
Abstract
BACKGROUND:
Paresthesia is defined as a burning or prickling sensation or partial numbness caused by neural injury.
OBJECTIVE:
The purpose of this paper is to present a rare and unusual case report of odontogenic infection-induced inferior alveolar nerve (IAN) paresthesia along with cutaneous draining sinus on the face of a pediatric patient and to discuss the possible pathophysiologic mechanism of nerve injury.
METHODS:
A 14-year-old female patient with cutaneous sinus and paresthesia associated with inferior alveolar nerve was enrolled in the study and the clinical and radiological manifestations of sinus lesion were carefully evaluated.
RESULTS:
The most appropriate treatment was carried out not only to resolve extraoral sinus but also to ensure progressive healing for the complete resolution of neurological disturbance.
CONCLUSION:
The simultaneous occurrence of infection and paresthesia strongly suggested a definitive relationship. Therefore, there seems to be a correlation between duration, origin, significance of the injury and the prognosis of paresthesia.
Introduction
Paresthesia is defined as a burning or prickling sensation or partial numbness caused by neural injury. It is described by the affected patients as: warm, cold, burning, aching, prickling, tingling, pins and needles, numbness and itching [1–3]. Literature reviews have advocated that local factors including mechanical, thermal, or toxic injuries of the inferior alveolar nerve (IAN) can be a potential cause of inferior alveolar nerve parethesia [4]. Mechanical injuries of the nerve corresponds with compression, stretching, partial or total resection, and laceration that are frequently caused by block anesthesia, third molar surgery, or local tumor infiltration [5]. Infection-related paresthesia is usually also related to mechanical pressure and ischemia associated with the inflammatory process (edema) or local pressure to the mental nerve or inferior alveolar nerve, consequent to the accumulation of purulent exudates in the mandibular bone. Another cause of paresthesia could be the toxic metabolic products of bacteria or inflammatory products released following tissue damage [6]. Thermal injury is an end result of osseous overheating during the execution of surgical techniques. Chemical trauma can be caused by toxic elements of various materials, such as the para-formaldehyde, sodium hypochlorite, or local anesthetics. In the majority of the cases reported in the literature, the duration of the neurologic symptoms associated with the inferior alveolar nerve and its branches vary greatly from days or weeks to several months and, in some cases, paresthesia might even become permanent [7]. This paper aims to present a rare and unusual case report of odontogenic infection-induced IAN paresthesia along with cutaneous draining sinus on the face of a 14-year-old female patient and to discuss the most appropriate treatment solutions.
Case report
A 14-year-old female patient reported to the dental outpatient department with the chief complaint of hemimandibular pain and numbness on the left half of the lower jaw associated with intermittent pus discharge at the base of the left side of the mandible. The symptoms were present for one year. The history further revealed the occurrence of swelling in the cheek, well-localized, and reduced after burst. The patient reported to a nearby medical practitioner for an opinion, suspecting it to be a cancerous lesion. Subsequently, she received several courses of oral antibiotics and supplements, but did not get long-term relief. The burning sensation, however, was disappearing temporarily with the use of antibiotics. Continuous paresthesia and foul smelling discharge led the patient to visit a dermatologist and an otorhinolaryngologist (ENT) specialist before being referred to the dental department.
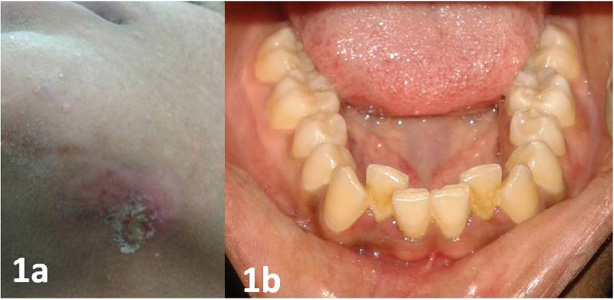
(a) Preoperative photograph of the extraoral cutaneous sinus on the chin; (b) preoperative intraoral photograph.
Extra-oral examination revealed a cutaneous sinus about 2 cm in diameter along the lower border of left mandibular region, with a reddish yellow halo at the center (Fig. 1a). Palpation elicited purulent exudate from the sinus. Detailed intraoral examination revealed that her lower first molar tooth was extremely tender to palpation (Fig. 1b). No abnormalities such as discoloration or carious teeth were noted. Paresthesia extension was explored with a probe and took part around the infected tooth until the left corner of the lower lip. Pulp vitality tests were positive for all the mandibular left posterior teeth except for the lower left first molar. Panoramic radiograph revealed a well-defined unilocular, periapical lesion measuring around 2 cm by 4 cm in relation to this tooth. The well-defined margins of the lesion indicated a chronic-longstanding lesion such as a periapical cyst/periradicular abcess. A computed tomography (CT) scan was done, which displayed large periapical radiolucency involving the first molar extending into the inferior alveolar nerve canal and perforating the lingual cortical bone (Fig. 2). The distal root of the molar exhibited external root resorption. Root canal treatment was initiated for the teeth in question. Mild exudate drained through the canal was sent to the microbiology department for bacterial culture and antibiotic sensitivity testing. Thorough cleaning and shaping of the canal was done, and calcium hydroxide (Metapex, Chungcheongbuk-do, Korea) was placed within the root canal as an intracanal medicament.
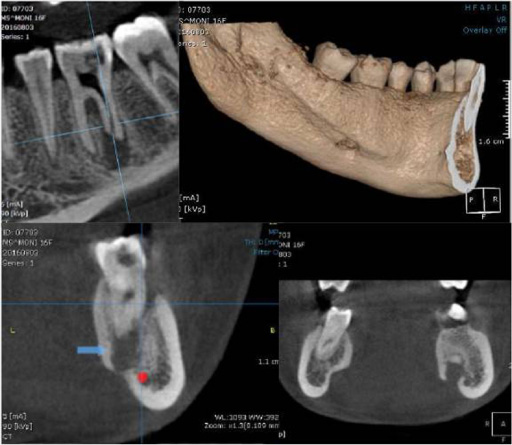
Computed tomography scan revealing distinct radiolucency extending into the inferior alveolar nerve canal, external root resorption of distal root and fenestration defect involving the lingual cortical bone in relation to apices of mandibular left first molar tooth.
On two weeks recall, cutaneous sinus drainage ceased. Calcium hydroxide was removed, and an antibiotic paste was placed as intra-canal medicament (paste of ciprofloxacin 500 mg and metronidazole 400 mg, 1:1 ratio) based on sensitivity testing of microbes within the pus sample [4,5]. The patient was recalled after eight weeks, at which point the extraoral sinus had resolved considerably. The canal obturation was performed by the lateral condensation technique using gutta-percha (Dentsply, Mailleffer, Switzerland) and AH26 sealer (DentsplyDeTrey, Germany). Three weeks after treatment completion, numbness was still present. After evaluation and discussion with the patient, in order to prevent permanent nerve damage, it was decided that the tooth would be extracted (Fig. 3). After a traumatic tooth extraction, a progressive healing initiated up to the complete resolution of neurological disturbance in three weeks. Six months after the tooth extraction, during the radiological examination, complete disappearance of the lesions was observed (Fig. 4a). Clinical follow-up at one year revealed no abnormalities and implant rehabilitation was planned (Fig. 4b).

Extracted mandibular left first molar tooth depicting partial resorption of the distal root.

(a) Postoperative photograph showing diminished extraoral sinus after six months recall; (b) postoperative healed sinus after one-year follow-up.
The diagnosis of neural anesthesia or paresthesia necessitates a review of detailed patient history to evaluate the onset of altered sensation and its progression. The examination of the affected area can be carried out by using thermal, mechanical, electrical, or chemical tests that elicit subjective responses [8]. Radiographic measures such as panoramic radiographs, computed tomography (CT) and neurophysiologic screening may also be valuable in determining the cause of paresthesia [9,10].
In the case presented in this paper, paresthesia was caused as a consequence of the presence of a periapical lesion associated with the mandibular left first molar tooth. However, he intermittent pus discharge at the base of the left side of the mandible diluted the severity and symptoms of paresthesia sporadically. Paresthesia due to periapical lesions may be caused by mechanical pressure and ischemia associated with the inflammatory process (edema), local pressure on the inferior alveolar nerve fibers resulting from accumulation of purulent exudates in the mandibular bone as well as the toxic metabolic products of the bacteria or the inflammatory products released with tissue damage. The expanding infectious process and the associated edema can cause pressure on the nerve fibres severe enough to induce the symptoms of paresthesia [11]. Furthermore, it was demonstrated that the microbial products of certain microbes (gram negative bacteria) can breach the perineurium with resultant nerve bundle deterioration and impaired conduction [12].
Paresthesia resulting from periapical lesions usually subsides through elimination of infection by root canal treatment. During the appropriate nonsurgical endodontic treatment, pharmacologic therapy can be useful. In particular, drugs such as antibiotics, nonsteroidal anti-inflammatory drugs, steroids, proteolytic enzymes, cocarnitine, somatotropic hormone, nerve growth factor, increase tissue oxygenation and to control inflammation, edema, hematoma, or infection as described in the literature [13,14].
In particular, according to Zuniga [15], it was reported that if there are no signs of enhancement in an early phase (i.e. within three months after injury), the immediate extraction of the tooth is the treatment of choice in order to prevent irreversible paresthesia [16] because better treatment outcomes are achieved if nerve paresthesia is treated as early as possible. On the contrary, Gregg [17] stated that because most inferior alveolar nerve injuries are known to resolve spontaneously, there is no conclusive evidence that early intervention is better than delayed nonsurgical management (i.e. more than three months after injury). In the case presented in this paper, cutaneous sinus drainage ceased and extraoral sinus had resolved considerably eight weeks post endodontic treatment. However, no clinical sign of improvement was observed in paresthesia. Consequently, after careful consideration and discussion with the patient, the final treatment planning was decided for the tooth extraction leading to complete resolution of neurological disturbance in three weeks time. The simultaneous occurrence of infection and paresthesia strongly suggested a definitive relationship. Therefore, there seems to be a correlation between duration, origin, significance of the injury and prognosis of paresthesia. The longer the mechanical or chemical irritation persists, the more the nerve fibers degenerate and the greater the risk that the paresthesia will become permanent [18,19].
Footnotes
Conflict of interest
None to report.
Funding
The authors declare that the work was performed without financial support from a third party.