
Abstract
Background
There are variations in practices regarding the initiation and stopping of caffeine for apnea of prematurity among neonates above 28 weeks.
Objective
To estimate the proportion of recurrence of apnea of prematurity among neonates between 28 and 32 weeks on stopping caffeine after an apnea-free period of 7 days.
Methodology
This was a prospective, observational study conducted in a tertiary care government medical college from April 2023 to May 2024. Study population were neonates between 28 and 32 weeks gestation. Injection Caffeine citrate was started for all within 2 hours of birth and it was stopped after an apnea-free period of 7 days.
Results
Out of the total 300 neonates enrolled, 285 were available for primary outcome analysis. Out of the 38.2% (n = 109) who developed recurrence of apnea, only 11.9% (CI: 8.4%–16.3%, n = 34) was due to apnea of prematurity. Late-onset sepsis was the major cause in the rest. The median day of recurrence was 7 days (IQR 3) after stopping caffeine. On multivariable logistic regression birth weight less than 1250 g was the only significant predictor for the recurrence.
Conclusion
The incidence of recurrence of apnea of prematurity was only 11.9 % (CI 8.4%–16.3%) among 28–32 weeks babies on early stopping of caffeine. For judicious use of caffeine, considering its cost and side effects, it may be reasonable to stop it after an apnea-free period of 7 days. Close monitoring is required for 7–10 days in babies less than 1250 g.
Keywords
Introduction
Cessation of airflow is called apnea and when it is accompanied by bradycardia (heart rate <100 beats per minute), hypoxemia (detected clinically by cyanosis or SpO2 <80% on saturation monitoring), hypotonia or pallor, it is considered as pathological (also called apneic spell). 1 Preterm infants (<37 weeks) are more prone to apnea due to the developmental immaturity of their respiratory centers, and that is called apnea of prematurity (AOP). The incidence of AOP is inversely related to gestational age and birth weight. Seven percent of neonates born at 34 to 35 weeks gestation, 15% of those between 32 and 33 weeks, 54% of those between 30 and 31 weeks, and nearly all infants born at <29 weeks gestation or <1000 g (ELBW/extremely low birth weight) exhibit AOP. 2 In most cases, AOP resolves by 34–37 weeks of postmenstrual age in infants born at 28 weeks but has been recorded up to 43 weeks of post menstrual age. 3 For many years, methylxanthines have been the mainstay of pharmacologic care for AOP, both in prevention and treatment. Caffeine citrate is chosen over theophylline in this group due to its longer half-life, greater therapeutic index, and absence of the requirement for drug-level monitoring. 4 The Caffeine for Apnea of Prematurity (CAP) study confirmed that caffeine in the standard dose of 20 mg/kg loading with 5–10 mg/kg day maintenance for infants <1251 g coming off mechanical ventilation, or being treated for apnea, resulted in less need for respiratory support, subsequently less BPD, and long-term follow up also showed improved neurodevelopmental outcomes. 5 In the CAP trial, caffeine therapy was initiated at a median of 3 days (IQR, 2–5) and permanently discontinued at a median postmenstrual age of 34.4 weeks (IQR, 33.0–35.9). 6 There has been a trend in recent years toward starting caffeine within the first 1–2 days of life, and as early as in the delivery room.7,8 The gestational age at which caffeine should be started for prophylaxis varies between guidelines. In a recommendation by Schmidt B et al. in 2014 very-low-birth-weight (VLBW) infants should only be considered for caffeine therapy soon after birth if they are extremely immature and receive positive airway pressure without an endotracheal tube or are weaning from mechanical ventilation toward a trial of extubation or have documented apnea. 7 According to NICE guidelines (2019) it was recommended as appropriate to start caffeine citrate in babies born at or before 30 weeks (equivalent to babies born at or below 1250 g) on admission to the neonatal unit. 8 According to the New World Health Organization recommendations (2022) for care of preterm or low birth weight neonates, caffeine for prevention of apnea may be considered in preterm infants <34 weeks of gestation, based on low certainty evidence. But as the chance of apnea decreases beyond 32 weeks, clinical practices vary, and in the majority of the units, it is considered only when there are symptoms of AOP.
The postmenstrual age at which apnea resolves increases with decreasing gestational age at birth.9,10 This natural history, as well as between-patient variability at comparable gestational ages, mandate that decisions to start and stop caffeine therapy be individualized. 11 While some units prefer to continue caffeine for a longer duration, till infants are 34–35 weeks PMA or beyond, others try to stop caffeine early, as soon as infants attain 7 apnea-free days.12,13 Longer-duration caffeine therapy has more side effects (feed intolerance, tachycardia, dysrhythmias, seizures, increased metabolic demand leading to diminished preterm growth, etc.), more cost, and has a prolonged hospital stay.14–16 No universal consensus or no major Randomized controlled trials (RCT) have been published on this area.
Hence, this study was planned to estimate the proportion of recurrence of AOP among neonates between 28 and 32 weeks on stopping caffeine after an apnea-free period of 7 days and also to study the predictive factors associated with its recurrence.
Methods
This was a prospective, observational study (registered under the Clinical Trials Registry of India no. CTRI/2023/09/057347) conducted in a tertiary care NICU of a government medical college over a period of 1 year from April 2023 to March 2024 after getting human ethical committee clearance. All inborn preterm neonates of gestation between 28 and 32 weeks whose parents have consented for the study and not having any major congenital anomaly were included. The sample size was calculated based on a study by Raj et al. 17 In that study on 60 neonates, the proportion of clinically significant apnea after early stopping of caffeine was 15%. We assumed a proportion of 25%, with precision of 20%. Hence, with 80% power and an alpha error of 5%, the sample size calculated was 300. Caffeine citrate was administered at a loading dose of 20 mg/kg intravenously, followed by a 5 mg/kg maintenance dose for all babies less than 32 weeks. Caffeine was stopped after 7 days of apnea-free period if the baby was out of respiratory support at that time. The proportion of neonates with recurrence of clinically significant apnea (CSA) were analyzed, and caffeine citrate was restarted in them and continued after ruling out secondary causes of apnea. If secondary causes were found, caffeine was not continued. CSA was defined as a drop in saturation to ≤80% and any one of the following like decrease in heart rate to <100/min, or poor respiratory effort requiring PPV, or a need for o2 supplementation, HFNC, CPAP, or Mechanical ventilation, or restart of caffeine therapy by the clinical team or intermittent hypoxic spell >10/day (spo2 <90 even without bradycardia).1,9,18 Babies were monitored with Masimo pulse oximeter, and doctors on duty evaluated for the CSA. Secondary causes were evaluated with blood investigations, ultrasound, lumbar puncture, or nasopharyngeal swab for viral studies according to the history and clinical findings.
Statistical analysis
Data was entered in Microsoft Excel and was analyzed using SPSS-27. Frequency was noted as numbers and percentages among categorical variables. The percentage with a 95% confidence interval was calculated for the primary outcome variable. Mean with standard deviation or median with IQR was used for continuous variables, depending on the normality of the data. The comparison of continuous variables was done using t test and Mann–Whitney U test according to the normality of the data. Chi-square or Fisher Exact test was used, wherever applicable, to find out the significance of association. The strength of association was calculated with relative risk and its 95% confidence interval. A p value of < .05 was considered significant throughout the analysis.
Result
Baseline characteristics of the study population (n = 300).
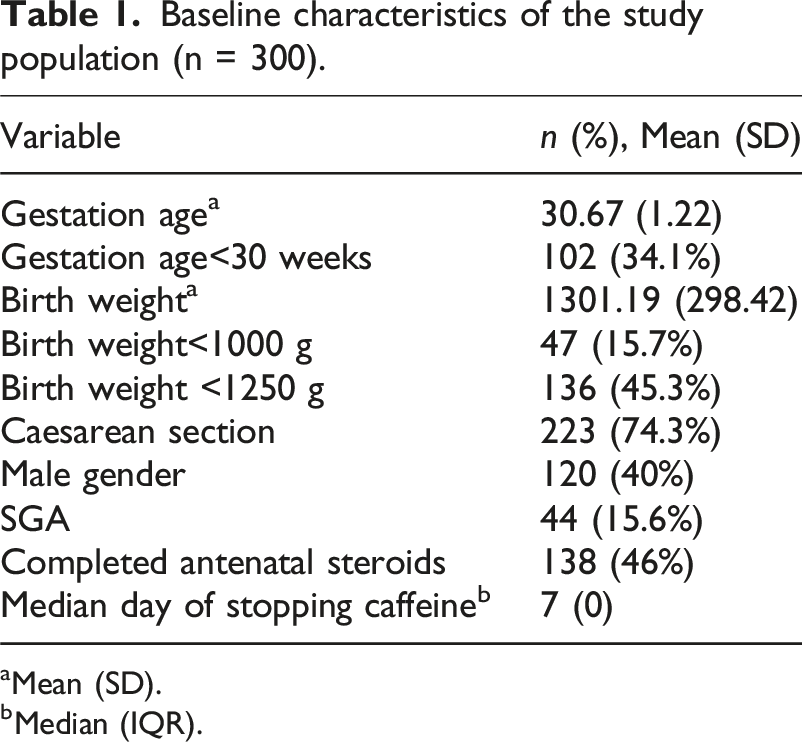
aMean (SD).
bMedian (IQR).

Flow chart showing patient selection process and outcome analysis.
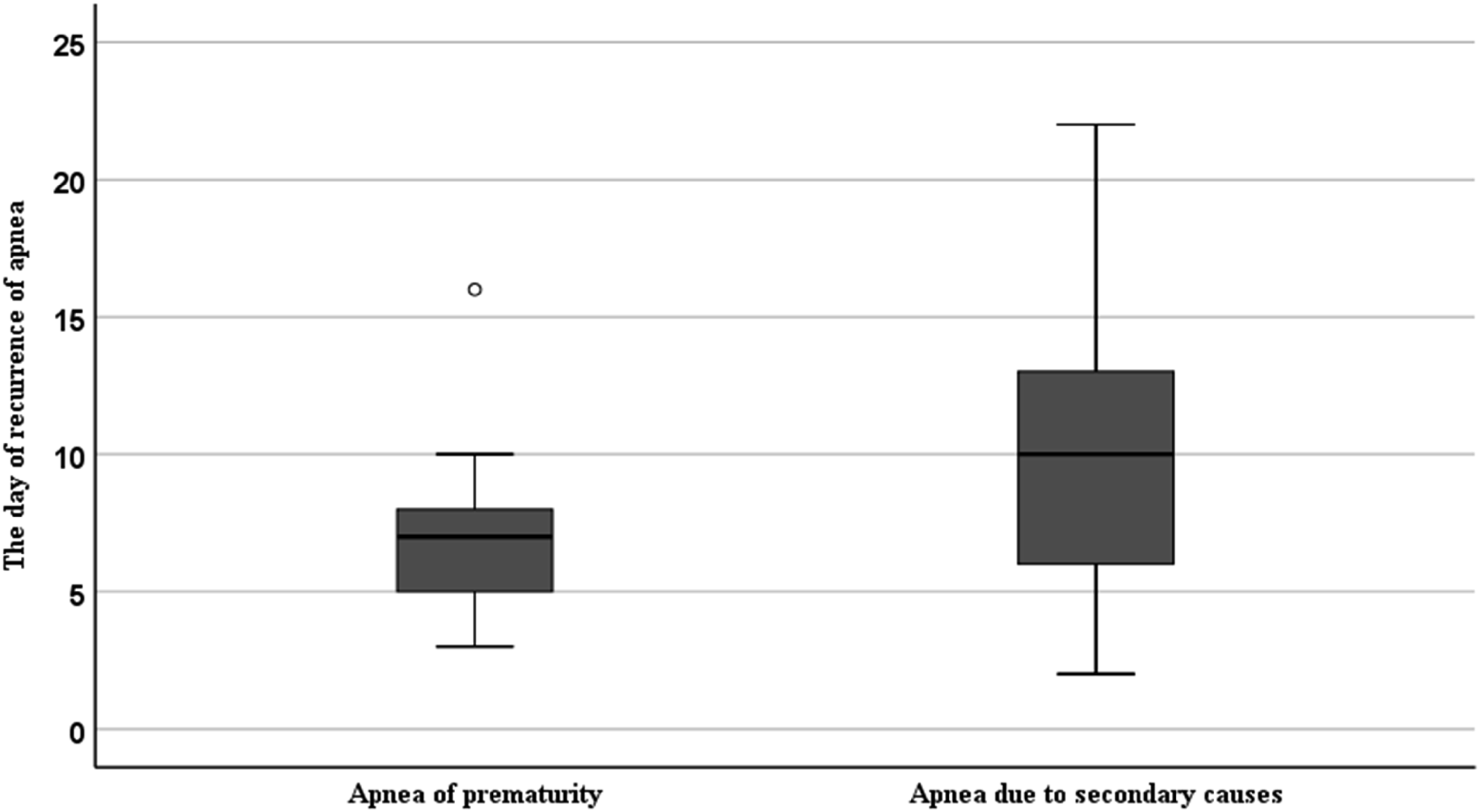
Among 285 neonates, we could attempt stopping caffeine on 7th day in 77.5% of cases (n = 221). The maximum day of first try of stopping was 19 days. Though 38.2% (n = 109) developed recurrence of apnea on stopping caffeine citrate, only 11.9% (CI 8.4%–16.3%, n = 34) had AOP. Rest 26.32% (n = 75) had apnea due to secondary causes. The possible causes were as shown in Figure 2. The median day of recurrence of apnea after the first attempt of stopping caffeine in neonates with AOP was 7 days (5,8 & IQR 3), but apnea occurred as early as 3 days and as late as 10 days of stopping caffeine (Figure 3). In cases with apnea due to secondary causes, the apnea recurred as early as 2 days and as late as 22 days with a median day of 10 (6,13 & IQR 7). Comparison of the postnatal day and corrected gestational age (CGA) at which the first attempt of stopping caffeine was made, between those with and without recurrence of apnea of prematurity (AOP), was as shown in Table 2. Bar Chart showing the secondary causes for apnea recurrence. Box and whisker plot showing the comparison of the day of recurrence of apnea after the first attempt of stopping of caffeine in neonates with apnea of prematurity and apnea due to secondary causes. Comparison of the postnatal day and CGA of first attempt of stopping between babies who had the recurrence and nonrecurrence of AOP. *t value.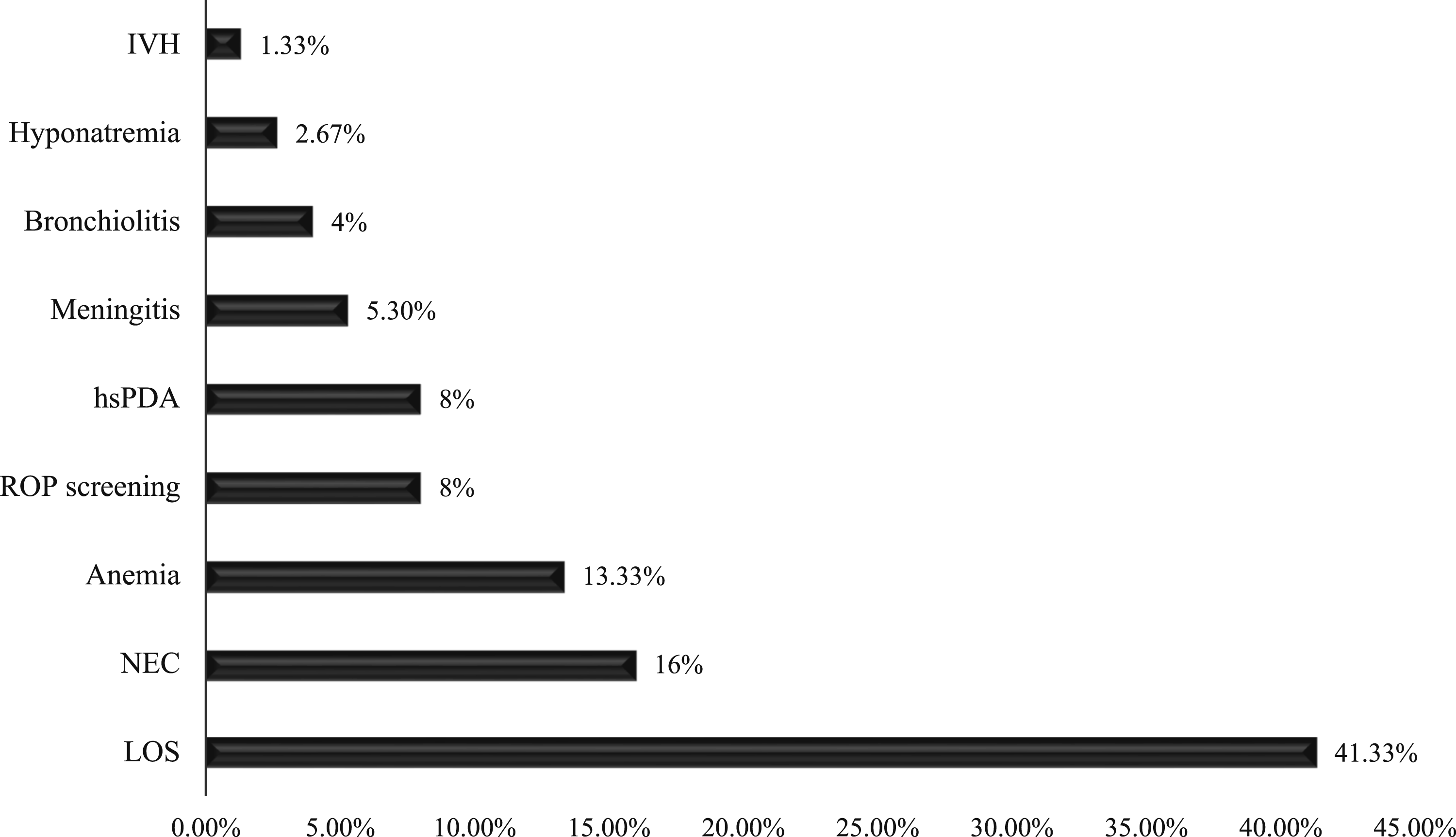

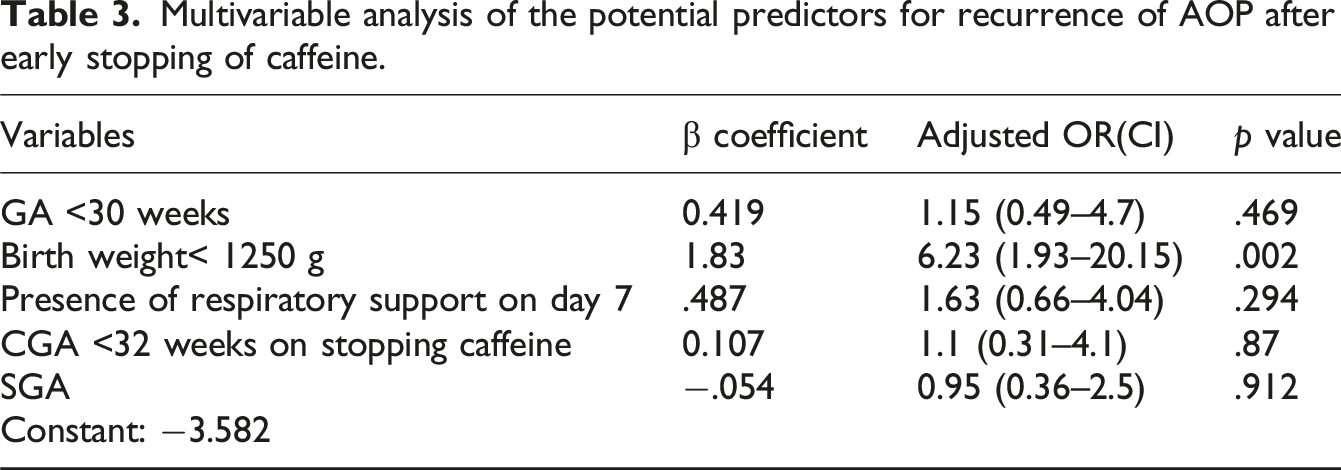
Multivariable analysis of the potential predictors for recurrence of AOP after early stopping of caffeine.
While comparing the anthropometric parameters at discharge, there was no statistically significant difference in weight or length at discharge between neonates who restarted and not restarted on caffeine (1620.59 vs 1681.30 g and 42.82 vs 43.23 cm). Though there was a statistically significant difference in head circumference of 0.54 cm (29.2 vs 29.74 cm), the clinical significance needs to be assessed on follow up.
Discussion
In this study among neonates less than 32 weeks, excluding extreme preterm, caffeine was stopped after an apnea-free period of 7 days if the babies were no longer on respiratory support on that day. Among 300 neonates, 73% (n = 219) never had apnea in the initial 7 days and the first attempt of stopping caffeine was done on day 7. Around 53% among neonates <30 weeks and 12.74% among 30–32 weeks had apnea in the first week of life. Above 32 weeks till 32 weeks 6 days, 4.8% had apnea in the first week. The maximum day at which the first try of stopping caffeine done was 19 days. Though 38.2% (n = 109) neonates developed recurrence of apnea on stopping caffeine after an apnea-free period of 7 days, on further evaluation it was identified that in only 11.9% (CI: 8.4%–16.3%, n = 34) it was due to AOP. Rest were due to secondary causes and in majority it was due to LOS (Figure 2), followed by NEC and anemia. So, there was no need to continue caffeine till 34 weeks of CGA for the remaining 88.1% of the neonates in this age group. Around 1/4th of neonates <30 weeks (22.8%, n = 21) and 1/4th (23.6%) of neonates less than 1250 g had recurrence of AOP. In above 30 weeks only 6.7% and in above 1250 g only 3.1% had recurrence of AOP after this early stoppage. In a study done by Pergolizzi et al., 19 the incidence of AOP was inversely related to the gestation age and it was 54% between 28 and 30 weeks and it was 15% between 30 and 32 weeks. It is almost similar to the incidence in our study. So, it may be reasonable to discontinue caffeine after an apnea-free period of 7 days in those above 30 weeks and those above 1250 g. This also can be followed in neonates above 28 weeks under close monitoring. In one reported RCT from south India by Raj et al. comparing the short course (7 days of apnea-free period) versus longer-duration caffeine therapy (till 34 weeks of PMA) among 60 neonates, the proportion of significant apnea in two groups were almost similar (15% vs 13%). 17 Lorch et al., in a retrospective cohort study of 1400 infants less than 34 weeks, reported that an event-free interval of 5–7 days successfully predicts the resolution of apnea in 94 to 96% of cases. 20 Secondary causes like late-onset sepsis (41.33%), anemia (13.33%), and NEC 12 (16%) were the major contributors for recurrence of apnea. Other causes included screening procedure for retinopathy of prematurity (ROP), hyponatremia, meningitis, bronchiolitis and anemia. In a study published by Stark AR et al. in 2017, 14 sepsis (19.6%) and NEC (7.6%) were major contributing factors for recurrence of apnea.
The mean corrected gestational age (CGA) of stopping caffeine was 32 weeks (SD: 1.09). The mean CGA on stopping caffeine in those who did not have the recurrence was closely to 32 weeks comparing to those who had the recurrence (in them it was 31 weeks and 2 days). So, it is safer to stop towards completion of 32 weeks. The median day of stopping caffeine was 7 days in those who did not have recurrence compared to 8 days in others. Those who do not have even a single episode in first week may not have the recurrence of AOP than who had at least one episode.
On comparison of baseline and clinical characteristics among babies in whom there was recurrence of AOP versus nonrecurrence, gestational age less than 30 weeks (RR: 3.39, C.I. 1.78–6.46), birth weight less than 1250 g (RR: 7.64, CI 3.05–19.16), CGA on stopping caffeine less than 32 weeks (3.5 (1.65–7.5)) and the need for respiratory support on day 7 (RR: 3.73, CI 2.01–6.9) had a significant association with the recurrence of AOP. ANS coverage, SGA, and gender had no significant association. But after multivariable logistic regression analysis, to adjust for the confounders, the only independent predictor for the recurrence of AOP was birth weight less than 1250 g. Birth weight <1250 g had an increased odds of 6.23 for the recurrence of AOP in these babies. In an RCT by Raj et al. 17 among early stopped caffeine group, chances of recurrence of apnea was more with a birth weight of <1246 g.
The median day of recurrence of AOP was 7 days after stopping caffeine with the minimum day of 3 days and recurrence was seen as late as 10 days (Figure 3). This may be due to the physiological variability in the half-life of caffeine in the neonates. But for one case, the recurrence was seen as late as 16 days and no secondary causes was found. So, after stopping caffeine the period of observation may be extended up to 10 days for a safer discharge.
There are not much reported studies on this aspect. Though this was not an RCT, it was a prospective observational study with adequate sample size and included an adequate number of neonates less than 30 weeks too. Babies were monitored continuously in NICU or special newborn care unit (SNCU) with monitors for 7 days of stopping caffeine. But after that majority of the babies were with mothers in special wards without monitors and apnea was reported from there by the mother. Also this study has the limitation of a single center observational study.
To conclude, in this study, the incidence of recurrence of AOP was only 11.9 % (CI 8.4%–16.3%) among 28–32 weeks babies on stopping caffeine following an apnea-free period of 7 days. For judicious use of caffeine, considering its cost and side effects, it may be reasonable to stop it after an apnea-free period of 7 days. But closely monitor babies <1250 g or less than 30 weeks for as long as 10 days for the recurrence of apnea. There was less chance of recurrence of AOP if the baby had no apnea in the initial 7 days and the stopping caffeine was towards 32 weeks of CGA. But the decisions should be individualized based on the monitoring capacity and the workload of the unit.
Key messages
What this study adds?
• Caffeine may be stopped early if apnea free for 7 days in neonates above 28 weeks. • Should monitor babies for recurrence of AOP till 10 days after stopping caffeine.
Footnotes
Authors’ note
Presented a part of this work for award paper Category at Kerala Neocon 2024 on 18th May.
Acknowledgment
We sincerely thank Dr Prakash Duraisamy, Dr Meghna Nema, and Dr Aishwarya Venugopal, senior residents in Neonatology department for their constant mental support and scientific suggestions offered throughout the study.
Ethical considerations
Human Ethics Committee, Medical College, Thiruvananthapuram. Permission Number: HEC: 02/08/2023/MCT in place of 02/08/2022.
Consent to participate
We authors certify that we have obtained all appropriate patient consent forms. The parents understood that their baby’s name and initials will not be published and due efforts will be made to conceal their identity.
Author contributions
Each author contributed sufficiently for the concepts, design, data analysis, interpretation, manuscript drafting & critical revision of the manuscript for important intellectual content and final approval of the version to be published. First author has done the data acquisition. All authors can be the guarantor of this work.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Clinical trial registration
CTRI/2023/09/057347.