
Abstract
OBJECTIVE:
We hypothesized that in-utero SSRI exposure affects Apgar scores and immediate post-delivery oxygen requirements.
STUDY DESIGN:
SSRI in-utero exposure was assessed retrospectively in preterm neonates ≥ 28 weeks gestation and term neonates. Primary outcome was Apgar <7 at five minutes and delivery room oxygen requirements. Secondary endpoints included one-minute Apgar, length of stay, birth weight, and NICU admission.
RESULTS:
Fifty-one preterm and 117 term neonates were exposed to a SSRI; mostly to sertraline. Pre-term SSRI-exposed neonates had 4.1 times higher delivery room oxygen requirements. One minute Apgar <7 was 3.5 times higher and NICU admission 5 times higher 95% CI (1.3–19) in SSRI-exposed term neonates. Higher doses of sertraline had associated adverse outcomes.
CONCLUSION:
In-utero SSRI exposure was associated with increased neonatal care at birth, differences in Apgar scores compared with controls, and increased NICU admissions. Higher sertraline doses were associated with poorer outcomes.
Introduction
Depression is a common condition, affecting approximately 10% of the general population in USA and a similar percentage of pregnant patients [1–4]. Depression often goes undiagnosed and untreated in pregnant patients [3]. Selective Serotonin Reuptake Inhibitors (SSRIs) and Venlafaxine, a Serotonin Norepinephrine Reuptake Inhibitor (SNRI), are the most common medications used to treat depressive symptoms during pregnancy according to the Centers of Disease Control (CDC). Prevalence of SSRI and SNRI use during pregnancy varies by country 1.8% in Norway to 7.0% in Iceland and 5.6% in the USA according to a 2008 multi-site study evaluating the use of antidepressant medications during pregnancy [1].
SSRIs diffuse freely across the placenta [5]. The majority of SSRIs and venlafaxine are pregnancy category C, with the exception of paroxetine, which is classified as pregnancy category D due to a potentially increased risk for cardiovascular and other congenital malformations [6–13]. Conversely, untreated maternal depression may also have untoward effects on the infant [6, 13]. Continuation of SSRIs/Venlafaxine during pregnancy is a controversial topic that is not adequately addressed in the literature, and this poses a very difficult decision for obstetricians and psychiatrists. Joint recommendations from the American Psychiatric Association (APA) and the American College of Obstetricians and Gynecologists (ACOG) suggest continuing medication in patients with severe depression and replacing or augmenting medication with psychotherapy in patients with recurrent depression or in those who experience symptoms despite medication use. The decision to continue antidepressants in psychiatrically stable patients is individualized and takes patient preference into consideration [14, 15].
Respiratory distress [16–19], seizures, feeding difficulty [17], vomiting [18], hypoglycemia [18], alterations in muscle tone [3, 15–17], hyper-reflexia, jitteriness [2, 19], irritability [15, 17], crying, disturbances [20], tremor [15, 21], and lower Apgar scores [22, 23] in neonates are associated with SSRI exposure to the fetus during pregnancy. Preterm births and low birth weights have been observed with SSRI exposure [14–16, 21]. An increased risk for persistent pulmonary hypertension of the newborn (PPHN) occurs with SSRI exposure after the 20th week of gestation [19]. Additional potential complications of in-utero SSRI exposure include cardiovascular malformations [14, 24], sleep disturbances [17–18], and alterations in heart rate [17]. Available data for 40 months post-delivery suggest that exposed infants have changes in gross motor movement, but not for mental development based on Bayley mental developmental indexes [22]. The long-term effects of in-utero SSRI/SNRI exposure on abstract thinking are not known.
A vast amount of literature regarding the effects of in-utero exposure to SSRIs on term infants is available, with minimal data regarding the effects on preterm infants. Several studies have related prematurity to SSRI exposure [17]. None of the studies to date have included preterm infants as the target population. Additional data is necessary to determine which of the study medications are safest and therefore preferred in pregnant women at risk for preterm delivery and those medications that should be avoided in this population. Information regarding potential higher acuity needs in the delivery room for a neonate exposed in-utero to SSRIs is also lacking. We hypothesized that in-utero exposure to SSRIs or Venlafaxine affects Apgar scores and respiratory outcomes for term and preterm neonates, specifically increasing the risk for perinatal respiratory depression and the need for neonatal resuscitation in the delivery room. The Cleveland Clinic granted IRB approval to conduct this study.
Materials and methods
This retrospective cohort study was conducted at Hillcrest Hospital, a tertiary care medical facility of the Cleveland Clinic Health System located in Mayfield Heights, OH. Approximately 4500 infants are delivered at Hillcrest Hospital annually. Hillcrest Hospital has 24 hour in house coverage by neonatologists and provides care to preterm and term neonates in a Level III 35-bed NICU. The study involved review of electronic medical records for neonates born between January 2007 and December 2014 at Hillcrest Hospital. The exposed group included neonates of mothers who were treated with SSRIs (citalopram, escitalopram, fluoxetine, fluvoxamine, paroxetine, or sertraline) or venlafaxine during pregnancy. Patients were evaluated for inclusion if the mother received one of the study medications during her obstetric care. Each participant’s obstetric visits for prenatal care, medication histories, and other inpatient notes were reviewed to ensure the neonate was exposed to one of the study medications during pregnancy. The control group included neonates who were not exposed to SSRIs or venlafaxine in-utero and were identified based on similar gestation to exposed infants. Control neonates with a gestational age within the predefined three-gestational week groupings of exposed neonates were selected for inclusion. All controls were selected using a random number table generator.
Study subjects
The study sample was identified through various reports, including patients taking one of the study medications during pregnancy and neonates born at the institution during the evaluation period.
Preterm neonates included those with gestational age 28–36 weeks, and term neonates, defined as gestational age ≥ 37 weeks. Gestational age was taken from obstetric history as it was calculated by ultrasound. Neonates less than 28 week gestation were not included since the majority require respiratory support in the delivery room and after admission to the NICU. Neonates of mothers who received general anesthetic during labor, who underwent treatment with chronic pain medications, or who had a documented substance abuse were excluded. Neonates who were exposed to multiple antidepressants concomitantly were excluded from the analysis.
The primary endpoint of the trial was five-minute Apgar scores. Secondary endpoints included one-minute Apgar scores; oxygen and positive pressure ventilation use in the delivery room; oxygen requirements outside of the delivery room, including duration and type, which was defined as whether or not the neonate required any supplemental oxygen for all neonates and ventilator time and oxygen requirements post-extubation as additional considerations for preterm neonates; hospital length of stay (LOS); birth weight; incidence of persistent pulmonary hypertension of the newborn (PPHN); feeding, including type and time to full feeds; and NICU admission rates for term neonates.
Statistical analysis
We estimated that 99% of term infants and 85% of preterm infants have 5-minute Apgar scores ≥ 7. Therefore, 214 term infants and 214 preterm infants (or 107 in each exposed and unexposed group) were required to detect a difference of 10% in the proportion of infants with Apgar scores ≥ 7 using the Fisher’s exact test, a power of 80%, and a two-tailed alpha level of 0.05. Sample size calculations were performed using G*Power software [25]. Analyses were performed separately for the term and preterm cohorts. In each cohort, control and SSRI-exposed neonates were compared on infant and maternal demographics, clinical characteristics, and outcomes using Kruskal-Wallis, Pearson’s Chi-square, and Fisher’s Exact tests as appropriate.
We used propensity score methods to adjust for baseline differences between the SSRI exposure groups. A propensity score was calculated for each cohort using a multivariable logistic regression model for SSRI exposure predicted by the neonatal factors gender, Caucasian race, delivery type (vaginal, caesarean section, or assisted), year of birth, birth length, birth weight, and gestational age, and the maternal factors number of prenatal care visits (<3 or > = 3), diabetes mellitus, hypertension, preeclampsia, other significant comorbidities, alcohol use, tobacco use, use of potentially harmful medications, antepartum magnesium sulfate, antepartum steroids, age, and parity. The associations between SSRI exposure and postnatal outcomes were assessed using logistic regression models with propensity score adjustment for demographic and clinical characteristics; a second model also adjusted for gestational age. Unadjusted and adjusted odds ratios with 95% confidence intervals were calculated.
We used the Cochrane-Armitage trend test to assess the association between SSRI doses (treated as an ordinal variable) and patient outcomes. All analyses were performed on a complete-case basis and sample sizes reflect missing data. All tests were two-tailed and performed at a significance level of 0.05. SAS 9.3 software was used for all analyses.
Results
A total of 168 neonates were exposed in-utero to SSRIs during the study period. Fifty one of these neonates were pre-term neonates and 117 were term neonates. The most common exposure to SSRIs among all subjects in this study was to Sertraline (55% of preterm and 60% of term SSRI exposed infants). Approximately 10% of infants were exposed to each of citalopram, escitalopram, and fluoxetine; paroxetine and venlafaxine exposures were less common (Table 1).
All SSRI exposed neonates: Type of medication exposure
All SSRI exposed neonates: Type of medication exposure
Values presented N (column %).
Forty-five percent of SSRI exposed pre-term neonates were exposed in all three trimesters, while 25% were exposed only in the first trimester. No subjects were exposed only in the second trimester. Seventy-five percent of pre-term neonate subjects had first trimester exposure, 59% had second trimester exposure, and 71% had third trimester exposure. Descriptive statistics for pre-term neonates including baseline characteristics and outcomes are presented in (Table 2). Pre-term neonates exposed in-utero to a SSRI were more likely to be Caucasian, more likely to have other drug exposures, and had significantly older mothers, compared to pre-term control neonates. Three neonates (too few for statistical analysis) had 5-minute Apgar scores less than 7, all of whom were in the SSRI group. The odds of a 1-minute Apgar score less than 7 was marginally higher in the SSRI-exposed group as well (P = 0.068). The odds of oxygen administration in the delivery room was 4.1 times higher (95% CI: 1.3–13.0, P = 0.018), and the odds of breastfeeding at discharge was only 27% as high (95% CI: 0.09–0.83, P = 0.023) in SSRI-exposed preterm neonates vs. those not exposed to SSRIs after adjusting for baseline characteristics and gestational age (Fig. 1).
Demographics for preterm infants
Demographics for preterm infants
Statistics presented as Median [P25, P75] and N (column %). p-values: a = Kruskal-Wallis test, b = Pearson’s chi-square test, c = Fisher’s Exact test.

Preterm Neonates: unadjusted and adjusted odds ratio for outcomes. Odds ratios and their 95% confidence intervals are represented by circles and lines, respectively. Unadjusted odds ratios and confidence intervals are shown in gray; odds ratios and confidence intervals adjusted for demographic and clinical characteristics including gestational age are shown in black. The 95% confidence interval for the odds ratio of the outcome ‘LOS >14’ is (0.29, 26.7) and has been truncated for display.
Preterm infants exposed to sertraline at higher doses were more likely to have 1-minute Apgar scores of 1–6, significantly more likely to require positive pressure ventilation, and less likely to be breastfed at discharge. Doses over 100 mg daily were associated with poorer outcomes and doses of 150 mg daily were associated with the worst outcomes. The rates of each outcome at each dose of sertraline are summarized in Fig. 3. Data for all other SSRIs were insufficient for a proper analysis.

Term Neonates: unadjusted and adjusted odds ratios for outcomes. Odds ratios and their 95% confidence intervals are represented by circles and lines, respectively. Unadjusted odds ratios and confidence intervals are shown in gray; odds ratios and confidence intervals adjusted for demographic and clinical characteristics including gestational age are shown in black. The 95% confidence intervals for the unadjusted and adjusted odds ratios of the outcome ‘5-min Apgar <7’ are (0.18, 22.4) and (0.11, 62.2) respectively and have been truncated for display.
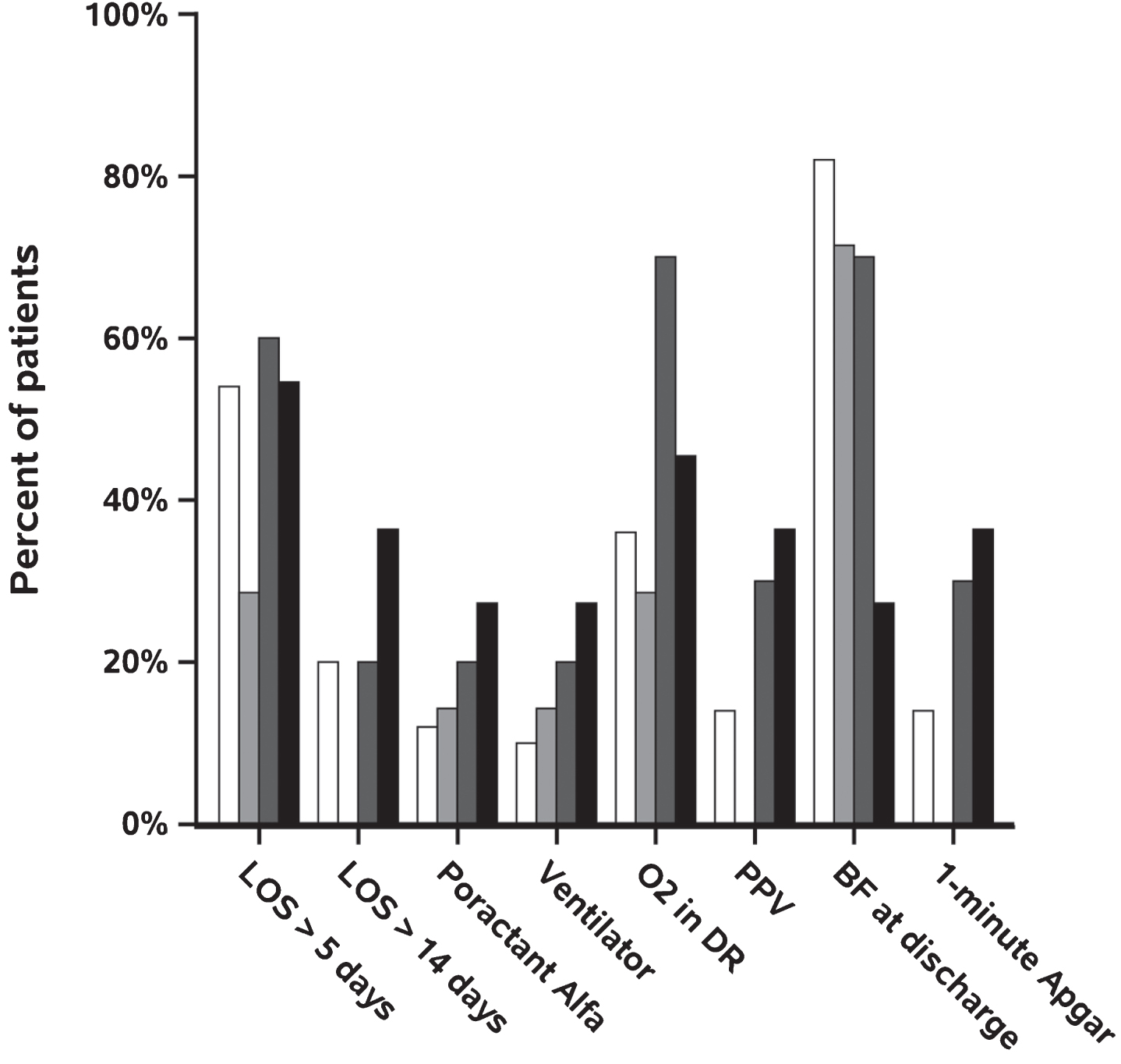
Effect of sertraline dose on preterm neonate outcomes. Outcomes experienced by less than 10 subjects not shown. Dose: Controls (N = 50), white; 1–25 mg (N = 7), light gray; 50 mg (N = 10), dark gray; >50 mg (N = 11), black.
Sixty-one percent of in-utero SSRI exposed term neonates experienced exposure in all three trimesters, while 10% were only exposed in the first trimester, and 9% in the second and third trimesters only. Seventy-four percent of subjects had first trimester exposure, 74% had second trimester exposure, and 84% had third trimester exposure. Descriptive statistics for term neonates, including baseline characteristics and outcomes are presented in (Table 3). Term neonates exposed in-utero to SSRIs were more likely to be Caucasian, have more prenatal care, and were more likely to have other concomitant medications versus term neonate controls. The odds of a lower five minute Apgar score did not differ between in-utero SSRI-exposed neonates and controls. The odds of a 1-minute Apgar score less than 7 was 3.5 times higher (95% CI: 1.04–11.9), P = 0.043) in term neonates exposed to SSRIs in-utero vs. control neonates (Fig. 2). NICU admission was five times higher (95% CI: 1.3–19.0), P = 0.020) in exposed neonates vs controls. The time-to-full-feeds was inconsistent among term neonates exposed to SSRIs vs. control term neonates (Table 5).
Demographics for term infants
Demographics for term infants
*Data not available for all subjects. Missing values: Discharge weight (grams) = 5, Head circumference (cm) = 9, Maternal age (years) = 6. Statistics presented as median [P25, P75] and N (column %). p-values: a = Kruskal-Wallis test, b = Pearson’s chi-square test, c = Fisher’s Exact test.
Preterm infants: Unadjusted, propensity score (PS) adjusted, and PS and gestational age (GA) adjusted odds ratios (OR) for SSRI exposed vs. control on outcomes
Term infants: Unadjusted and propensity score (PS) adjusted odds ratios (OR) for SSRI exposed vs control on outcomes. Note two patients were missing breastfeeding information and 9 were missing time to full feed
Analyses were performed for the subgroup of SSRI patients taking sertraline, separately for the term (N = 70) and preterm (N = 28) cohorts. Data for other SSRI use in term neonates was not sufficient to perform proper analysis. The data for term neonates exposed to sertraline show a significant association between higher sertraline doses (>100 mg) and 1-minute Apgar scores of 1–6. No other associations were significant. The rates of each outcome at each dose of sertraline are summarized in Fig. 4.
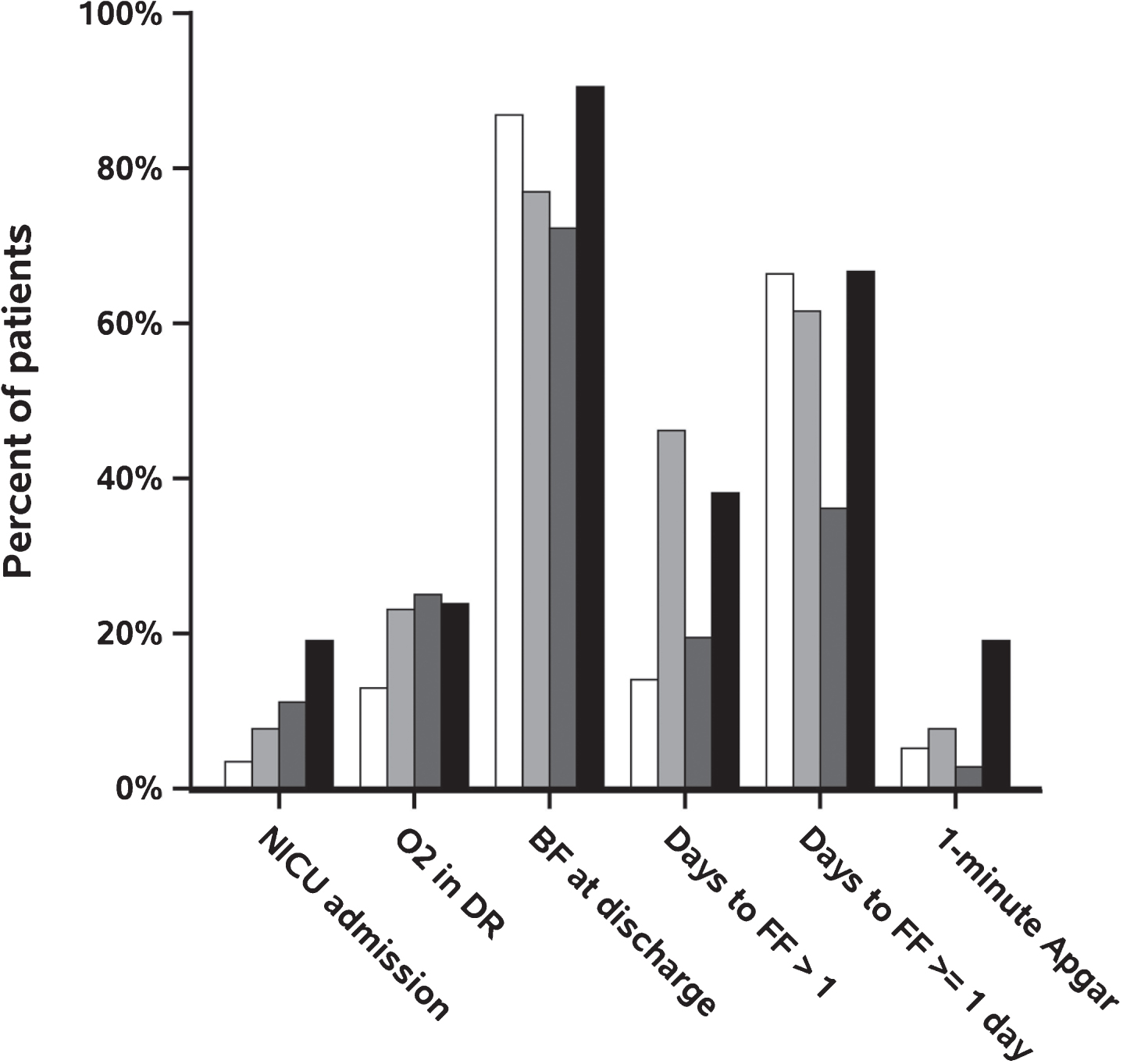
Effect of sertraline dose on term neonate outcomes. Outcomes experienced by less than 10 subjects not shown. Dose: Controls (N = 116), white; 1–25 mg (N = 13), light gray; 50 mg (N = 36), dark gray; >50 mg (N = 21), black.
Depression is a relatively common condition in women of childbearing age. SSRIs and venlafaxine are frequently used in the treatment of depression; therefore, the incidence of fetal exposure to these medications is high [3]. Sertraline comprised the majority of exposures in our cohort which is consistent with prior published recommendations to minimize the risk for cardiac defect and other congenital anomalies [26, 27]. A number of studies have demonstrated low Apgar scores and a higher risk of neonatal adaptation difficulties in full term neonates with in-utero exposure to SSRIs [4, 28–35]. Our primary outcome assessed Apgar scores and the need for respiratory support and resuscitation in the delivery room in both term and preterm neonates. Our results are consistent with the published literature. The odds of a 1-minute Apgar score less than 7 was 3.5 times higher in term neonates and only marginally higher in preterm neonates. Researchers of a prospective cohort trial found significantly lower Apgar scores at 15 minutes of life (p < 0.02) after in-utero exposure to fluoxetine and citalopram [34]. Researchers in a retrospective cohort study assessed Apgar scores after exposure to sertraline, fluoxetine, paroxetine or venlafaxine. Neonates exposed in-utero to these agents had an OR of 2.33 of a lower Apgar score [30]. Casper et al. in a case control study comparing SSRI exposed to non-exposed neonates during pregnancy found that those exposed had significantly lower APGAR scores [23]. Notably all the published studies and our study had low enrollment, thus, further prospective studies and potentially additional meta-analyses are needed to provide an accurate assessment as other studies show either no difference in Apgar scores or no difference in neonatal adaption after prenatal SSRI exposure [28, 36]. Disparities in sample size or under-powering may have contributed to differences in the latter studies.
We are aware of a few studies that provide data on association of SSRI doses with birth outcomes [34, 37–42]. Dosing of medications is a key principle of teratology as demonstrated by a dose stratification study of paroxetine where cardiac malformations were not significant after paroxetine exposure until dose stratifications were performed [38]. Doses of paroxetine >25 mg were associated with congenital malformations. A subgroup analysis of neonates exposed to paroxetine in a larger SSRI exposure study found a correlation between higher paroxetine dose and the presence of neonatal abstinence (NAS)(p = 0.01) [34]. Levinson Castiel et al. were unable to delineate an exact dose where NAS might occur, but NAS didn’t occur in any neonate exposed to less than 20 mg of paroxetine [34]. Neonates with no symptoms, mild symptoms, and severe symptoms received an average of 19 mg, 23 mg, and 27 mg daily, respectively. Roca et al. in a prospective case control study assessed dose effects on neonatal outcomes [39]. Researchers stratified doses as either high (sertraline >150 mg, citalopram >40 mg, escitalopram >20 mg, paroxetine >40 mg, fluoxetine >40 mg, or sertraline >150 mg) or medium to low. Neonates exposed to the high doses of SSRIs had a 5.53 OR (95% CI 1.46–20.93) of preterm birth compared to the low-medium dose exposed neonates, and were significantly smaller in birth weight (p = 0.011). The subgroup analysis for dose was a very small sample (N = 19 in high dose and N = 65 in low-medium dose), but provides insight into how important dosing may be in adverse effects experienced by neonates. Our results are consistent with the findings of these studies. We were only able to analyze a subgroup of neonates exposed to sertraline due to of small sample size. Neonates exposed to doses of sertraline >100 mg daily experienced poorer neonatal outcomes, most notably lower Apgars and also required additional support post-delivery. Doses greater than 150 mg were associated with even more adverse outcomes. We must be cautious with our results due to our small sample size. Further studies are needed to confirm that doses lower than 100 mg sertraline are not associated with poor neonatal outcomes. Additionally, larger subgroup stratification by dose in a large prospective trial may provide evidence of what is the definitive dose where poor neonatal outcomes occur. Our findings of lower Apgar scores and increased need for positive pressure ventilation in preterm at birth underscores the need for appropriately trained staff in neonatal resuscitations when a history of antenatal SSRI exposure is revealed until research is provided for dose stratification. Recently, Nagai et al. explored the potential impact of a pharmacokinetic model to allow paroxetine dose tapering to avoid neonatal toxicity after in-utero exposure [27]. They developed a 5 compartment model for paroxetine to assist in designing a dosage regimen during pregnancy that allowed tapering which avoided toxicity in the neonate. Further pharmacokinetic modeling during pregnancy is needed for all SSRIs to delineate doses that prevent or minimize neonatal toxicity.
The odds of a NICU admission in our study patients was five times higher in the term exposed group. Our finding of increased NICU admissions for term neonates coincides with findings in the literature. Casper et al. in a prospective cohort study of 329 pregnant women on SSRIs, 4902 women not on SSRIs but with a history of psychiatric illness and 51770 women not on SSRIs and without psychiatric history found that SSRI exposure during pregnancy increased neonate NICU admissions [23]. The authors noted that admissions were not attributed to low Apgar scores or gestational age. Several other studies demonstrate similar findings. Interestingly, mothers in our study who consumed SSRIs were more likely to consume alcohol and use tobacco products; however, usage of alcohol and tobacco did not correlate with increased NICU admission.
Finally, term and premature neonates were found to less likely be breastfed at discharge if exposed to an SSRI. Our findings are consistent with the literature which reports feeding difficulty after in-utero SSRI exposure [3]. Several reasons may stem from concern of continued medication exposure through breast milk, latching difficulty, or a discouraged mother.
Our study has strengths and limitations. Its strengths included a study of oxygen requirements of term and preterm neonates in the delivery room, assessment of dose effects of sertraline on neonatal outcomes and control of confounders with statistics which may have prevented bias in our study. We controlled for some of the important confounders such as maternal illness, trimester of exposure, maternal medications, maternal age, nicotine and alcohol use. Researchers in future studies may need to control for maternal weight, socioeconomic status, diet, and illicit drug use, all of which have been confounders in previous research.
Our research was limited by several factors. A retrospective cohort study using chart review is not the strongest study design and our results are only as good as the documentation provided. Even though we deliver about 4500 neonates a year, the time period to perform a prospective study is time and cost prohibitive. Our study provides information to conduct a multi-center prospective study. Second, we were unable to match controls to exposed neonates and we did not match mothers with psychiatric illness on an SSRI with mothers with psychiatric illness but not on an SSRI; however, we attempted to mitigate this by conducting a multivariate regression and by utilizing propensity scoring. Third, it is difficult to ascertain the effects observed and the cause: the medication or a medical condition. This raises the following question: does the neonatal outcome relate back to the acuity of illness of the neonate or to the severity of maternal depression? Future studies may provide further insight. Fourth, although we observed positive associations with higher sertraline doses and neonatal outcomes, our N was very small and no further information was provided for other SSRIs. A large prospective study assessing dose stratifications and neonatal outcomes as well as pharmacokinetic models to direct dose tapers are needed. Finally, we did not meet power in the preterm group; however, oxygen utilization in the delivery room in SSRI exposed neonates still reached statistical significance in this subset of patients. This result provides data for future research into neonate oxygen requirements in the delivery room and immediately post admission to a NICU.
Conclusion
Term and pre-term neonates exposed in-utero to SSRIs experienced significantly worse outcomes after adjusting for baseline differences. Adjusted odds ratios that were not statistically significant tended to indicate better odds of outcomes in the non-exposed groups. The predominance of treatment with sertraline and treatment times across all three trimesters limits our ability to statistically compare medication and exposure time outcomes. This study provides evidence that SSRI exposure in-utero may lead to increased neonatal resuscitation requirements in the delivery room as well as lower Apgar scores. Future research is required for SSRI dosages to provide specific doses that lead to poor neonatal outcomes.
Conflict of interest
The authors declare no conflict of interest.