARVBNet, which detected the key anatomical structures on a plane.
Del Bianco et al. [18] have suggested a general framework on the basis of instance segmentation for precisely and concurrently segmenting the four heart chambers. Experimental findings demonstrated that the technique could obtain higher segmentation performance vs conventional techniques in the gathered dataset, which comprised echocardiogram images having four-chamber views of 319 foetuses. The model obtained Dice coefficients of 0.7956, 0.7619, 0.8199, and 0.7470 for the four cardiac chambers, having an average precision of 45.64 percent, utilizing fivefold cross-validation.
Rahmatullah et al. [19] have included an element for extracting ROI on the basis of target detection, and determined the four-chamber view in order to improve classification performance. However, the merged neighbor frame difference into image channels not lose the time dependency. To increase diagnostic accuracy, researchers have devised a simple yet efficient RLDS for identifying embryonic CHD that used CNNs to extract discriminative aspects of the foetal cardiac anatomical structures [20]. Extensive testing has shown that the suggested RLDS was quite successful in detecting foetal CHD. Moreover, in the test set, the suggested RLDS attained an accuracy of 93% and a recall of 93%, considerably improving the prenatal detection rate for foetal CHD.
The separation of the four heart chambers in foetal echocardiograms using a unique group subspace approach is presented in [21]. The method was able to leverage the intrinsic structure of echocardiograms by merging the group reconstruction error, sparsity, and distinguishing term into a cohesive framework, resulting in the production of a discriminative group dictionary. To create a small dictionary having high atom usage and minimal complexity, a unique adaptive group dictionary learning technique was devised. The reconstruction residue was used to distinguish the starting position of four chambers using the learnt dictionary. The final outlines were refined regionally using the local appearances. Extensive testing was done to assess the performance of the developed AGDL and its use in foetal echocardiography segmentation. The findings showed that the technique has superior representation as well as discriminative power than other competitive traditional sparse representation approaches and general intensity methods. The method could learn a more concise and discriminative group vocabulary, resulting in more reliable and appropriate four-chamber segmentation outcomes.
Verdurmen et al. [22] have developed a system for keeping track of the main factors that characterize the content of every frame of freehand 2D US scanning movies of a healthy foetal heart. This was a critical initial step in developing tools to aid in the identification of CHD in unusual situations. The visibility, position, orientation of the foetal heart in the image, and the observing plane label from every frame, were predicted using regression and classification forests. Author also created a new regression forest adaption for circular variables to cope with cardiac phase forecasting. Chen et al. reported findings from a difficult dataset collected in a real-world clinical context and compared them to expert annotations, reaching equal levels of accuracy to inter- as well as intra-observer variance. The Aplio i800 (CANON Medical Systems Corporation, Tochigi, Japan) and a convex probe (4 MHz) for foetuses were used for the entire recordings [23].
An end-to-end DW-Net presented in [24] for precise segmentation of seven major anatomical components. The ssuggested DW-Net might help further extract valuable clinical indicators in early FE and enhanced the prenatal diagnosis effectiveness and accuracy of CHDs by accurately and automatically segmenting the A4 C image. Traditional segmentation and classification procedures for the entire foetus, as well as the foetal brain, brain, lungs, heart, liver, and placenta in MRI and three-dimensional US have been addressed [25]. Potential clinical uses of the aforesaid technologies were also investigated.
Proposed model for the fetal heart chamber segmentation and classification
Proposed model
The proposed fetal heart chamber segmentation and classification frameworks contain the following phases data collection, pre-processing, feature extraction, optimal feature selection, segmentation, classification.
In the data collection phase, the data is collected from the US fetal images. This undergoes the pre-processing phase using the total variation technique. Next, the features are extracted in the feature extraction phase using the TF-IDF approach. Since the length of the extracted features seems to be long, it is necessary to select the optimal features using proposed TS-GWA. Further, the segmentation is accomplished using the SRDCF technique. Finally, the classification is done by LSTM, where the hidden neurons are tuned by same TS-GWA with the intention of PSNR maximization and MSE minimization thus referred as MLSTM. This MLSTM classifies the final fetal heart chamber output. The architecture of the developed fetal heart chamber segmentation and classification framework is shown in Fig. 1.

Proposed architectural model of fetal heart chamber segmentation and classification.
Sample pre-processed images of fetal heart chamber segmentation is presented in Fig. 2. The pre-processing is done to remove the noises present in the gathered data. Here, the pre-processing is performed by the total variation technique. Total variation [26] regularisation is a term used in signal processing to describe total variation denoising. This method is most commonly utilized in digital image processing to remove noise. It is based on the idea that signals having a lot of unnecessary and possibly erroneous features have a lot of overall variance because the integral of the signal’s absolute gradient is large. Minimizing the signal’s overall variance achieves a tight match to the original signal and eliminates extra detail while maintaining important characteristics like edges. This noise reduction approach offers advantages over basic approaches like median filtering, which decrease noise as well as smooth edges to a lesser or greater extent at the similar time. Therefore, even at low SNRs, total variation denoising is extremely effective at retaining edges while smoothing out noise in flat regions. Thus,
The noise model is represented by the Equation (1), in which z is the actual image and y is the observed image having noise o. Finding the signal y while reducing the objective function defined in the Equation (2)
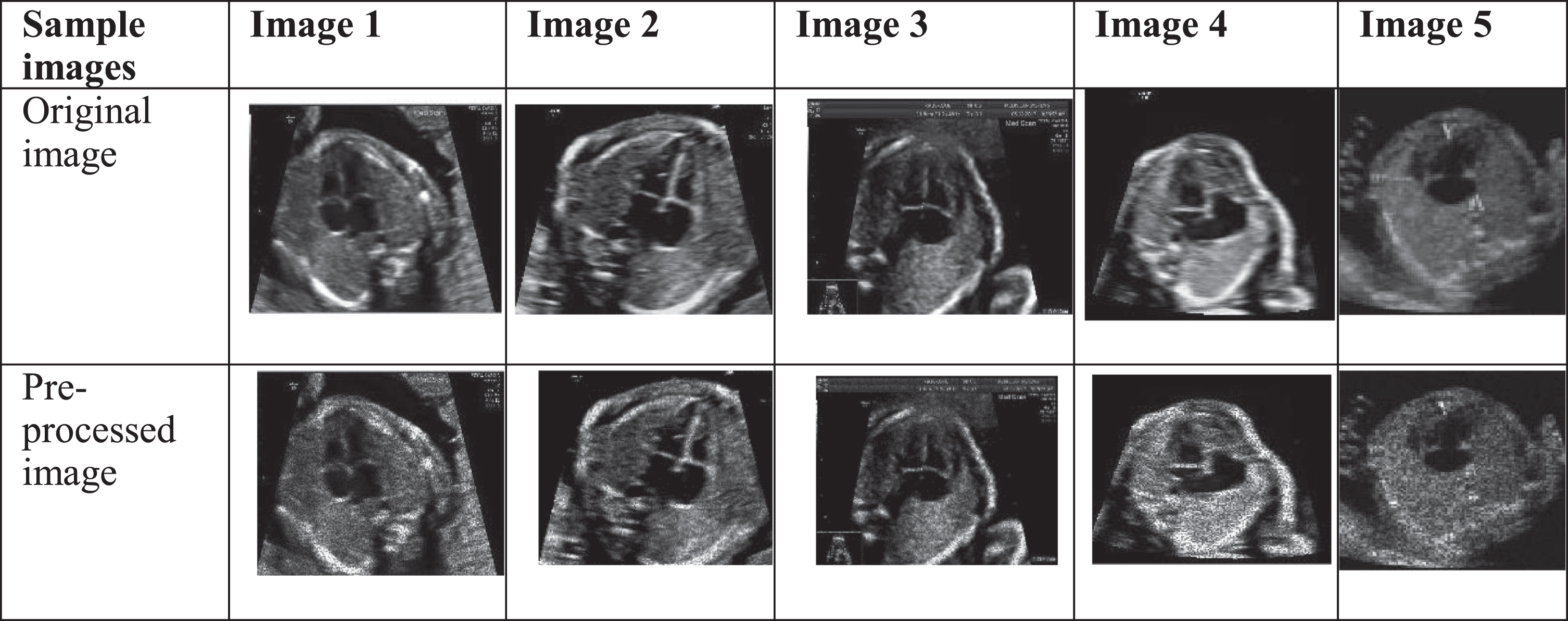
Sample pre-processed images of fetal heart chamber segmentation and classification.
The objective function is minimized by control the regularisation parameter λ which also limits the amount of smoothing that may be done in the pre-processing stage.
Feature extraction
The feature extraction supports in minimizing the redundant data count from the provided pre-processed dataset. It enhances the learning speed as well as the generalization steps. Here, the feature extraction is accomplished using the Term Frequency –Inverse Document Frequency (TF-IDF) technique [27].
In the TF-IDF feature extraction techniques, Fetal pre-processed image dataset is converted into raw vectors. Then each raw vectors are assessed through the cosine similarity measures. Since, we are using fatal images for feature extraction process, so that the value of TF-IDF is closely monitored. The value of TF-IDF value increases in certain region, that region is closely observed and that region converted into image set. From this feature extraction techniques, fine details related the fetal images are observed for further process.
Optimal feature selection
The fine features of fatal images are obtained from the previous step. This optimal feature selection process cuts the number of wrong features in half while keeping real positive rates the same. This implies it is more practical in selecting the appropriate variables, leading in a system that is simpler, more understandable, and more realistic. Since the extracted features seems to be lengthy, it is necessary to select the significant features in order to reduce the complexity. This is done by the introduced TS-GWA, where the features are being tuned. When creating forecasting models, it represents the method of minimising the count of input variables. The count of input variables should be reduced to lower the computational cost of modelling and, under certain situations, to increase the effectiveness of the algorithm. Removing extraneous data increases learning accuracy, decreases computation time, and makes the adaptive learning or data easier to grasp.
Segmentation
The segmentation signal divides a signal into many epochs having similar statistical features, like amplitude as well as frequency. Here, the segmentation is done using Spatially Regularized Discriminative Correlation Filters (SRDCF) approach. Because of the online aspect of the tracking issue, DCF-oriented trackers are becoming increasingly familiar in the tracking community owing to their high effectiveness, simplicity, and reliability. Color-Name [29], HOG [30], and deep features [31, 32] are examples of novel features that have been extensively employed; feature incorporation has also been employed [33]. Part-oriented trackers [34] are extensively used to alleviate occlusion. On the basis of the periodic presumption of the training instances, the entire correlation filter-oriented trackers employ FFT to considerably minimise the training as well as detection processing work. The periodic assumption, on the other hand, resulted in undesirable boundary consequences.
The SRDCF [28] formulized in the spatial domain is initially translated to the Fourier domain to obtain a complex equation, which is then converted to a real-valued equation and solved using the Gauss-Seidel technique. The results of the Gauss-Seidel technique must be altered again in order to obtain the correlation filters we want. When they obtain the complex equation, they divide it into real as well as imaginary parts, rebuild the issue as a real-valued equation, and then devise a simplified inverse approach to obtain a closed-form response; nevertheless, the simplified inverse operation has a high computational complexity. Transitions from spatial to Fourier or from complex to real-valued equations are seamless, and correlation filters are calculated immediately.
A collection of training instances
Here, α
l
⩾ 0 represents the weight of each training sample y
l
, spatial regularisation is provided by ω, which shows a Gaussian shaped function having smaller values in the centre region and larger values in the marginal area, and ⊙ symbolises element wise multiplication. The convolution function equals to the T
g
(y
l
) which is given by Equation (4)
The SRDCF uses the same detecting technology as ordinary DCF-oriented trackers. The object tracking represented in the Equation (5).The SRDCF uses a scaling pool to manage target scale variations during the detection stage, and the Fast Sub-grid approach to improve the detection findings.
Proposed TS-GWA
The proposed TS-GWA is used for enhancing the optimal feature selection and the classification phases of the fetal heart chamber. It optimizes the features in optimal feature selection phase as well as hidden neurons of LSTM with the intention of PSNR maximization and MSE minimization. The Grey Wolf Optimization (GWO) [35] is modelled after the natural leadership structure and hunting operation of grey wolves. For emulating the leadership structure, four sorts of grey wolves are used: beta, alpha, delta, and omega. Furthermore, the three basic processes of hunting are installed: seeking for prey, encircling prey, and attacking prey.
The GWO has several advantages such as better convergence, local optima avoidance, exploitation, and exploration. It also has superior performance in challenging, unknown search spaces. But, it cannot solve the binary as well as the multi objective versions. Thus, to overcome this drawback, Tunicate Swarm Algorithm (TSA) [36] is integrated into it and the resulting algorithm is called as TS-GWA. This TS-GWA can handle the binary as well as the multi objective optimization problems.
In the navigation as well as the foraging phase, the suggested algorithm mimics tunicate jet propulsion and swarm behaviours. Tunicate includes the capacity to locate a food source in the water. Unfortunately, in the supplied search space, there exists no information regarding the food source. Two tunicate behaviours are used to select the best food source, i.e., optimal. Jet propulsion and swarm intelligence are two of these traits. A tunicate must satisfy three standards in order to statistically describe jet propulsion behaviour: prevent conflicts among search agents, move in the path of the best search agent’s location, and stay near to the optimal search agent. The swarm activity, on the other hand, will keep remaining search agents up to date on the best optimum answer.
The TS-GWA works on the basis of fitness. If fit ⩽ 0.5, then the update takes place using GWO which is represented in the Equations (6)–(10).
In these Equations (6)-(10), the components of
Otherwise, if fit > 0.5, then the update takes place by TSA as in Equation (11) –Equation (12).
Here, Start Initialization of population Initialization of parameter Calculation of fitness
else
Repeat till maximum iterations Compute best fitness Return best solution Stop
The proposed MLSTM is used for enhancing the classification phase of the developed fetal heart chamber classification model, by optimizing the hidden neurons of LSTM by TS-GWA with the consideration of PSNR maximization and MSE minimization. Hochreiter and Schmidhuber [38] created LSTM [37], a development of RNN, to overcome the RNN shortcomings by including more interactions per module (or cell). LSTMs are a type of RNN that, by default, can learn long-term dependencies and recall information for lengthy periods of time. The LSTM is structured in a chain format, according to Olah [39]. The recurring module, on the other hand, contains a distinct structure. It features four interacting layers having a unique form of communication, rather than a single NN like a normal RNN.
The initial stage in building an LSTM network is to recognize information that not needed and will be left out of the cell. The sigmoid function, which considers the output of the final LSTM unit (iu-1) at time u - 1 and the present input (Y
u
) at time u, determines the procedure of detecting and excluding data. The sigmoid function also decides whether parts of the old output should be removed. The forget gate g
u
defined in Equation (13), describes a gate in which g
u
shows a vector having values ranging from 0 to 1 that corresponds to every count in the cell state, Du-1.
Here, σ shows the sigmoid function, and X
g
and c
g
describes the forget gate’s weight matrices and bias, accordingly. The decision and storage of information from the new input (Y
u
) in the cell state, as well as updating the cell state, are the next steps. The sigmoid layer and the tanh layer are the two sections of this stage. The sigmoid layer determines whether new information must be adjusted or discarded (0 or 1), and the tanh function assigns weight to the values that pass through, determining their relevance (1 to 1). To update the new cell state, the two values are multiplied. The old memory Du-1 is then joined to the new memory, producing in D
u
which is defined in Equation (14).
Du-1 and D
u
describes the cell states at time u - 1 and u, correspondingly, whereas X and c shows the cell state’s weight matrices and bias, accordingly. The output values (i
u
) defined in Equation (17) in the last step are filtered versions of the output cell state (P
u
) expressed in Equation (18). A sigmoid layer is used to determine whether aspects of the cell state find it to the output. The sigmoid gate output (P
u
) is then multiplied using the new values produced by the tanh layer from the cell state (D
u
), having a value ranging from -1 to 1.
The structure of MLSTM for fetal heart chamber classification is shown in Fig. 3.

MLSTM for fetal heart chamber classification.
The major objective of introduced TS-GWA-based fetal heart chamber segmentation and classification is to optimize the features of optimal feature selection phase as well as hidden neurons of LSTM with the intention of PSNR maximization and MSE minimization. The objective function is modelled as in Equation (19).
In the above Equation (19), the features to be optimized are shown by Ft, hidden neurons of LSTM are shown by HN
LSTM
, and the fitness is shown by fit respectively. PSNR and MSE is expressed in Equations (20) and (21) Respectively.
Fetal heart US images
The images of the second trimester foetal cardiac US utilised in this study came from Mediscan systems, a facility for US, prenatal care, and genetics in Chennai, India, as well as internet data. The foetal cardiac images are more visible in the second trimester than in the first trimester. since the growth of the cardiac system of the foetus occurs in the second trimester. Hence, only second trimester foetal cardiac images are considered in this research work. There are 50 normal foetal cardiac US images in the database, 18 abnormal images with AVSD, 18 abnormal images with VSD, and 14 abnormal Ebsteins images. The images were taken with a GE Healthcare Voluson E8 US machine having a 51 Hz linear transducer. The images attained were 800 x 600 pixels in size. Before filtering, all of the images were shrunk to 512 x 512 pixels. This study also used 25 normal foetal heart images from the internet. Figure 4. Shows the normal foetal heart images considered for this work. The following Performance and Error Measures given in Equations (22) to (24) are used in this work to evaluate the effectiveness of proposed intelligent technique.

Sample US Fetal Images associated with various datasets.
The MSE analysis of various heuristic-based algorithms for the fetal heart chamber segmentation and classification is shown in Fig. 5. It is clearly understood that the MSE error measure of TS-GWA is lower than the other methods, thereby revealing its superiority. The MSE of TS-GWA is 0.81%, 1.43%, 2.31%, and 0.96% higher than PSO, GOA, TSA, and GWO.
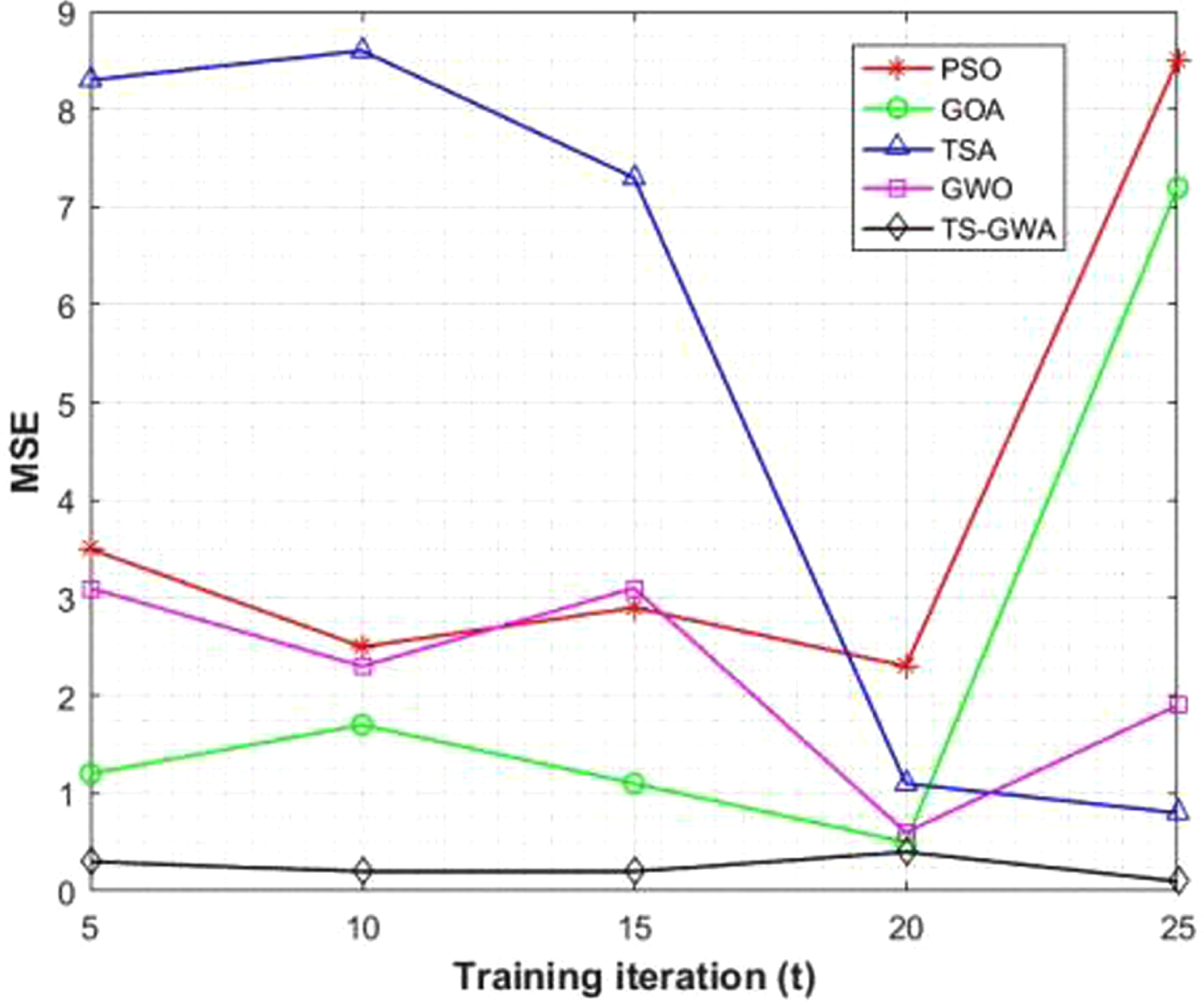
MSE Analysis of different heuristic-based methods for the fetal heart chamber segmentation and classification.
The PSNR analysis of several heuristic-based algorithms for the segmentation and classification of foetal heart chambers is shown in Fig. 6. The PSNR error measure of TS-GWA is clearly lower than that of the other approaches, demonstrating its superiority. PSO, GOA, TSA, and GWO have PSNRs of 3.21 percent, 2.31 percent, 1.89 percent, and 0.80 percent, respectively. As a result, it can be deduced that the presented TS-GWA has a higher PSNR value, demonstrating its superiority in foetal heart chamber segmentation and classification.

PSNR Analysis of different heuristic-based methods for the fetal heart chamber segmentation and classification.
Figure 7 shows the RMSE analysis of multiple heuristic-based techniques for segmenting and classifying foetal cardiac chambers. TS-GWA’s RMSE error metric is significantly lower than the other techniques, proving its superiority. RMSE s of 1.82 percent, 2.76 percent, 1.52 percent, and 2.15 percent are found in PSO, GOA, TSA, and GWO, respectively. As a consequence, the provided TS-GWA has a better RMSE value, confirming its superiority in the segmentation and categorization of foetal heart chambers.

RSME Analysis of different heuristic-based methods for the fetal heart chamber segmentation and classification.
The MAE analysis of different heuristic-oriented approaches for segmenting and classifying foetal cardiac chambers is depicted in the Fig. 8. The MAE error statistic of TS-GWA is substantially lower than the others, demonstrating its superiority. PSO, GOA, TSA, and GWO had RMSEs of 2.53 percent, 3.01 percent, 1.15 percent, and 2.03 percent, correspondingly. As a result, the offered TS-GWA has a lower MAE, indicating that it is superior at segmenting and classifying foetal heart chambers.

MAE Analysis of different heuristic-based methods for the fetal heart chamber segmentation and classification.
Figure 9 shows the accuracy analysis of several heuristic-oriented techniques for segmenting and classifying foetal cardiac chambers. TS-GWA has a significantly higher accuracy than the others, proving its superiority. The accuracies for PSO, GOA, TSA, and GWO, respectively, were 1.99 percent, 3.14 percent, 5.61 percent, and 4.98 percent. As a result, the TS-GWA that is being supplied has a higher accuracy, indicating that it is better at segmenting and classifying foetal heart chambers.

Accuracy Analysis of different heuristic-based methods for the fetal heart chamber segmentation and classification.
Time efficiency analysis of various heuristic-oriented methods for segmenting and categorising foetal cardiac chambers are presented in Table 1. The advantage of TS-GWA is shown by the fact that its time efficiency statistic is significantly lower than those of the competitors. The time efficiency for PSO, GOA, TSA, and GWO were respectively 2.51 percent, 3.02 percent, 1.13 percent, and 2.01 percent. The supplied TS-GWA is therefore better at segmenting and categorising the foetal heart chambers since it saves time than the existing methods.
Time efficiency analysis
Time efficiency analysis
In this work, we proposed revolutionary intelligence technologies to segment and classify the fetal heart chambers. The data was initially acquired through prenatal imaging in the US system. The total variation approach was used to pre-process the acquired data. The TF-IDF technique was used to extract features from pre-processed images. Because the length of the extracted features was so long, the best features were extracted. The SRDCF technique was used to segment images based on the ideally selected characteristics. The LSTM was used to classify prenatal images in the last stage, where the hidden neurons were tweaked, resulting in MLSTM. The unique hybrid optimization technique combined TSA and GWO, resulting in TS-GWA for feature selection and hidden neuron optimization in MLSTM. From the extensive experiments results, higher PSNR and Accuracy has been achieved to segment the fatal images. Also, the proposed TS-GWA based optimization technique achieve the better prediction of fatal image content over the existing algorithms.