
Abstract
Introduction
The fetus is known to predict and subsequently, adapt to the environment it will be born into (on the basis of intra-uterine conditions) to gain a competitive advantage in later life [1]. However, these adaptations later may lead to the origin of diseases like coronary artery disease, diabetes mellitus and hypertension [2]. Association between low birth weight (LBW) and cardiovascular diseases in adulthood has been widely replicated in previous studies conducted in the USA and Europe [3–5]. The cord blood lipid profile has been shown to be associated with changes in the metabolic functions in later life; therefore, the assessment of serum lipid levels in neonates might be of importance [6].
Impaired fetal growth has been associated with elevated serum cholesterol and apolipoprotein -B (Apo-B) concentrations in adulthood [7–9]. Increased Apo-B levels and an elevated Apo-B to apoliprotien-A-1 (Apo-A1) ratio are considered to be the most sensitive predictors of atherogenesis [10]. The incidence of coronary heart disease in Indian adults is also increasing but the effects of intrauterine growth retardation (IUGR) on cord blood lipid profile and their predictive role as markers of adulthood diseases is not completely explored [11, 12]. Therefore, we conducted this study to evaluate the influence of IUGR over lipid profile in Indian cohort ofneonates.
Material and methods
A hospital based cross-sectional study was conducted in the Department of Pediatrics and the Department of Obstetrics and Gynecology, of a tertiary care teaching hospital of Central India. The study was conducted over a period of 6 months after obtaining approval from the institutional ethics committee. Informed consent from both the parents of the eligible newborns was also obtained before enrollment. Only healthy term newborns of either sex born by normal vaginal delivery after an uneventful normotensive pregnancy were included in the study. Of these, full-term (>37 weeks of gestation) small for gestational age newborns (SGA i.e. birth weight less than 10th percentile for their gestational age) were taken as cases while full-term appropriate for age newborns (AGA i.e. birth weight between 10th and 90th percentile for their gestational age) were taken as controls.
Newborns of the mothers having a history of familial hypercholesterolemia and/or having a history of medical disorders associated with hypercholesterolemia (diabetes mellitus, renal, hepatic, or thyroid function disorders) as per the medical records of the mother were not recruited in the study. Newborns with any perinatal complication (e.g. perinatal asphyxia, respiratory distress syndrome), congenital anomalies or requiring admission in NICU within 24 hours of life, preterm (less than 37 weeks of gestation) or post-term newborns (more than 42 weeks of gestation), large for date newborns (birth weight >90th percentile) were excluded from the study as shown in Fig. 1.
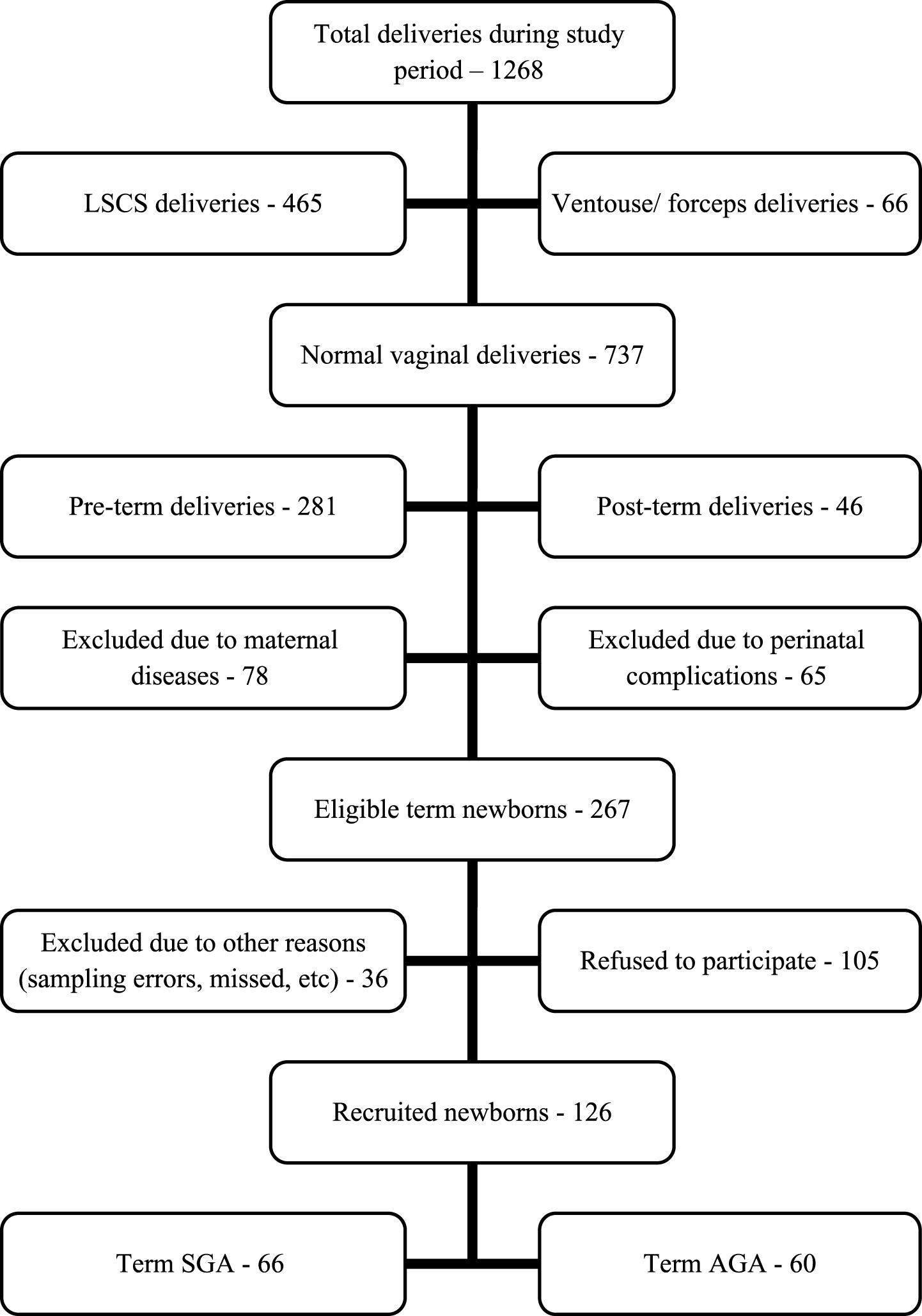
Study flowchart.
After recruitment, demographic details of mothers including maternal age, parity, and last menstrual period (LMP) were recorded. Birth weight was taken over electronic weighing machine specifically designed to weigh newborns with an accuracy of±5 gm (SECA Model –727) and length was recorded using an infantometer. Head circumference was measured using non-stretchable tape passing above the supraorbital ridge and over occipital protuberance. Gestational age was assessed by LMP and new Ballard scoring [13, 14]. These data were plotted on intrauterine growth charts and newborns were recruited into either SGA or AGA group according to the criteria set by Alexander et al. [15].
Six milliliters of cord blood was collected from the placental end of the umbilical vein after the birth of the baby and before the expulsion of the placenta while mothers were in the non-fasting state. Samples were centrifuged within 5 minutes of collection and aliquots of plasma were stored at –20° C until further analysis.
Serum triglyceride, total cholesterol, HDL-C, and LDL-C concentrations were measured on a Hitachi 902 autoanalyzer (Hitachi High-Technologies Corporation, Tokyo, Japan) by enzymatic colorimetric assay (Roche, Mannheim, Germany). Serum apolipoprotein A-1 (Apo-A1) and apolipoprotein B (Apo-B) levels were measured via nephelometry (by Nephelometer 100 Analyzer). The Intra and inter-assay coefficients of variations were <2% for total cholesterol (TC) and triglycerides (TG), and <5% for Apo-A1 and Apo-B. Serum low-density lipid cholesterol (LDL-C) was calculated using the Friedewald–Fredrickson formula: LDL = TC –HDL –(TG/5) (provided that triglycerides levels were lower than 400 mg/dl).
All of the statistical analyses were performed using SPSS statistical software version 17.1 (SPSS Inc., Chicago, IL, USA). Results on continuous measurements are presented as mean with standard deviation (SD) and results on categorical measurement are presented in number and percentage. The significance is assessed at 5% level of significance. Student t-test (two-tailed, independent) has been used to find the significance of study parameters on a continuous scale between two groups. Pearson’s correlation carried out to find the relationship between the pairs of study variables.
In this study, 66 SGA and 60 AGA eligible newborns were recruited as per the details shown in Fig. 1. Male preponderance (60%) was observed in the SGA group while in AGA group sex ratio was equal. Mean gestational age and birth weight in SGA group were 38.81±0.72 weeks and 1.923±0.628 kg respectively while in AGA group these values were 39.04±0.89 weeks and 2.745±0.354 kg respectively. The demographic profile of study population is given in Table 1. As shown in Table 2, the difference between mean values of serum triglyceride (141.56±69.67 vs. 113.67±33.38; p < 0.006; 95% CI = 8.31 to 47.46) and serum apo-B/apo-A-1 ratio (0.67±0.28 vs. 0.55±0.20; p < 0.007; 95% CI = 0.033 to 0.206) was significantly high and that of HDL-C (35.84±10.42 vs. 40.73±11.70; p < 0.014; 95% CI = –8.79 to –0.98) and Apo-A1 [87.59±12.44 vs. 101.87±35.07; p = 0.002; 95% CI = –23.39 to –5.16) was significantly low in SGA newborns. Serum cholesterol,VLDL-C rLDL-C and apo-B did not show any significant difference. Among SGA neonates there were highly significant negative correlations between birth weight and Apo-B/Apo-A1 (r = rand there was a significant positive correlation between birth weight and serum Apo-A1 level (r = 0.276 at 0.01 level). There was no statistically significant difference in mean values of lipid profile and serum Apo-B and Apo-A1 among male and female newborns.
Demographic profile of the study population
Demographic profile of the study population
Lipid profile of the study population
Measurement of serum lipoproteins in infancy and childhood could be predictive for lipoprotein disorders and cardiovascular diseases in adulthood since LBW is an important risk factor for cardiovascular diseases, especially in low-income countries. In the present study, we found significantly higher levels of serum triglycerides and Apo-B/Apo-A1 ratios as well as significantly lower levels of Apo-A1 in SGA neonates than in AGA neonates. It is well-documented that low Apo-A1 and/or elevated Apo-B and LDL-C in young adults are linked with cardiovascular diseases in later life [16]. Lower serum Apo-A1 seen in SGA newborns in the present study might result in higher Apo-B/Apo-A1 ratio in SGA newborns as was reported by Morlese et al [17]. We found a negative correlation between birth weight and Apo-B/Apo-A1 as reported by Sattar et al. also [18].
Radunovic N et al. reported significant differences in Apo-B level and its ratio to Apo-A1 in growth retarded fetuses as compared to the normal fetus [19]. They also reported that fetal Apo-A1 and Apo-Blevels do not correlate with gestational age. Fetal growth retardation establishes a life-long irreversible atherogenic profile and those individuals with a history of low birth weight are reported to have an atherogenic profile [19]. In the present study, Apo-A1 showed a positive correlation with birth weight. This observation of the present study, as well as the previous studies, are suggestive of the rate of production and/or clearance of Apo-A1 is altered during the latter third of human intrauterine development and is affected by growth restriction. Further research is needed to determine the exact mechanism. Barker et al. have reported an inverse correlation between birth weight and neonatal abdominal circumference with adult serum cholesterol, LDL-C, and Apo-B levels, suggesting that the association between aberrant lipoprotein metabolism and low birth weight is present by the time intrauterine growth restriction is clinically evident [20]. Other reports have demonstrated that abnormal lipoprotein profiles in childhood persist into adult life [21, 22]. Furthermore, the prevalence and severity of carotid artery atherosclerosis in later life are linked to lower birth weight [23]. A Swedish cohort study found a strong relationship between impaired fetal growth and subsequent cardiovascular mortality [5]. These findings indicate that fetal growth restriction is associated with a chronic pattern of atherogenic lipoprotein metabolism.
Immunochemical studies of the umbilical cord lipid transport system have shown that all the well-characterized apolipoproteins are present in cord blood, although at a lower level than that found in the normal adult. McConathy et al. reported the existence of all well-characterized adult apolipoproteins in cord blood, with Apo-B levels being the most reduced [24]. In the present study, we also observed that Apo-B level was the most reduced apolipoprotein parameter and Apo-A1 was higher.
In this study, serum triglyceride was significantly high in SGA group as compared to AGA group, and there was a significant negative correlation between birth weight and serum triglyceride. Authors of the different studies conducted in newborns [6, 19] and fetuses [9, 18] have concluded similar results in their studies. Conversely, Diaz et al found that HDL-C was substantially higher (P < 0.05) in umbilical cord plasma of SGA newborns than in cord plasma of full-term newborns [25].
The fetus needs a considerable amount of cholesterol for the development of tissues and organs; there should be no surplus cholesterol. However, high Apo-A1 is found to track closely during the first year of life [26]. Limitations of this study were financial constraints so that we could not compare these values with maternal lipid profile. Secondly, the sample size was small and we could not collect the follow-up data. Longitudinal follow-up study with large sample size may confirm the relationship of the atherogenic milieu of IUGR neonates with adult coronary heart disease.
Conclusion
Roots for many adult diseases, including atherosclerotic cardiovascular diseases, begin in childhood and clustered risk factors track from childhood to adulthood. These factors can be altered favorably and can be modified by preventive interventions and early lifestyle-related factors. Establishment of references values for lipoprotein and apolipoprotein would facilitate comparison between different studies. These findings are another supportive evidence for the association of prenatal factors with cord blood lipid profile and can serve as starting point for studying lipid transport system changes during early life in Indian population.
Conflict of interest statement
We declare that we have no conflict of interest.
Sources of funding
None.