
Abstract
Dance-based interventions have been proposed for the management of Parkinson’s disease (PD) symptoms. This review critically appraises and synthesises the research on the effects of dance interventions on gait, cognition and dual-tasking in PD, through a meta-analysis of peer-reviewed literature from seven databases. Eligible studies included people with PD, used a parallel-group or cohort design with a dance-based intervention, reported outcome measures of gait, cognition or dual-tasking, and were published in English up until September 2017. Of the initial 1079 articles, 677 articles were reviewed for eligibility, and 25 articles were retained. Only 12 articles had sufficient common assessment items for meta-analysis. Two independent reviewers extracted the data and assessed the risk of bias of each study using the Cochrane risk-of-bias tool. Based on pre-post change scores, gait speed, Timed Up and Go (TUG) test performance, freezing of gait questionnaire, and six-minute walk test times significantly improved after a dance intervention compared to controls. Global cognition assessed with Montreal Cognitive Assessment, and cognitive dual-tasking measured using dual-task TUG, also exhibited greater improvement in dance groups. There was limited evidence to determine the most effective intensity, frequency, duration of dance interventions or the most beneficial music. Findings must be interpreted cautiously because of the lack of randomised control trials, and the moderate to high risk of bias of studies. However, the results of papers with level-I and level-II.1 evidence suggest that dance may have the potential to ameliorate PD symptoms, particularly gait, global cognition and cognitive dual-tasking.
INTRODUCTION
Dance interventions in people with Parkinson’s disease
Dance is a multifaceted activity with many different forms of expression which occur in societies around the world [1, 2]. It may include patterned rhythmic movement in space and time, the use of music, expression of ideas or emotions, or simply taking delight in the movement itself [3, 4]. Dance may occur in groups, pairs or individually and may draw on structured sequences or improvisational approaches. The use of dance for wellbeing and as a healing ritual dates back to early human history [2, 5]. In the western medical context, dance as a therapeutic intervention was formalised by the work of Marian Chace in the 1940s using dance for a group of patients who had extreme emotional disturbances [6]. The American Dance Therapy Association defines dance therapy as the psychotherapeutic use of movement [5, 7] and Dance Movement Therapy
Dance Movement Therapy is “focused on movement behaviour as it emerges in the therapeutic relationship. Expressive, communicative, and adaptive behaviours are all considered for group and individual treatment. Body movement, as the core component of dance, simultaneously provides the means of assessment and the mode of intervention for dance/movement therapy”.
Over the past decade, dance has emerged as a potential intervention in people with Parkinson’s disease (PD). Dance uses movement to support the intellectual, emotional, and motor functions of the body and is often community based [9]. Dance is a type of exercise that can improve muscle flexibility and strength and also involve functional movements that people with PD may find particularly difficult, such as walking backwards and turning [9, 10]. Execution of dance patterns involves motor planning and memory [9]. Dancing involves techniques such as visual focus, rhythm, imagery, proprioception, and imitation of discrete parts of dance sequences [11]. Additionally, dance may provide a context for the practice of dual-tasking which can be problematic for people with PD [9, 12]. Finally, dance may act as an enjoyable alternative way to exercise [10], improving adherence with greater social connectivity. Different dance styles have been used as an intervention for managing symptoms of PD worldwide which include Argentine Tango [13–15], American Ballroom[16], contact improvisation [17, 18], waltz, foxtrot [19], and different cultural dance [20–22]. The Dance for PD® methodology has also been used which incorporates different dance styles, an emphasis on an artistic experience and is specially designed for individuals with PD [23]. Most reviews on the effects of dance have concentrated on motor symptoms such as gait [9, 24] and balance [25, 26] and non-motor symptoms such as quality of life [27, 28], mood [27] and cognitive function [9, 29]. Some reviews have reported the frequency, intensity, duration, and types of dance [25–32]. There are now several recent studies assessing the effects of dance on gait and cognitive outcomes that have not yet been captured by past reviews. Furthermore, none of these reviews has comprehensively synthesised literature on the impact of dance on dual-tasking. Therefore, the current systematic review updates and extends the existing knowledge by quantifying the effects of dance on gait, cognition and dual-tasking, and summarising the characteristics, attrition and safety of dance interventions. It also provides a rigorous evaluation of the methodological quality of the studies.
Objectives
This systematic review aimed to 1) appraise the literature evaluating dance as an intervention to improve gait, cognition and dual-tasking in people with PD; and 2) identify strengths and limitations of this evidence through a formal risk of bias analysis, in order to inform future researchers and practitioners.
METHODS
The current review followed the Preferred Reporting Items for Systematic Reviews and Meta-analysis (PRIMSA) guidelines [33]. The protocol was registered in the international prospective register of systematic reviews (PROSPERO) with CRD number 42017062278 on 7 April 2017. Since the registration, minor changes were made to the inclusion criteria and outcomes as outlined below.
Literature search strategy
A systematic search of the literature was undertaken on 28th September 2017, by the principal reviewer (NK). This included searching electronic bibliographic databases; PubMed, Cochrane Central Register of Controlled Trials (CENTRAL), Embase on Embase.com, CINAHL on EBSCOhost, PsycINFO on EBSCOhost, Web of Science, and Scopus. Clinical trials were accessed through ClinicalTrials.gov. The search terms included the Mesh terms “Parkinson*”, “Parkinsonism”, “Parkinson’s Disease”, combined with “dance”, “dance therapy”, “danc*”, “ballet”, “jazz”, “tap”, “salsa”, “tango”, “waltz”, “foxtrot”, “contemporary”, “ballroom”, “Irish set”, and “Zumba”. This search was combined with three different groups of search terms in order to collect the articles separately on gait, dual-tasking and cognition. Searches were limited to articles in English. The key words and syntax used are presented Supplementary Material 1.
Inclusion and exclusion criteria
Original research studies published in peer-reviewed journals were included in this review. Dance is a fundamental form of individual and group human expression that has evolved into different genres [34]. The current review included studies of dance interventions without restricting the type of dance. Details of inclusion and exclusion criteria are provided in Supplementary Material 2. In brief, studies meeting the following criteria were considered for inclusion: 1) study participants had PD (any stage of the disease, any age, and gender); 2) at least one study group underwent a type of dance intervention lasting for at least two weeks (changed from 3 weeks in PROSPERO registration to 2 weeks which allowed inclusion of two more studies); 3) the study reported on at least one outcome measure for gait or cognition or dual-tasking; 4) randomised and quasi-randomised (studies where participants were not strictly randomised to intervention arms) controlled trials and observational studies (case-control, cohort and crossover studies). Only fully peer-reviewed articles with full text available in English were included without a date limitation.
Outcomes of interest
Multiple outcome measures in each of the three domains (gait, cognition, dual-tasking) were considered. For gait, the primary outcome measure was gait velocity (m/s) with secondary measures of stride length, step length, single support time, swing stance and double support percentages, and cadence (steps/min). Clinical measures of gait such as Timed up and go (TUG) test, six-minute walk test (6MWT), and freezing of gait questionnaire (FOG-Q), which were commonly used across studies, were included. Movement Disorder’s Society: Unified Parkinson’s Disease Rating Scale-III (MDS: UPDRS-III) which represents motor function including gait was also included. For cognition, the primary outcome measure was executive function, while attention, working memory, response inhibition, processing speed, planning, and visuospatial function were secondary outcome measures. The Montreal Cognitive Assessment (MoCA) was included to assess global cognition. For dual-tasking, the primary outcome measure was gait velocity (m/s) during a manual or cognitive secondary task. There was sufficient literature on the selected primary outcome measures for a detailed review. Therefore the secondary outcome measures (balance, QOL, mood, caregiver burden), which were identified in the registered protocol, were not included in this review. All outcomes were assessed using measures that have been recommended for the use in PD population by the Academy of Neurologic Physical Therapy PDEDGE task force (Gait – TUG, 6MWT, FOG-Q, MDS: UPDRS-III; Cognition – MoCA, Dual-tasking – dual – task TUG) [35].
Selection of studies
Following the database search, duplicates were removed by the principal reviewer NK. The two main reviewers, NK and SB, determined suitability of the articles in a staged process in an independent and blinded manner. The titles were independently screened by each reviewer. The abstract screening was carried out for all articles recognised as relevant by either reviewer. Remaining articles were read in full, by the two reviewers independently and checked for compliance with the inclusion criteria. Any disagreement between the reviewers was resolved through discussion or third-party adjudication (GK and KS).
Data extraction and management
Data were extracted by NK and SB in an independent and blinded manner. The extracted data were summarised, including author, year, participant characteristics (number of participants, sex, age, and disease severity), intervention characteristics (the type of dance, frequency, intensity, length of session, and duration of the intervention), outcome measures, and main results.
Risk of bias assessment
The risk of bias assessment was carried out by NK and SB independently using the Cochrane Risk of Bias tool [36]. The methodological quality of studies was assessed with respect to sequence generation, allocation concealment, blinding of participants, personnel and outcome assessors, incomplete outcome data, selective outcome reporting, and other sources of bias [36, 37]. Each of these domains was assessed as high, low or unclear risk of bias according to Section 8.5 of the Cochrane handbook [37]. The risk assessment ratings were based on the published study report and the related trial registration protocols if available. For dance intervention studies without a control group (i.e. cohort studies), random sequence generation and allocation concealment were considered as high risk [37]. Disagreements between authors regarding the risk of bias for domains were resolved by third-party adjudication (GK and KS).
Data analysis
Details of the 27 included studies (e.g., participant details, interventions, outcome measures) were collated in customised forms (Supplementary Material 3–5). Meta-analyses were performed for outcomes sufficiently reported only in nine RCTs and four parallel group designs [13–15, 38–43]. Selected outcomes were gait velocity during preferred forward walking, freezing of gait score, six minute walk test time, UPDRS-III, MOCA score, and TUG time during normal walking and dual-tasking. The means and standard deviations (SD) or standard errors (SE) of these outcomes were used. Authors were contacted through email for unreported data. Review-Manager version (RevMan) 5.3 was used for data processing and missing SDs were calculated using the RevMan calculator. Forest-plots using the change scores of pre-and post-intervention were used to compare the group effects (Dance vs. control). Sub-totals were calculated for the RCTs and parallel group designs separately.
RESULTS
Identification of studies
After duplicates were removed from the 1075 studies that were identified from the databases and the four studies identified from other sources, 677 studies remained (Fig. 1). Following the title and abstract review, 44 underwent full-text review. Seventeen papers were excluded with reasons detailed in Fig. 1. The remaining 27 articles met the eligibility criteria and were included in the review (Supplementary Material 1). Only 12 articles had sufficient common assessment items and adequately mentioned results for meta-analysis.

Summary of search and selection process based on included and excluded studies.
Study cohort
The 27 studies included in the review comprised a total of 586 participants with PD. Overall, 403 participants followed the dance intervention and 183 were part of a control group (standard medical practice) or another intervention (strength, mobility, balance, or resistance exercise). The mean age of participants in the included studies was 68.06±3.09 years. The male to female ratio was 0.97. All of the included studies used the Hoehn and Yahr classification [44], according to which, participants were in the mild to moderate stage with a mean disease severity level of 2.22±0.44, and overall range between 1–3.
Study characteristics and methodological quality
Nineteen studies were conducted in the US [14, 45–53], two each in Italy [13, 22] and Ireland [54, 55], and one each in Japan [56], Germany [57], Canada [15], and Thailand [20]. All studies had relatively small sample size ranging from 7 [47] to 46 [56]. Among the included 27 studies, nine were RCTs with the highest level of evidence (Level 1 according to the Canadian Task Force on the Periodic Health Examination) [58]. Six studies were at Level II.1; well-designed cohort or case-control studies. The majority of the studies (12) were at Level II.2; time series comparisons.
Intervention characteristics
Type of intervention
Whilst a variety of dance styles were evaluated in the studies, the most popular was Argentine Tango; (used by 14 studies [13–15, 48–51]). Of these studies, four mentioned the use of adapted materials [14, 50]. Adapted tango has the same spirit and the general structure of traditional Argentine tango, but the positioning of partners and some steps have been modified to address the impairments of PD [59]. In the majority of these Tango studies, PD participants partnered with individuals without PD and spent time in both leading and following roles. Three studies each used Irish set dancing [22, 55] and contact improvisation dancing [18, 47]. In four studies the dance classes were based on Dance for PD® methodology [23, 57]. One study used Thai classical dancing [20], another study used a combination of different dance styles [56], and one did not state the type of dance style [52]. Ten studies had no control group [18, 57]. Seven studies used passive controls without any intervention [15, 56]. Ten studies used active controls with diverse interventions [13, 52]. These active control interventions consisted of traditional exercise classes, home-based exercises or education sessions. The study by McNeely (2015) compared two different dance interventions only: non-partnered Tango versus Dance for PD® [51]. Twenty two studies provided details of the dance instructors [14, 57], among which 11 of them mentioned that the instructors were professional and experienced in the particular dance [18, 53]. None of the studies mentioned that the instructors were registered under a recognized dance therapy association.
Duration
Dance class duration ranged from 60 to 90 minutes. Fifteen studies had 60 minute classes [13, 56], three had 75 minute classes [23, 57], one study had 85 minute classes [46] and eight had 90 minute classes [14, 55]. The duration of the intervention ranged from two to 104 weeks. The majority of studies (six) completed a twelve-week intervention [14, 56]. Three studies each had three weeks [45, 50], ten weeks [23, 54], and 13 weeks [40–42] of intervention. Two studies conducted a two-week intervention [18, 48], two studies reported an eight-week intervention [19, 55], and two studies completed a 2-year (104 week) intervention [38, 39]. One study each had six weeks [52], seven weeks [47], 16 weeks [53], 24 weeks [22], and 32 weeks [57] of classes.
Frequency
The majority of the studies (12) provided classes twice a week [13–15, 51], while three studies had three classes per week [20, 47]. Four studies conducted classes five times a week [18, 50]. Remaining eight studies had one class per week [22, 52–57].
Exposure
The exposure of the dance interventions (session duration x number of sessions) ranged from 12 hours to 208 hours. Five studies each had 12 hours [52, 56], 20 hours [13, 53], 24 hours [15, 51], 26 hours [40–42], 36 hours [14, 22] 104 hours [38], and 208 hours [39] of exposure to intervention. Two studies had exposure of 22.5 hours [45, 50].
Intensity
None of the studies measured the intensity of the dance intervention; for example, in terms of energy expenditure or heart rate. Seven studies stated that the intervention was progressive [13, 49] but did not specify how. Hackney (2009) stated that at each class a new step was introduced as an addition to previously learned steps [48].
Assessment time points
The majority of studies (22) reported two assessment time points one week before the intervention (pre) and one week after the intervention (post). Two studies [38, 39] had an assessment time point half-way through the study. Three studies had a follow-up assessment, four weeks [49], 8 weeks [13] and 10–12 weeks [14] post-intervention.
Attrition and safety
Among the twelve studies that mentioned attrition rate, three studies had active controls (Average attrition: IG = 35.5%, CG = 28.5%), three studies had passive controls (Average attrition: IG = 35.2%, CG = 24.4%) and six studies had no controls (Average attrition: 14%). While the dance and control groups had similar attrition rates, generally the dance group had more enjoyment and willingness to continue the classes [15, 55]. Duncan (2012) reported that 11 of the 16 individuals in the Tango group chose to continue attending classes even though they had formally completed the 12-month study [38]. Several studies reported the safety of the dance classes. Seven studies stated that there were no adverse events during the dance classes [13, 55]. Volpe (2013) reported one non-injurious fall during Irish set dancing class [22], while McKee (2013) reported two non-injurious falls related to two self-reported frequent fallers [14]. Romenets (2015) mentioned that 11% of Tango group and 13% of controls experienced falls during the class [15].
Risk of bias
Overall there was a moderate to high risk of bias across all studies (Figs. 2 and 3). There was a high risk for random sequence generation (approximately 70%) and allocation concealment (approximately 75%) across the reviewed studies. While blinding of the participants would be difficult due to the nature of the intervention, blinded assessment of the outcomes was feasible, as indicated by the low risk for blinding of outcome assessment (approximately 60%). Among the 27 studies, one study was double blinded [49] (participants were blinded to study hypothesis), 16 were single-blinded, and the remaining ten studies were not blinded (singly or doubly). The majority of the studies (over 75%) had a low risk for attrition bias. Selective reporting had an unclear risk of bias (approximately 70% of studies). Six studies made reference to a published protocol. Trial registration details were found for five of these [15, 57]. Twenty-five studies had low risk, and two studies had a high risk of “other bias” [43, 50]. For instance, one study was supported in part by a dance association [50], and the other study declared a conflict of interest with respect to the research, authorship, and/or publication [43].
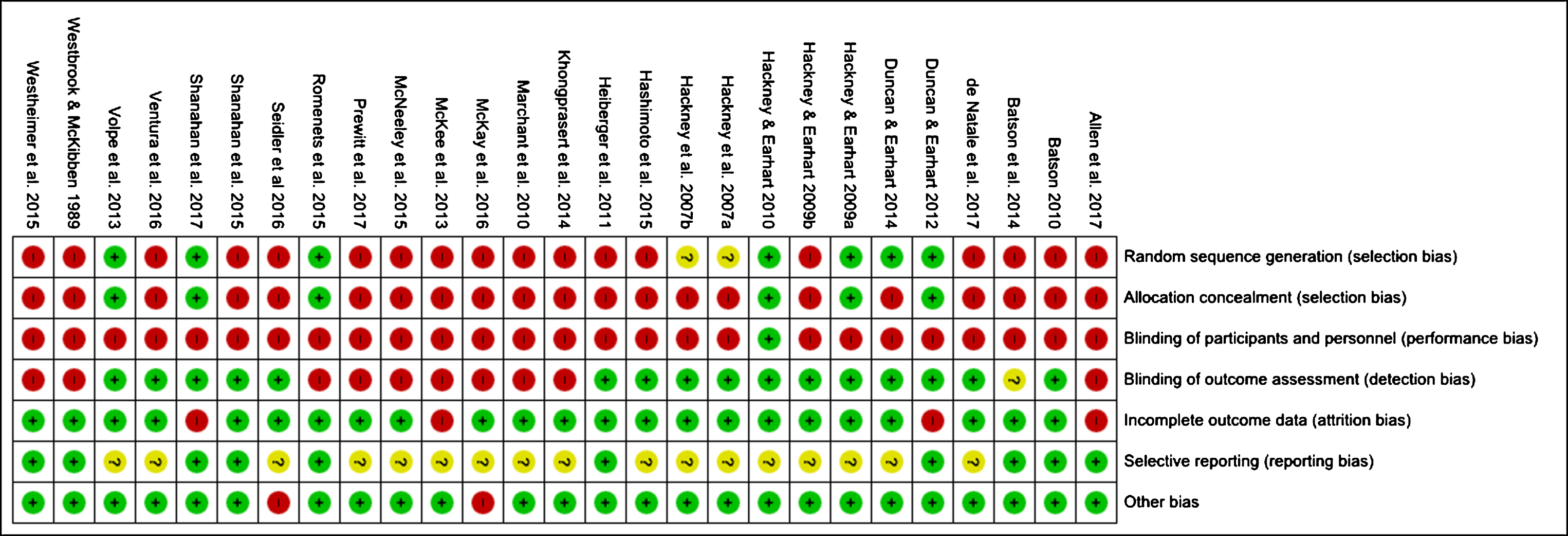
Risk of bias summary: review authors’ judgement about each risk of bias item for each included study.

Risk of bias graph: review authors’ judgements about each risk of bias item presented as percentages across all included studies.
Gait
Fourteen studies measured gait velocity (m/s); eleven when walking at a preferred speed walking over 8–10 m [18, 52], eight when walking backwards [18, 51], and seven when walking at a fast pace [18, 49–51]. Five studies measured spatiotemporal gait variables such as stride length, step length, single support time, swing and stance percentages, double support time, and cadence (steps/min) [18, 49] (Supplementary Material 3).
Eight studies used a pressure sensitive mat (computerised GAITRite walkway) to measure gait velocity [18, 51]. Two studies [41, 42] used a motion capture system to measure gait variables. Twelve studies used Six-Minute Walk Test (6MWT) to measure walking endurance [13, 55] and Timed Up and Go (TUG) to reflect dynamic balance during walking [15, 48–51]. Gait, balance and falls risk was measured using the Dynamic Gait Index (DGI) in three studies [13, 50]. The Functional Ambulation Profile (FAP) was only used in one study [48] (Supplementary Material 3). Seven studies used the freezing of gait questionnaire [15, 50].
Based on the results of the meta-analysis, the RCTs [15, 42] (Level I Evidence) demonstrated significant improvement for gait velocity [38, 42] (SMD 0.49 [95% CI 0.04, 0.94], Fig. 4A), freezing of gait (SMD – 0.37 [95% CI – 0.74, – 0.01], Fig. 5B) and TUG (SMD – 1.38 [95% CI – 1.98, – 0.78], Fig. 5C), but not for the 6MWT (SMD 0.51 [95% CI – 0.01, 1.03], Fig. 4B). For studies using a parallel group design [13, 56] (Level II evidence), there was no improvement for gait velocity (SMD 0.37 [95% CI – 0.13, 0.86], Fig. 4A) or freezing of gait (SMD – 0.38 [95% CI – 0.09, 0.34], Fig. 5B). However, there were significant improvements in the TUG (SMD – 0.54 [95% CI – 0.91, – 0.16], Fig. 5C) and 6MWT (SMD 0.75 [95% CI 0.15, 1.35], Fig. 4B). The UPDRS-III presented with significant improvement for both groups; RCTs (SMD – 1.04 [95% CI – 1.69, – 0.39], parallel group designs; (SMD – 6.15 [95% CI – 7.17, – 5.14], Fig. 5A).

Subgroup analysis forest plot of comparison based on pre-post change scores: Dance vs. control – Randomised Control Trials and Parallel Group Designs: Gait velocity, Six-minute walk test and Montreal Cognitive Assessment (CI, confidence interval; IV, inverse variance; SMD, standard mean difference).
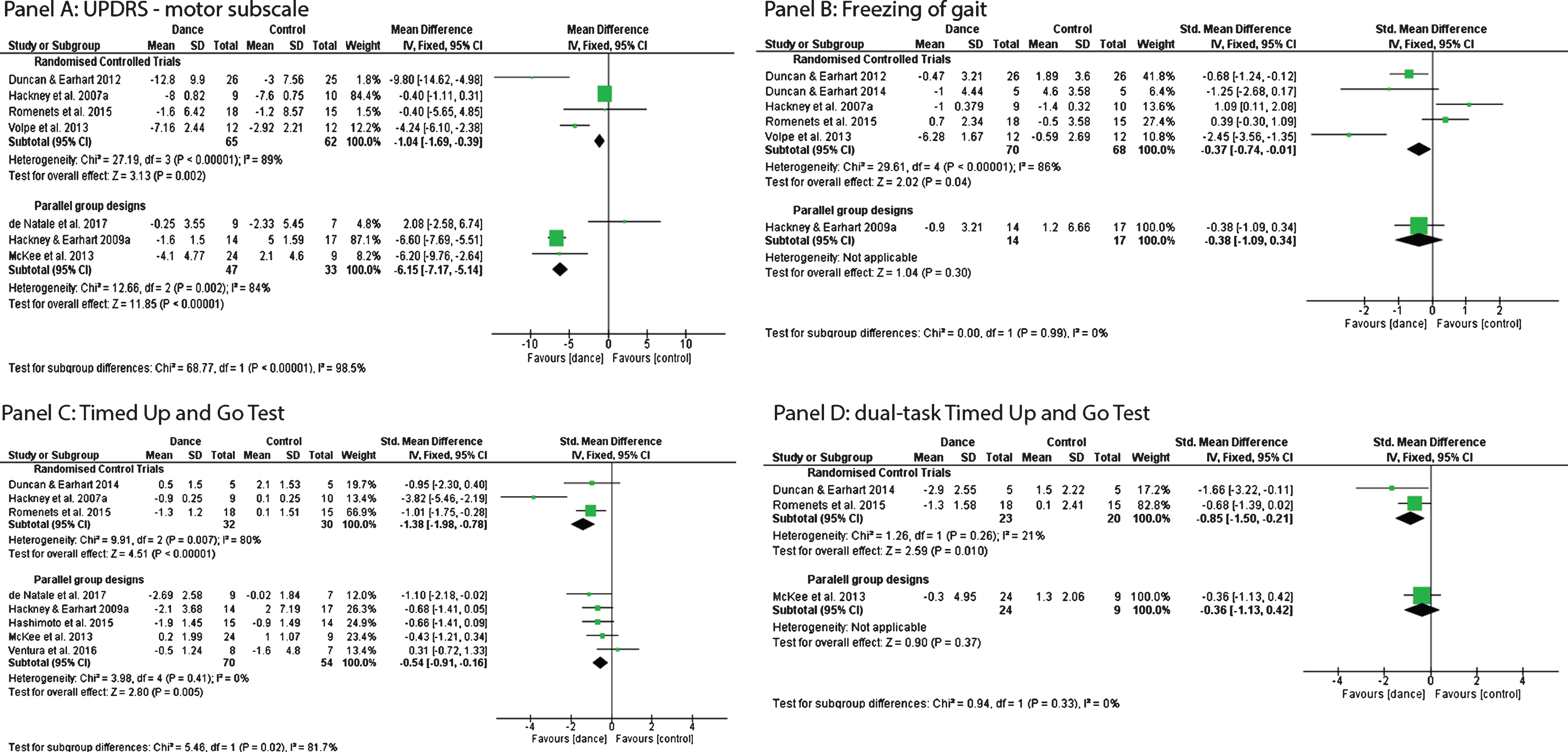
Subgroup analysis forest plot of comparison based on pre-post change scores: Dance vs. control – Randomised Control Trials and Parallel Group Designs: UPDRS: motor subscale, Freezing of Gait, Timed Up and Go test and Dual-task timed Up and Go Test (CI, confidence interval; IV, inverse variance; SMD, standard mean difference).
Cognition
Overall the tests used were MOCA, SCOPA-COG (if we consider total score) and FAB: which are screening measures of overall cognition and frontal functions. The TMT-A, TEA, and visual elevator test were used to measure attention. Digit span, Brook’s spatial task and a reverse Corsi block test were used to measure working memory. TMT-B and Stroop test measured executive functions.
Two RCTs (Level 1 Evidence) utilised the MoCA for assessment of global cognition which we included in our meta-analysis [14, 15]. MoCA demonstrated a significant improvement following the dance interventions (SMD 0.52 [95% CI – 0.00, 1.04], Fig. 4C).
Results below are based on the cognitive skills not included in the meta-analysis (Supplementary Material 4). The overall cognition improved significantly measured using the SCOPA-COG test [49]and FAB [56] in the dance group. Executive function using TMT-A and B [13] and reported a significant improvement in TMT-A and TMT-B scores in the dance group compared to a group who underwent balance and motor coordination exercises [13]. Among the studies which measured attention, the studies which used TMT-A and TEA demonstrated significant improvement [13, 23]. No significant improvement was found for visuospatial memory assessed using the reverse Corsi Block test [14] or working memory measured with Digit Span forward and backward [23] in the dance groups compared to the controls.
Apart from the basic cognitive skills, Mental rotation task [56] (a complex task evaluation of different cognitive functions including spatial and numerical abilities [60]) and the Alternate uses test (AUT) [23] (a standard test of divergent thinking, used to measure creativity) had also demonstrated significant improvement in the dance group.
Dual-tasking
Eight studies, including three RCTs, measured dual-tasking using walking as the primary task (Supplementary Material 5). Six studies measured dual-cognitive tasks [15, 51]. Secondary tasks included verbal fluency (word naming) [38, 51], subtraction by 3’s [14] or 7’s [41]. There was significant improvement in dual-task TUG results for RCTs (SMD – 0.85 [95% CI – 1.50, – 0.21], Fig. 5C) (Level 1 Evidence) but not for parallel group designs (SMD – 0.36 [95% CI – 1.13, 0.42], Fig. 5C). Gait velocity during dual-task walking significantly increased in one study [38] but not for another [41]. The effect was higher for the verbal fluency task designs (SMD – 1.66 [95% CI – 3.22, – 0.11], Fig. 5C) compared to a serial subtraction task designs (SMD – 0.66 [95% CI – 1.39, 0.02], Fig. 5C). Two studies [14, 50] measured dual-manual tasks. One study used the Manual-TUG with carrying a full cup of water as the secondary task [14] but the second study did not provide details about the manual secondary task [50]. Neither study demonstrated a significant improvement in walking [14, 50].
DISCUSSION
The current review aimed to summarise the existing literature on the effectiveness of dance for PD in the areas of gait, cognition and dual-tasking and to identify limitations that should be addressed in future studies. In total, 27 publications published between 1989 to 2018 were included in this review and 12 of these in a meta-analysis. The dance styles tested were Argentine Tango, Irish set, contact improvisation, Dance for PD®, and Thai classical dancing. Level I Evidence from the Randomised Control Trials indicated support for the positive effects of dance [61]. Based on the pre-post change scores between dance and control groups of RCTs included herein, gait velocity, FOG-Q, TUG, UPDRS-III, MOCA, and DT-TUG exhibited significant improvement. Based on the results of parallel group studies (non-randomised), the 6MWT and TUG showed significant improvement. Although all of the reviewed studies had a moderate to high risk of bias, overall the results indicate that dance interventions induce better responses particularly in gait velocity, global cognition and cognitive dual-tasking when compared to active or passive controls.
Intervention characteristics
Argentine Tango was used in the majority of studies. There was limited evidence on the use of other dance types making it difficult to determine the most beneficial dance intervention. Moreover, there was limited information available on the interventions themselves, namely components performed in sitting, standing and moving across the floor, and the type of music used. Differences in outcomes for dance types and the components might be expected given that each dance genre has its own style, cognitive demands and musical stimulus [62]. For example, participants who practice Tango usually spend a larger proportion of class time practicing stepping, posture, and rhythmic movements [51] and potentially have more opportunity to improve their walking compared to other dance styles.
Health care and exercise professionals commonly use the Frequency, Intensity, Type, and Time (FITT) principle when prescribing exercises [63]. The American College of Sports Medicine (ACSM) guidelines suggest that a FIIT principle of 3 days a week, moderate intensity (40 % – 60% VO2 reserve), 30 min of continuous or accumulated aerobic activities such as walking, cycling swimming or dancing is recommended for individuals with PD [64]. Most of the reviewed dance studies came close to meeting this guideline in terms of exposure per week. However, there was insufficient information to judge the exercise intensity. The majority of the studies employed 60 minutes, twice weekly dance sessions, for three months, and this regimen appeared to be both effective and feasible in improving selected outcomes. However, there was substantial variability in the duration and frequency of the sessions. Interestingly, some of the studies with a shorter exposure duration, such as 12 hours [52, 56], 12.5 hours [23], and 12.75 hours [46] demonstrated significant improvement in gait velocity, TUG and UPDRS-III, when comparing pre-post measures. Even the shortest duration studies which were performed over two weeks (15 hours) presented with significant improvements in the gait cycle including improved stance [18, 48] and swing phases [18].
Researchers have used the metabolic equivalents of task (METs) per minute to estimate the energy expenditure related to physical activities (the ratio of the work metabolic rate to the resting metabolic rate) [65]. One MET is considered a resting metabolic rate obtained during quiet sitting [66]. As per the published MET values Tango and slow ballroom dancing (e.g., waltz, foxtrot_ is considered a light-moderate exercise with a typical expenditure of at least 3 METs per minute [67]. Other styles, such as Irish step dancing or ballet, modern, and jazz have higher MET values of 4.5 or 4.8 per minute, respectively [65]. The published MET estimates for different dance types suggests that, in general, the energy required to perform different dance styles varies. If this holds true in clinical applications, it suggests that a direct comparison of findings from studies that use different styles cannot be completely justified.
Overall there is a lack of details about the dance classes which is vital for the rigour and replicability of these studies. It is important, to be as specific as possible regarding the activities, the amount of time spent on each activity and the movements that were part of each component. These details would be important to provide the readers with a sense of what these dance classes looked like in practice and how they could be replicated. Moreover, the qualifications and the experience of the dance teachers could greatly influence the participants’ experiences. While selected studies used qualified, professional dance instructors, for some studies the instructor experience was less evident, which might have influenced the results. Future researchers could also consider further articulating dance teacher experience and approaches as well as potentially including qualified dance movement therapy instructors to explore the dance movement therapy context.
Adherence
Well-documented barriers to engaging traditional exercises for people with PD include low outcome expectation, lack of time, and fear of falling. These factors have contributed to suboptimal adherence for traditional exercise programs [68, 69]. Dance-based interventions have attempted to overcome some of these barriers by allowing for and promoting social benefits [9, 70]. Dance interventions have demonstrated high adherence, particularly the studies with less than 16 weeks (below 20% attrition) [15, 55]. Westbrook (1989) stated that “a number of participants were tearful [at program end], expressing how meaningful and enriching experience the dance had been for them” [52]. While the current review found similar attrition rates in dance groups compared to active or passive control groups, most studies stated that participants wanted to continue the dance classes even after the study completion [38, 55]. However, the feasibility of longer duration interventions needs to be carefully considered, given that Duncan (2012) had 50% attrition rate over 12 months [38]. This might be ameliorated in longer duration studies by prescribing home-based activities to compliment dance [54, 55].
Assessment of gait
Gait was measured in eight RCTs (Level I) [15, 54], seven parallel group designs (Level II.1) [13, 56] and nine time series comparisons (Level II.2) [18, 57], using different tools ranging from qualitative clinical measures to objective measures. Gait velocity was measured objectively, mainly using a GAITRite walkway [71], Two studies used a motion capture system to measure gait velocity by tracking a reflective marker placed on the trunk [41, 42]. These systems were used in the RCTs included in the meta-analysis [38, 42] and demonstrated significant improvement in gait velocity. The TUG score was improved significantly both in RCTs and parallel group designs, FOG-Q scores improved significantly in the RCT studies, and 6MWT scores were improved in parallel group studies. The noted improvement in gait is supportive of the benefits of auditory cueing, in the form of music used in dance, acting to improve gait initiation, walking speed, and cadence [46].
Assessments of cognition
Only a small number of studies including two RCTs [14, 15] (Level I), three parallel group designs [13, 56] (Level II.1) and one time series comparison [19] (Level II.2), measured the impact of dance on cognition. These studies assessed a relatively narrow selection of cognitive abilities, primarily attention/working memory or, executive functions, or they used a screening measure of global cognition (i.e., MOCA). The average global cognition scores of dance group participants, showed a significant improvement in the meta-analysis. Executive function [13] and attention [13, 23] also improved, whereas working memory [14, 23] did not show a significant improvement.
Assessment of dual-tasking
Three RCTs [15, 39] (Level I), three parallel group designs [14, 51] (Level II.1) and two time series comparisons [47, 50] (Level II.2) measured dual-tasking. Most of the studies that assessed improvement in dual-task following a dance intervention used a cognitive secondary task. Only two studies used a manual secondary task. However, there were insufficient data to determine whether spatiotemporal gait variables improved during dual-tasking. The meta-analysis of the RCTs which used dual-task TUG exhibited significant improvement in the dance group. No study reported dual-task cost, which is the difference between the dual-task performance and the single-task performance [72]. Dual-task cost is an indicator of the efficiency of the dual-task performance, and would provide a further indicator of the effectiveness of the intervention [73]. The higher effect size for verbal fluency dual-tasks indicates the potential benefits to everyday activities such as walking and talking.
Comparison with other reviews
The current review extends previous reviews because of its novel focus (dual-task performance while walking) and the inclusion of a risk of bias assessment. This review presented the findings from nine RCTs (Level I evidence) and six parallel group studies (Level II.1 evidence) separately so the potential biases of the original studies could be considered in the interpretation as well as differences in the level of evidence.
Quality of evidence
There was a moderate to high risk of bias in all studies, most of which had relatively small samples, indicating the limited quality of the evidence overall. There were relatively few RCTs, and even these had a moderate risk of bias (detection bias, attrition bias and reporting bias). Apart from one study that used another dance type as a control [49], the remaining 26 studies did not use blinding, leading to high-performance bias. Allocation concealment was poorly performed across almost all studies resulting in high selection bias. The bias from selective reporting could not be evaluated, as there were insufficient details to make a judgment. The inclusion of cohort studies with their inherent non-randomised and uncontrolled study designs also created a default high risk of bias. Overall the level and quality of the evidence is a major limitation in establishing benefits of dance for PD on the selected areas.
Recommendations
Longer term trials, particularly RCTs that are appropriately powered, must be undertaken to provide stronger evidence of the potential benefits of dance interventions for people with PD. This includes follow-up evaluations of the durability of effects and evaluations of clinical benefits and cost-effectiveness of programs, including whether they lead to functional gains. While the meta-analysis found positive effects for gait velocity, there were insufficient data to analyse other spatiotemporal gait parameters; thus additional studies with these measures are required, as are studies that compare dance genres and explore the optimal frequency, duration and intensity of programs, and their timing relative to disease stages. Although dance has shown positive effects in limited aspects of cognition, there is scope to assess a wider range of abilities, standardise the measures, and potentially, to include finer-grained tests. In fact, the use of common measures for all outcomes would aid future attempts to pool data. Future trials should follow published reporting standards (e.g., CONSORT) to facilitate assessments of the quality of the evidence.
Conclusion
Dance has become a popular adjunct management option for patients and clinicians to consider in addition to the primary treatments for PD. The community-based nature of dance promotes enjoyment and a higher adherence rate. The nine RCTs provide the highest level of evidence to support the positive effects of dance on gait velocity, freezing of gait, global cognition (screening test) and dual-tasking and while promising, additional RCTs are needed to confirm these results and address the many important questions that remain about this activity.
CONFLICT OF INTEREST
The authors declared the potential conflicts of interest with respect to this manuscript. Erica Rose Jeffrey is the Director of Dance for Parkinson’s Australia and a lead teacher in Dance for Parkinson’s attached to Queensland Ballet.