
Abstract
Congenital mesoblastic nephroma (CMN) is the most common renal tumor of infancy; however, it occurs infrequently with an incidence of 1 : 125,000. The cellular and classical variants are the most common subtypes of tumors, with a mixed variant occurring infrequently. We describe two cases of mixed variant CMN, which presented within days of each other differing in their clinical behavior. The first case followed a typical course, previously described in the literature, while the other deviated significantly. Traditionally, CMN presents as large abdominal mass in the neonatal period associated with a paraneoplastic syndrome, which can result in hypertension or hypercalcemia. Surgical resection is curative in most cases and long-term prognosis is excellent. Hypertension rarely persists after removal of the tumor, but remained in one of our two patients.
Abbreviations
neonatal intensive care unit
positive pressure ventilation
congenital mesoblastic nephroma
appropriate for gestational age
blood pressure
magnetic resonance imaging
vanillylmandelic acid
homovanillylmandelic acid
blood urea nitrogen
creatinine
twice daily
Patient one
A 39.1 week infant delivered at a community hospital via spontaneous vaginal delivery was noted to have a large, palpable, right sided abdominal mass resulting in intermittent tachypnea. The discovery of the abdominal mass was a surprise to the delivery team as the mother, a 27 years old G2 P2 African American female, had good prenatal care and normal ultrasounds, with no signs of increased amniotic fluid or abdominal masses. All maternal labs were negative and she denied any medication or drug use during pregnancy. The infant, weighing 3491 grams, was appropriate for gestational age (AGA) and required normal resuscitation, Apgar scores were 9 and 9 at one and five minutes, respectively. After palpation of the mass on physical exam, ultrasound and abdominal x-rays were performed.
On the second day of life, infant was transferred to Kentucky Children’s Hospital for further management. Upon arrival to the NICU, the infant was noted to be hypertensive the majority of the time, with intermittent periods of normal blood pressure (BP), via non-invasive monitoring with blood pressures of 60–130/30–90 mmHg, mean arterial pressures 40–100 mmHg, requiring multiple doses of hydralazine. Anti-hypertnesives were administered over the next seven days, ultimately requiring a combination of hydralazine and labetalol for blood pressure control.
A babygram revealed a normal thorax, with bowel displaced to the left side of the abdomen (Fig. 1). An ultrasound of the abdomen determined the right sided mass to have an encapsulated solid, cystic, and vascular components without involvement of the adrenal gland or liver. The left kidney was unremarkable. Laboratory studies revealed normal alpha fetal protein (30883 ng/mL), urine vanillylmandelic acid (VMA) (6 mg/gram cr) and homovanillylmandelic acid (HVMA) (11.3 mg/gram cr) levels. Renal function panel showed normal creatinine (0.34 mg/dL) and BUN (3 mg/dL). MRI of the abdomen showed a large 8.1 cm×6.8 cm×7.7 cm mass draped around the right kidney with slight ureter dilation (Fig. 2A, 2B). Blood vessels were seen entering the mass and no central enhancement was noted, the remainder of the abdomen was normal, including left kidney.
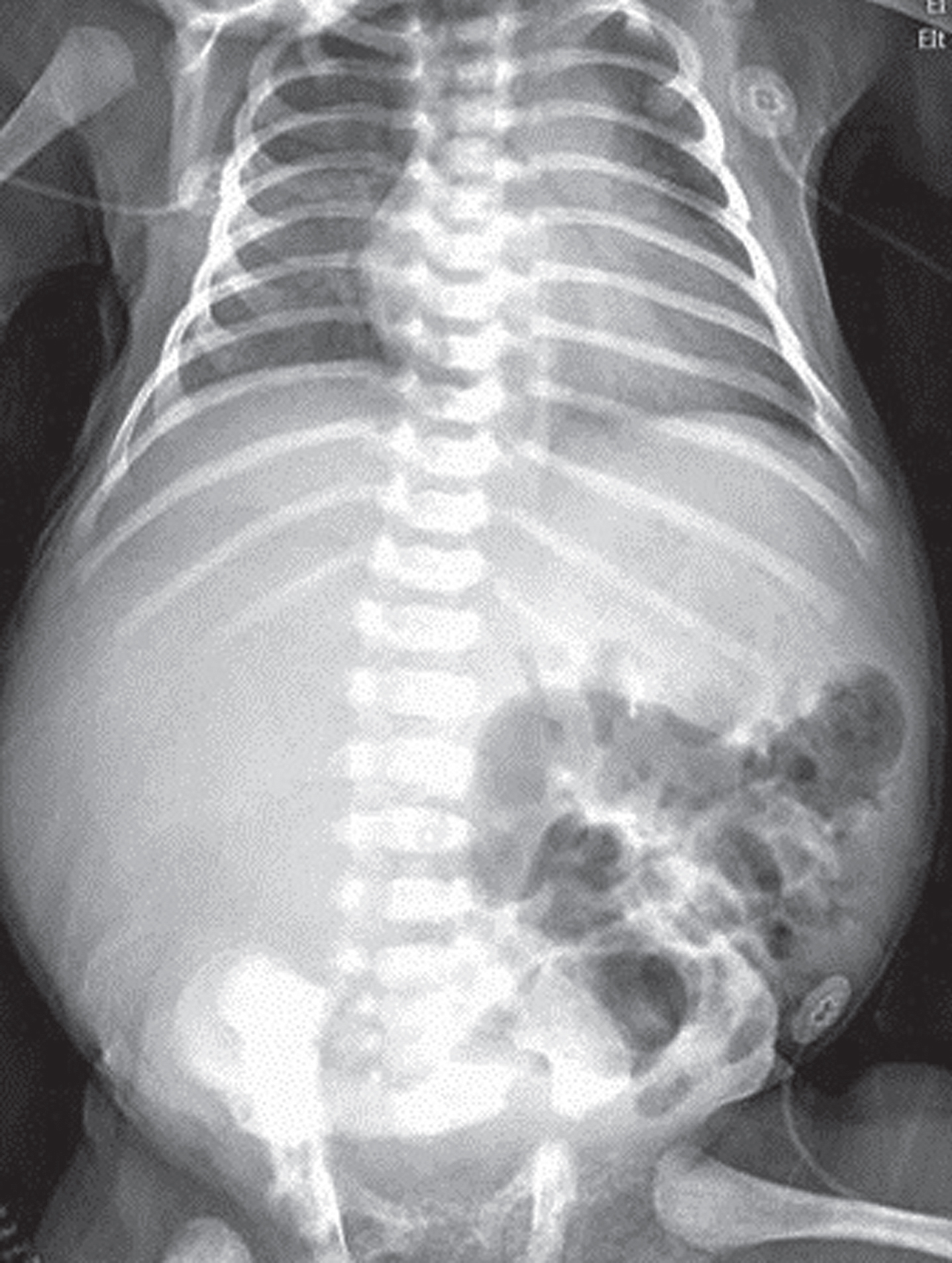
Initial Babygram upon arrival to NICU. Multiple areas of diffuse haziness, consistent with atelectasis. Bowel gas pattern is located only in the left hemi-abdomen, due to large abdominal mass on the right side.
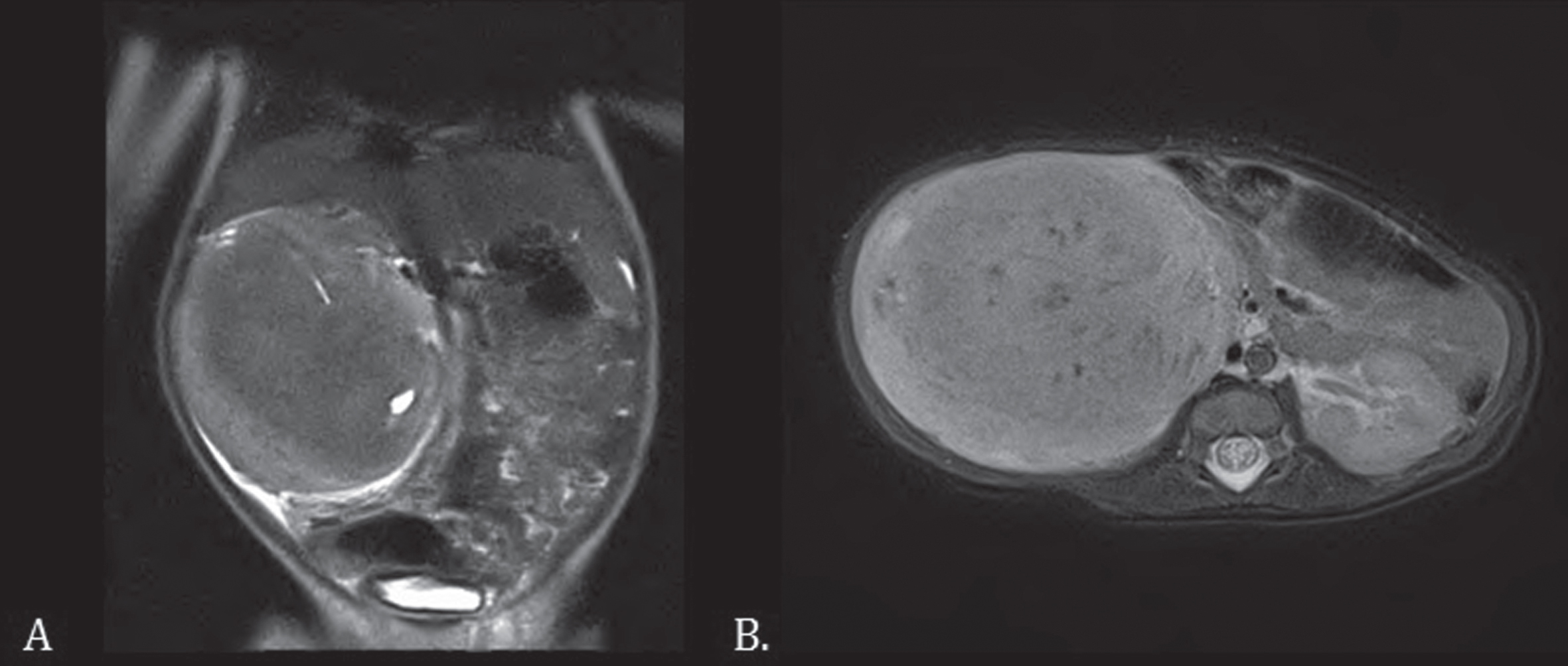
Coronal and axial MRI images with and without contrast for infant presenting with abdominal mass and hypertension. Patient One’s Coronal (A) and Axial (B) MRI T2 weighted images showing large heterogeneous mass that envelopes the right kidney without mass effect, with increased signal intensity around the periphery as compared with central region.
On day of life seven a radical right nephrectomy with paraaortic and paraclavical node dissection was performed, which resulted in complete gross resection. Pathologic evaluation showed a Stage II, mixed type CMN, measuring 8 cm×7 cm×6.5 cm with clear surgical margins, no lymphvascular involvement (Fig. 3A, B, and C). Immediately following removal of the mass, the infant’s hypertension began to subside. However, on day of life twelve his blood pressure began to intermittently increase yet again, which prompted treatment with hydralazine. Despite these measures the hypertension continued to worsen requiring the addition of amlodipine BID dosing that achieved optimal control. He was then discharged home on the same amlodipine dose.
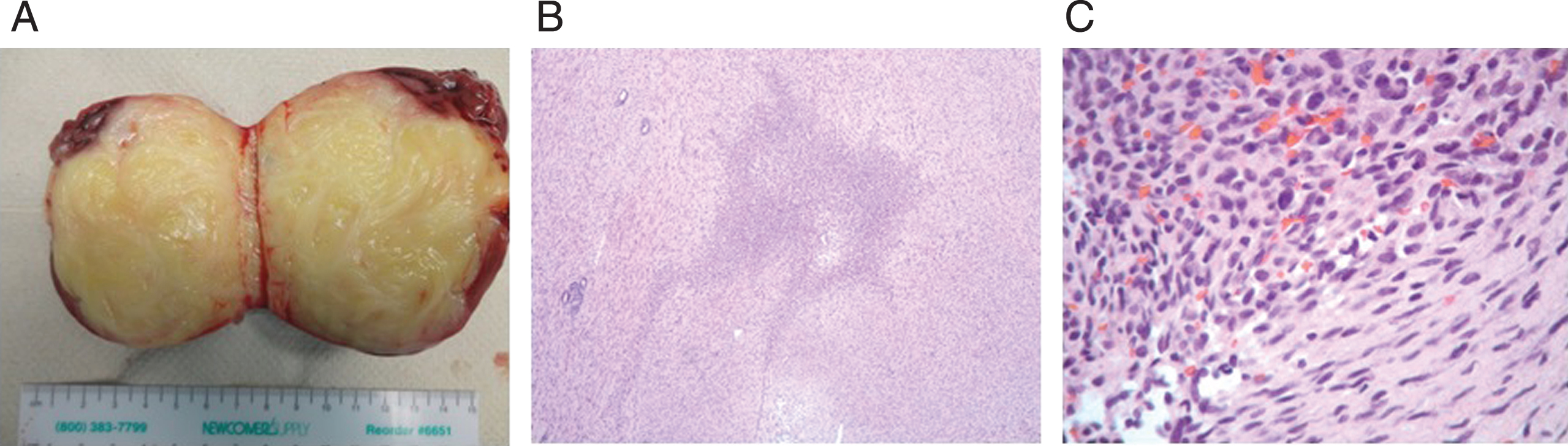
Gross and microscopic evaluation showed elements of both classical and cellular CMN variant, consistent with mixed type. A. Right kidney compressed by large well-circumscribed yellow homogenous whorled mass measuring 8×7×6.5 cm, 216 grams. B. & C. Congenital mesoblastic nephroma, mixed subtype, demonstrating adjacent classic and cellular components (B: H&E 4X, C: H&E 40X).
A 32 year old G2P1 African American female presented to the University of Kentucky high risk obstetrical service with severe polyhydramnios at 33 weeks gestation. An ultrasound at that time lead to the diagnosis of a large abdominal mass and the mother was expectantly managed for the next week prior to delivery. At 34.1 weeks gestation, a 2475 gram, AGA infant, was delivered via emergent C-section for worsening pre-eclampsia and maternal pulmonary edema. Upon delivery, the infant was blue, limp, and had no respiratory effort. He had minimal response to non-invasive positive pressure ventilation (PPV) and was intubated in the delivery room. Despite intubation his chest rise was poor, secondary to the large abdominal mass which appeared to be interfering with diaphragmatic movement.
On admission to the NICU, the baby’s physical exam was remarkable only for decreased breath sounds, specifically on the left side, and a large protuberant abdomen. A babygram was performed to evaluate the chest and the abdomen, given findings on physical exam. It showed bilateral ground glass opacities consistent with surfactant deficiency and he received one dose of surfactant. Additionally, a large radiodense mass was noted on the left side of the abdomen (Fig. 4). Despite surfactant administration, he remained difficult to ventilate, with poor chest wall movement on the left side, limited by the intraabdominal mass. Non-invasive BP tracings showed mild hypertension (81 mmHg/44 mmHg), with mean pressure of 58 mmHg. He received multiple doses of hydralazine, our institution’s first line agent for neonatal hypertension, over the first few days of life to control his BP.

Initial Babygram immediately upon admission to NICU. Significant opacification most likely represented atelectasis is noted on the left hemithorax. The left-hemi abdomen is protuberant and the bowel is located only in the right hemi-abdomen.
A renal ultrasound showed a large heterogeneous mass lesion involving the lower pole of the left kidney, measuring 7.5 cm×7.3 cm×7.0 cm in size resulting in moderate hydronephrosis. The right kidney was unremarkable. Laboratory studies showed elevated creatinine (0.81 mg/dL) and BUN (19 mg/dL). Homovanillylmandelic acid and urinary catecholamines were within normal limits. MRI revealed a heterogeneous, well circumscribed mass originating from the left kidney measuring 8.2 cm×7.3 cm×8.3 cm (Fig. 5A, B), without local tissue invasion. The right kidney, again, was described as normal in appearance.
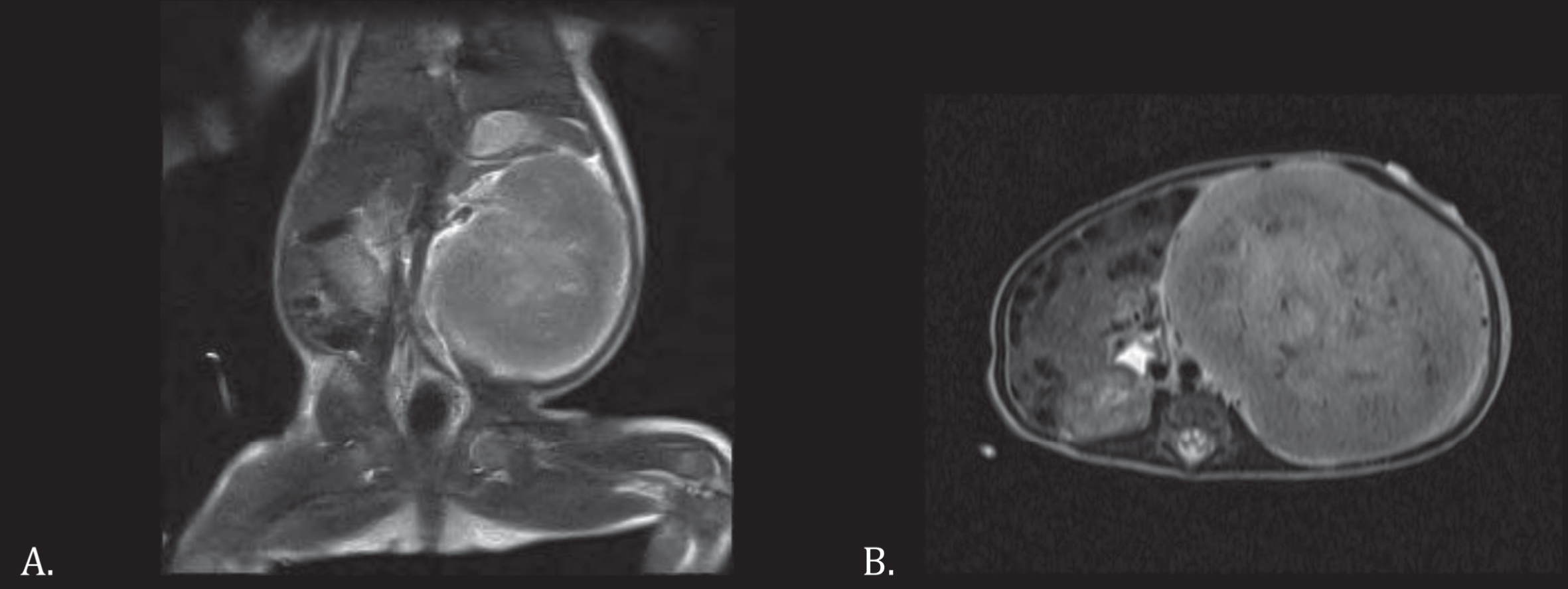
Coronal and axial MRI images with and without contrast for infant presenting with large abdominal mass. Patient Two’s coronal (C) and axial (D) T2 weighted images showing large heterogeneous enhancing mass well circumscribed edges, without invasion of adjacent structures.
Resection of the mass occurred on day three of life via a radical left nephrectomy, also with complete gross resection. Pathologic evaluation of the mass identified mixed type CMN (Fig. 6) without lymph node or extra-renal metastasis. Unlike the first patient, this infant developed refractory hypotension requiring aggressive fluid resuscitation and ionotropic support. Stress dose hydrocortisone was required to achieve normotension. His dopamine was discontinued on day seven of life, and steroids were discontinued on day of life sixteen. His BP remained stable through the remainder of his hospitalization and he was discharged home on day twenty eight of life without blood pressure medications.

Pathologic evaluation showed mixed type variant with elements of both classical and cellular CMN types. A. Left kidney with a thin rim of renal hilum adjacent to yellow, whorled mass measuring 8.5×7.9×6.7 cm, 242 grams. B. Classic variant components with fascicles of bland spindled myofibroblasts, collagen fibers and rare mitoses (H&E, 10x) C. Cellular variant component with plump, rounded nuclei, dense cellularity and increased mitotic activity (H&E, 20x).
In addition, this infant’s hospital course was also complicated by persistent direct hyperbilirubinemia (4.7 mg/dL), detected on day sixteen of life. The levels peaked on day 17 (5.9 mg/dL) and remained elevated on the day of discharge (3.8 mg/dL). Ursodiol was started on day sixteen of life and discontinued at discharge. A complete hepatic work up including ultrasound, liver function test, and a HIDA scan were unremarkable. Gastroenterology consultation was obtained and no specific etiology elucidated.
We have presented two cases of CMN which were admitted to our facility during a two week span, which is itself, extremely rare. While CMN is the mostcommon renal tumor in newborns, they remain extremely rare, with an incidence of 1 in 125,000 in children less than fifteen years of age [1, 2]. Nearly 80% of all CMNs occur during the neonatal period, and tend to have a slight female predominance, 1.5 to 1 [1].
CMNs are currently classified into one of three distinct categories. These categories play a major role in determining therapy and prognosis. The most common type of CMN, accounting for 66% of cases, is the cellular type [1, 3]. This type has the highest risk of undergoing malignant transformation and metastasizing after surgical resection. Goss pathological evaluation of these tumor shows that they tend to be soft, have a large cystic component, and multiple areas of hemorrhage within the tumor [4]. When examining these tumors on a micro-anatomical level, the reason for their propensity to become malignant and metastasize becomes evident. These tumors are made up of large numbers of highly mitotically active cells, small amounts of stroma, and a large nucleus to cytoplasmic ratio [3, 4].
The classic type, which occurs less frequently making up 24% of cases of CMN, has a very low risk of recurrence or malignant transformation [1, 2]. This is reflected on histological examination, as these tumors tend to be composed of cells that are significantly less mitotically active [5]. On gross examination these tumors appear more solid, tend to have a yellow color (Figs. 1 and 3) with a similar appearance to fat, and have less necrosis or hemorrhage [4].
A third, much less common type of CMN, can also occur. This is the mixed type, which has components of both classical and cellular and occurs in only 10% of cases [6]. The degree of relapse for this type of tumor is not well described. Both of our patients were ultimately diagnosed with this rare type of tumor (Figs. 3 and 6).
One of our two patients was identified on prenatal ultrasound and the other on initial physicalexamination and x-ray in the nursery. Prenatal diagnosis is becoming more and more common as ultrasounds technology improves. The most common initial finding leading to prenatal diagnosis is polyhydramnios, which is present in 71% of mothers of infants with CMNs, due to impaired gastrointestinal function and excessive fetal urine production [7]. Reports have shown CMNs have been detected as early as 26 weeks gestation [8]. Interestingly, our second patient had a normal fetal ultrasound at 22.2 weeks gestation, before having the polyhydramnios noted on a follow up ultrasound at 33.4 weeks.
The most common presentation is an asymptomatic abdominal mass; however, paraneoplastic syndrome or hematuria can also be present [2, 5]. Additionally, hypertension is an extremely common presenting symptom, as nearly one half of CMN infants have increased blood pressures [5]. Typically, after removal of the tumor an infant’s hypertension will completely resolve. One of our two infants, followed this typical clinical course, however, the other did not and was discharged home on amlodipine. This infant also had elevated serum creatinine (0.52 mg/dL).
There is no predilection for the left or right side [1]. Additionally, the underlying type of tumor determines timing for the onset of symptoms. Classical type CMN presents early, at around 6 days of age, while cellular type tends to present later at around 121 days of life [4]. The mean age of presentation for mixed type has not been well described in the literature. Non-invasive, low radiation imaging modalities play a crucial role in the diagnosis of CMNs. As stated, many infants are diagnosed on prenatal US, not by detection of a clear image of the mass, but rather an increased amount of amniotic fluid. MRI tends to be the preferred imaging modality for high resolution evaluation, due the lack of radiation exposure. We elected to perform an MRI on both patients (Figs. 1 and 3) and our findings of a heterogeneous mass with minor increase in signal intensity along the edges of the mass were consistent with those described in the literature [4, 7]. Both of our patients underwent routine management for CMN. Fortunately, patients with CMN have excellent prognosis after surgical resection. Nephrectomy of the affected side is the treatment of choice. While the risk of recurrence is related to the underlying pathology of the lesion, the literature reports survival rates between 94% to 98% [2, 5]. Overall the risk of recurrence for all types is around 5% [6]. Patients at the greatest risk for recurrence are those with spread to the abdominal lymph nodes and with margins that were not clear upon resection [3].
Interestingly, the second patient’s clinical course was complicated by significant direct hyperbilirubinemia. This feature has not been reported to be associated with CMNs in the literature. This may be partially due to his complicated post-operative course. The known neonatal renal mass, which presents with jaundice is clear cell carcinoma of the kidney [9]. The presentation of two mixed type congenital mesoblastic nephromas to a single center within a two week period is an extremely rare event that has not been previously described in the literature.
This case emphasizes the importance of a thorough physical examination of every infant that enters a regular or intensive care nursery. While ultrasound, computed tomography, and magnetic resonance imaging are excellent adjuncts, a complete physical exam can help guide clinicians to the appropriate test. The most important questions to answer on physical exam for a suspected abdominal mass are consistency and location (Table 1). Masses that are not compressible are more likely solid, where as those that are compressible are usually cystic in nature. The location of the mass also helps narrow the differential diagnosis. Flank masses tend to be of adrenal origin or renal origin; intraperitoneal masses, are typically located mid abdomen; pelvic masses are located in the suprapubic region [10].
The differential diagnosis of neonatal abdominal masses can be narrowed by performing a complete exam of the abdomen when the baby is calm and relaxed. Characteristics such as compressibility and location can greatly aid the clinician in identification of the unknown mass [10]
While these lesions are rare, our case series indicates that this etiology needs to remain in the differential diagnosis for all pediatricians, neonatologist, and pediatric surgeons. While recurrence rate for this type of CMN in unknown complete resection and close follow up should provide optimal outcome. Prompt recognition and treatment is important for optimal outcomes for these infants.
Conflict of interest
The authors have no conflicts of interest relevant to this article to disclose.