
Abstract
BACKGROUND:
The optimal composition of lipid emulsions in parenteral nutrition (PN) for premature infants remains controversial. This study examined the effects of a combination of soybean oil-based (SoyLE) and fish oil-based (FishLE) lipid emulsions compared to FishLE as monotherapy on the lipid and fatty acid profiles and clinical outcomes of premature infants requiring prolonged PN.
METHODS:
42 premature infants received FishLE+SoyLE or FishLE. Serum concentrations of lipoproteins and 29 fatty acids (FA) were measured at baseline, 4, and 8 weeks of PN and growth and neurodevelopmental outcomes were measured at 3, 6, 12, 18, and 24 months of life.
RESULTS:
Lipid profiles were similar between groups. Plasma concentrations of ω-6 fatty acids tended to decrease over time in both groups. Concentrations of most ω-3 fatty acids, in particular docosapentaenoic acid, eicosapentaenoic acid, and docosahexaenoic acid, were significantly increased over time in the FishLE+SoyLE group whereas they did not change in the FishLE alone group. However, serum concentrations of almost all fatty acids were similar between groups at the end of the study period. No differences in growth parameters including weight, height, fronto-occipital circumference (FOC), and body mass index (BMI) were observed up to two years of age. Similarly, there were no differences in neurodevelopmental test scores at 6, 12, 18, and 24 months of age.
CONCLUSIONS:
No substantial differences in lipid profiles and short clinical outcomes were found in infants exposed to FishLE+SoyLE when compared to FishLE.
Introduction
Premature infants have an increased risk of developing liver and cardiovascular diseases (CVD) as adults, possibly due to the altered metabolic adaptations that take place during the neonatal period [1, 2]. Many preterm infants require parenteral nutrition (PN), including intravenous lipid emulsions to survive, grow, and prevent other complications such as essential fatty acid deficiency [3, 4].
The optimal composition of these lipid emulsions remains controversial, and it has been shown that different types of lipid emulsions can have different effects on plasma fatty acid and lipid composition. A study by Lewandowski et al. [5] demonstrated that premature infants who are exposed to soybean oil-based lipid emulsions (SoyLE) during neonatal life exhibited elevated cholesterol levels, leading to changes in aortic stiffness and myocardial strain in adulthood [5]. SoyLEs are comprised of approximately 50% linoleic acid, an ω-6 fatty acid, which when present in large quantities, is believed to promote inflammation and immunosuppression [6]. Conversely, fish oil-based lipid emulsions (FishLE) contain high concentrations of docosahexanoic acid and eicosapentainoic acid, two ω-3 fatty acids, which are known for their anti-inflammatory properties [7–11]. Several studies in adults have shown that SoyLEs may negatively alter lipid profiles and contribute to the development of intestinal failure-associated liver disease (IFALD) [12–14]. In contrast, FishLEs have shown a favorable effect on lipid profiles, the normalization of liver function tests, and reversal of IFALD [9, 16]. Moreover, studies in PN-dependent children and term infants using FishLE as monotherapy have shown no signs of fatty acid deficiencies [17–19].
In the United States, the Food and Drug Administration (FDA) has approved a SoyLE, Intralipid®, and more recently, a FishLE, Omegaven®, for clinical use in pediatric populations. This represents a major innovation in the management of PN-dependent pediatric patients.
The maximum recommended dose for FishLE is 1 g/k/day in pediatric patients. The reduced caloric intake associated with this relatively low dose of lipids raises concerns for negative impacts on growth and neurodevelopment in the preterm population. Therefore, using a combination of SoyLE and FishLE may be clinically advantageous for treatment in preterm infants, by allowing the benefits and concerns of each therapy to balance the other. To our knowledge, no study to date has investigated the plasma fatty acid profiles and long-term growth and neurodevelopmental outcomes that result from the treatment of preterm infants with FishLE monotherapy or in combination with SoyLE.
The purpose of this study was to examine the effects of FishLE administered in conjunction with SoyLE on the lipid profiles, short-term clinical outcomes, and long-term growth and neurodevelopmental outcomes of premature infants requiring PN compared to those that received FishLE as monotherapy. We hypothesized that using FishLE in conjunction with SoyLE in premature infants at risk of developing IFALD, would lead to differences on their lipid profiles, fatty acid profiles, clinical, and long-term growth and neurodevelopmental outcomes, bringing them closer to reported neonatal levels, as compared to those that receive FishLE alone. We also speculated that infants receiving FishLE alone would have lower than normal levels of ω-6 fatty acids than those receiving FishLE in combination with SoyLE after 8 weeks of LE therapy.
Materials/subjects and methods
This study was approved by the Institutional Review Boards at the University of Texas Health Science Center at San Antonio and University Hospital (UH), San Antonio, Texas and was performed in accordance with the Declaration of Helsinki. This study was conducted prior to the approval by the FDA for the clinical use of Omegaven® in pediatric populations. The clinical trial titled Compassionate Use of a Fish Oil-Based Intravenous Lipid Emulsion in the Treatment of Parenteral Nutrition-Associated Liver Disease in Infants was registered with the NIH Clinicaltrials.gov as #>NTC01425567.
Subjects
The study population consisted of 42 preterm infants born before 37 weeks gestation, admitted to the Neonatal Intensive Care Unit (NICU) at UH between 2011 and 2017. Enrollment criteria included: postnatal age between 14 days and 24 months of age, and a requirement of at least 60% of caloric intake by intravenous infusion, and signed informed consent to participate in the study. A multidisciplinary team of dietitians, neonatologists, and gastroenterologists reviewed patient eligibility and coordinated patient care. Infants diagnosed with short bowel syndrome or severe intestinal dysmotility requiring PN for an additional 28 days were enrolled in the protocol and divided into two study groups set a priori. The FishLE group consisted of infants with severe IFALD, including a direct bilirubin (DB) >4 mg/dL. Following enrollment, SoyLE was discontinued and the FishLE group received Omegaven® (Fresenius Kabi; Bad Homburg, Germany) at a rate of 1 g/kg/day. The FishLE+SoyLE group consisted of infants deemed to be at high risk of developing IFALD, with DB >1 mg/dL but <4 mg/dL, and one or more of the following characteristics: birth weight <750 g, necrotizing enterocolitis with laparotomy or drain, gastroschisis, or jejunal atresia. After enrollment the FishLE+SoyLE group continued to receive Intralipid® (Fresenius Kabi; Uppsala, Sweden), at a rate of 1-2 g/kg/d in conjunction with Omegaven® at a rate of 1 g/kg/d. If infants in the FishLE+SoyLE group reached a DB >4 mg/dL, Intralipid® was discontinued and Omegaven® was continued at a rate of 1 g/k/d. Both groups remained on the Omegaven® protocol until they were weaned from PN for >10 days or their cholestasis was resolved (DB <1 mg/dL for four consecutive weeks) (Fig. 1).
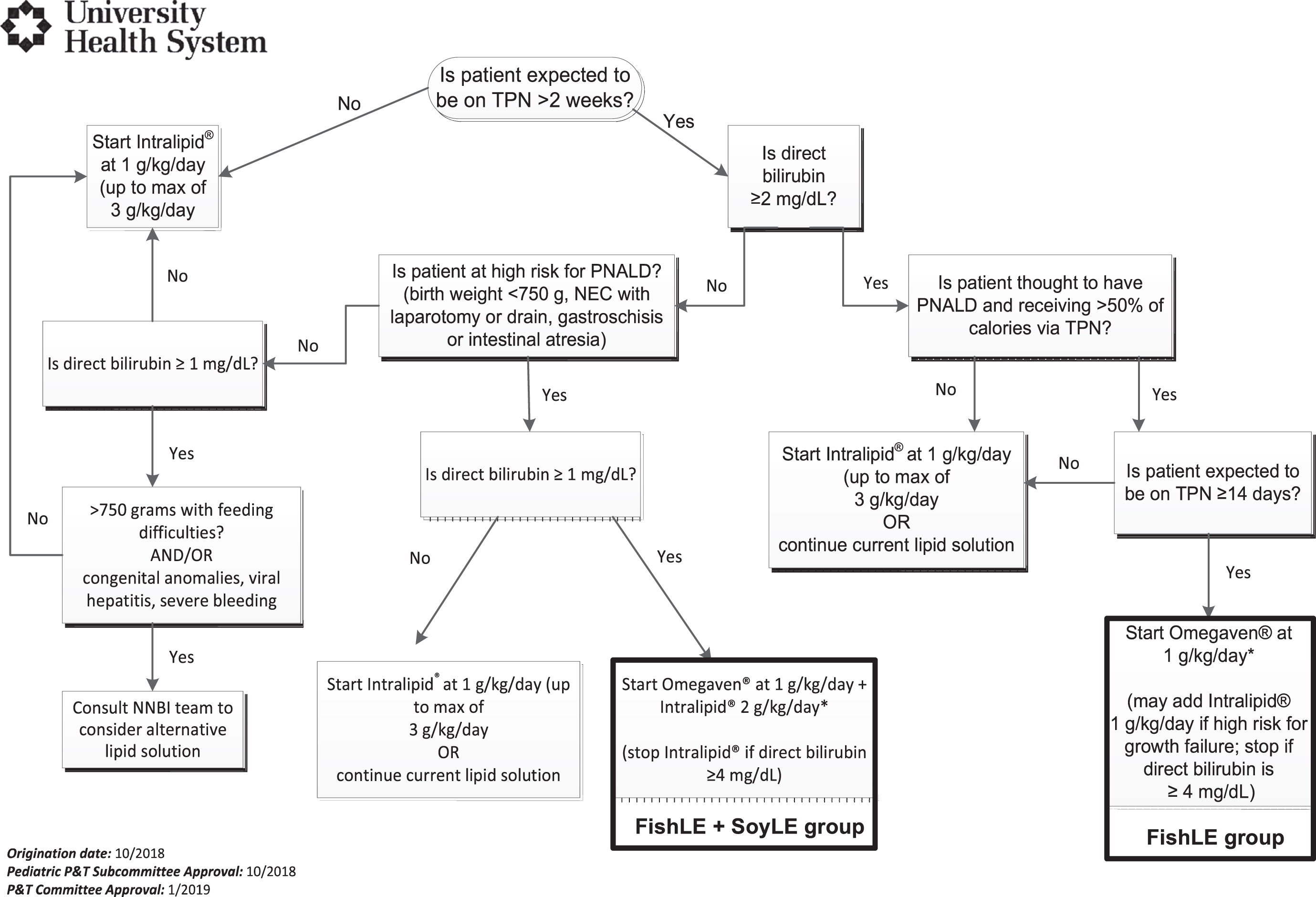
Decision tree used in the University Health System Neonatal Intensive Care Unit for lipid selection in neonates and infants. Text boxes with bold outline show the two study treatment groups.
Baseline demographic data (birth weight, gestational age, gender, race/ethnicity, discharge weight, maternal diseases, and other clinical data) were recorded prospectively from medical records. Laboratory results for liver function tests including DB, alanine aminotransferase (ALT), aspartate aminotransferase (AST), and gamma-glutamyl transferase (GGT) were obtained weekly and nutritional data was recorded daily. Clinical outcomes including length of stay, resolution of cholestasis, and other morbidities were also recorded. Follow-up data including growth parameters (weight, height, FOC, BMI) neurodevelopmental outcomes (cognitive, language, and motor scores) from Bayley Scales of Infant and Toddler Development®, Third Edition (Bayley III®) were obtained from the Neonatal Follow-Up PREMIEre Clinic at 3, 6, 12, 18, and 24 months of age.
Lipid and fatty acid profiles
Blood samples (0.5 ml) were collected from patients at enrollment (baseline), week 4, and week 8 of lipid emulsion therapy. These samples were centrifuged at 3,000 rpm for 10 minutes and the plasma stored at –80°C until analyses were performed. Lipid profile analysis included measuring the levels of total cholesterol (TC), triglycerides (TG), high-density lipoprotein (HDL), and low-density lipoprotein to very low-density lipoprotein ratio (LDL/VLDL). TC, HDL, and LDL/VLDL concentrations were measured using the HDL, LDL, and LDL/VLDL Cholesterol Assay Kit (Abcam; Cambridge, United Kingdom). Plasma TG levels were measured in the UH lab every four weeks for clinical purposes. Plasma non-esterified free fatty acid concentrations were measured using the HR-Series NEFA-HR kit from (Wako Diagnostics; Mountain View, CA) as per protocol to monitor triene-tetraine ratio. For fatty acid profile analysis, plasma samples were sent to Metabolon Inc. (Morrisville, NC) for analysis of 29 fatty acids using liquid chromatography-mass spectrometry.
Statistical analyses
All statistical analyses were performed using SPSS for Windows, version 26.0 (SPSS Inc., Chicago, IL). The data was determined to be normally distributed through histograms. Chi-square tests, Students’ t-test, repeated measures ANOVA, two-tailed Spearman correlations, and logistic regression analyses were used as appropriate. A value of p < 0.05 was considered statistically significant. Quantitative data was summarized using mean±standard deviation or median (interquartile range) and qualitative data was summarized using proportions and percentages. Missing data were dropped from the analysis.
Results
Demographics and Clinical Outcomes
Forty-two preterm infants receiving either FishLE (Omegaven®) or FishLE+SoyLE (Omegaven® + Intralipid®) were selected for this study. Infants receiving FishLE+SoyLE were, on average, 28 days younger than those receiving FishLE at the time of enrollment (p = 0.002); however, they had similar post-menstrual age (53 vs 58 weeks, respectively) (Table 1). Additionally, the FishLE+SoyLE group received a total cumulative amount of lipids 56% higher during the length of LE therapy (p = 0.007) and 46% higher during their entire hospitalization (p = 0.01) when compared to the FishLE group (Table 1). There were no significant differences in the monthly average and cumulative caloric intake before, during, and after LE therapy or during entire hospitalization between groups (Table 2). Patients receiving FishLE+SoyLE had a DB level 75% lower at baseline (p < 0.001), 55% lower at peak (p < 0.001) and 64% lower at the end of LE therapy (approximately 13 weeks) (p = 0.03) when compared to those receiving FishLE (Table 3).
Demographics and clinical data of study groups
Demographics and clinical data of study groups
aData is expressed as mean±standard deviation or as n (%). bTotal IV lipid intake is the cumulative amount of lipids received. cFOC = fronto-occipital circumference, GA = gestational age, PDA = patent ductus arteriosus, BPD = bronchopulmonary dysplasia, IVH = intra-ventricular hemorrhage, LE = lipid emulsion, SIP = spontaneous intestinal perforation, PMA = postmenstrual age, PN = total parenteral nutrition, IV = intravenous, DB = direct bilirubin. dTrophic feeds defined as <20 ml/kg/d. eFull feeds defined as >120 ml/kg/d. f *p < 0.05, **p < 0.01.
Enteral caloric intake
aData presented as mean±standard deviation. bLE = lipid emulsion.
Liver function tests laboratory values
aData presented as mean±standard deviation. bLFT = liver function test, DB = direct bilirubin, ALT = alanine aminotransferase, AST = aspartate aminotransferase, GGT = gamma-glutamyl transferase. c+2 weeks = 2 weeks after end of LE therapy, +4 weeks = 4 weeks after end of LE therapy. d *p < 0.5, **p < 0.001.
Plasma lipoprotein, TG, TC, HDL, LDL/VLDL and fatty acid measurements performed in a subset of infants (Table 4). At baseline, plasma concentrations of alpha-linolenic acid (128%, p = 0.041), linoleic acid (162%, p = 0.002), and gamma-linolenic acid (55%, p = 0.043) were higher in the FishLE+SoyLE group (Table 4). In contrast, the FishLE+SoyLE group had significantly lower concentrations of eicosatetraenoic acid (54%, p = 0.013), docosapentaenoic acid (63%, p = 0.033), mead acid (59%, p = 0.046), myristoleic acid (47%, p = <0.001), palmitoleic acid (46%, p = 0.002), vaccenic acid (40%, p = 0.032), myristic acid (50%, p = 0.020), and pentadecanoic acid (45%, p = 0.041) compared to the FishLE group at baseline. At 4 weeks of LE therapy, there were higher concentrations of linoleic acid (68%, p = 0.025), adrenic acid (27%, p = 0.009), and cis-11,14-eicosadienoic acid (68%, p = 0.026) in the FishLE+SoyLE group. At 8 weeks of LE therapy, only adrenic acid remained higher (68%, p = 0.044) in the FishLE group (Table 4).
Lipid and fatty acid profiles
Lipid and fatty acid profiles
aData presented as median (interquartile range). b †denotes essential fatty acids. cPUFA = polyunsaturated fatty acid, MUFA = monounsaturated fatty acid, SAT = saturated fatty acids. TC = total cholesterol, HDL = high density lipoprotein, LDL = low density lipoprotein, VLDL = very low density lipoprotein, N/Q = not quantifiable. d *p < 0.05, **p < 0.01.
There was a significant increase over time in the ω-3 poly-unsaturated fatty acids (PUFAs) stearidonic acid, eicosatetraenoic acid, eicosapentaenoic acid, docosapentaenoic acid, and docosahexaenoic acid (p < 0.05) and a significant decrease over time in alpha-linolenic acid (p = 0.016) in the FishLE+SoyLE group, but no significant changes were observed in the FishLE group (Fig. 2). There were significant decreases over time in the ω-6 PUFAs linoleic acid, gamma-linolenic acid, dihomo-gamma-linolenic acid, arachidonic acid, osbond acid, and cis-11,14-eicosadienoic acid in the FishLE+SoyLE group (p < 0.05). Likewise, the FishLE group showed significant decreases in gamma-linolenic acid, dihomo-gamma-linolenic acid, arachidonic acid, osbond acid, and cis-11,14-eicosadienoic acid over time (p < 0.01), but unlike the FishLE+SoyLE group, the FishLE group also showed a significant decrease over time in the level of adrenic acid (p = 0.01) (Fig. 3). Only the FishLE group showed a significant decrease in mead acid (p = 0.002) over time. Only the FishLE+SoyLE group showed a significant increase in myristoleic acid (p = 0.03) over time. Both groups showed a significant decrease in palmitoleic acid (Fish+SoyLE p = 0.01, FishLE p = 0.03) over time (Table 4).
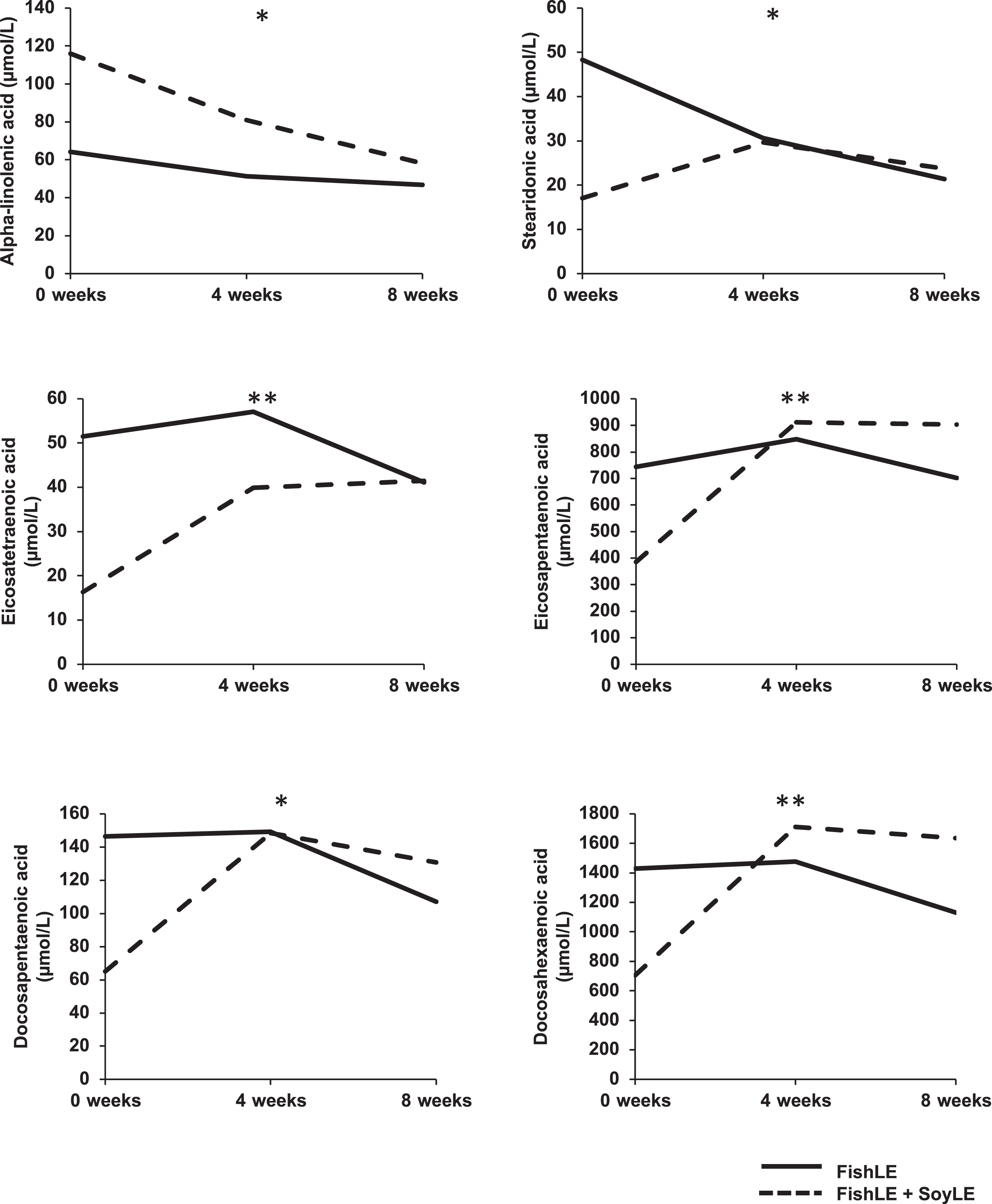
Concentrations of ω-3 fatty acids (reported in μmol/L) in the plasma of premature infants receiving a fish oil-based lipid emulsion (FishLE) alone or in combination with a soybean oil-based lipid emulsion (FishLE+SoyLE) at baseline, 4 weeks, and 8 weeks of lipid emulsion therapy. Solid line = FishLE, Dotted line = FishLE+SoyLE. *=p < 0.1, **=p < 0.001 in FishLE+SoyLE over time.

Concentrations of ω-6 fatty acids (reported in μmol/L) in the plasma of premature infants receiving a fish oil-based lipid emulsion (FishLE) alone or in combination with a soybean oil-based lipid emulsion (FishLE+SoyLE) at baseline, 4 weeks, and 8 weeks of lipid emulsion therapy. Solid line = FishLE, Dotted line = FishLE+SoyLE. *=p < 0.1, **=p < 0.001 in FishLE+SoyLE over time, †=p < 0.1, ‡=p < 0.01 in FishLE group over time.
There were significant increases in the saturated fatty acids myristic acid and pentadecanoic acid (p < 0.01) and a significant decrease over time in arachidic acid (p = 0.04) in the FishLE+SoyLE group. The FishLE group showed significant decreases of palmitic acid and stearic acid (p = 0.02 and 0.01, respectively) over time (Table 4).
There was no correlation between cumulative lipid intake from baseline to 4 weeks and any fatty acid concentration (data not shown).
There were no differences in weight, height, FOC, BMI, systolic and diastolic blood pressure, or pulse between groups at 3, 6, 12, or 24 months of age (Table 5). Additionally, no differences were observed between groups in neurodevelopment scores including cognitive, language, and motor skills (Table 6). In regards to early intervention services, a higher percentage of patients in the FishLE+SoyLE group received speech (ST), physical (PT), and/or occupational therapy (OT) at 12 months CGA (PT/ST 6% vs 47%, OT 6 vs 35%, FishLE vs FishLE+Soy, p < 0.01 respectively); at 18 months CGA (ST 9% vs 35% FishLE vs FishLE+SoyLE, p < 0.01 respectively; at 24 months of age (OT 9% vs 35% FishLE vs FishLE+SoyLE) (data not shown).
Growth and cardiovascular parameters
Growth and cardiovascular parameters
aData is expressed as mean±standard deviation. bFOC = fronto-occipital circumference. c *p < 0.05, **p < 0.01.
Neurodevelopmental follow-up
aData is expressed as mean±standard deviation. b *p < 0.05, **p < 0.01.
Spearman two-tailed correlations were used to assess the relationship between neurodevelopmental outcomes and fatty acid concentrations and plasma lipoproteins. At 18 months of age, we found negative correlations between language scores and plasma concentrations of arachidonic acid (r = –0.61, p = 0.05), docosahexaenoic acid (r = –0.74, p = 0.01), and total ω-3 (r = –0.77, p = 0.01) at 4 weeks of LE therapy. Additionally, there was a negative correlation between motor scores and adrenic acid (r = –0.61, p = 0.04) concentrations at 4 weeks of LE therapy. At 24 months of age, we found a positive correlation (r = 0.57, p = 0.05) between language scores and α-Linolenic Acid concentrations at 4 weeks of LE therapy. However, all of these differences disappeared after adjusting for day of life when LE therapy started and cumulative amount of lipids during LE therapy via logistic regression analyses (Fig. 4).

Spearman rank correlation graph showing the significant relationships between plasma fatty acid concentrations and neurodevelopmental test (Bayley III®) scores at 4 weeks of lipid emulsion therapy. p < 0.05 was considered statistically significant. LE = lipid emulsion.
In terms of plasma lipoprotein concentrations at 8 weeks of LE therapy, we found a negative correlation between total cholesterol and cognitive scores at 18 months of age (r = –0.79, p = 0.02) and a positive correlation between triglycerides and language scores at 24 months of age (r = 0.70, p = 0.02). (Fig. 5).
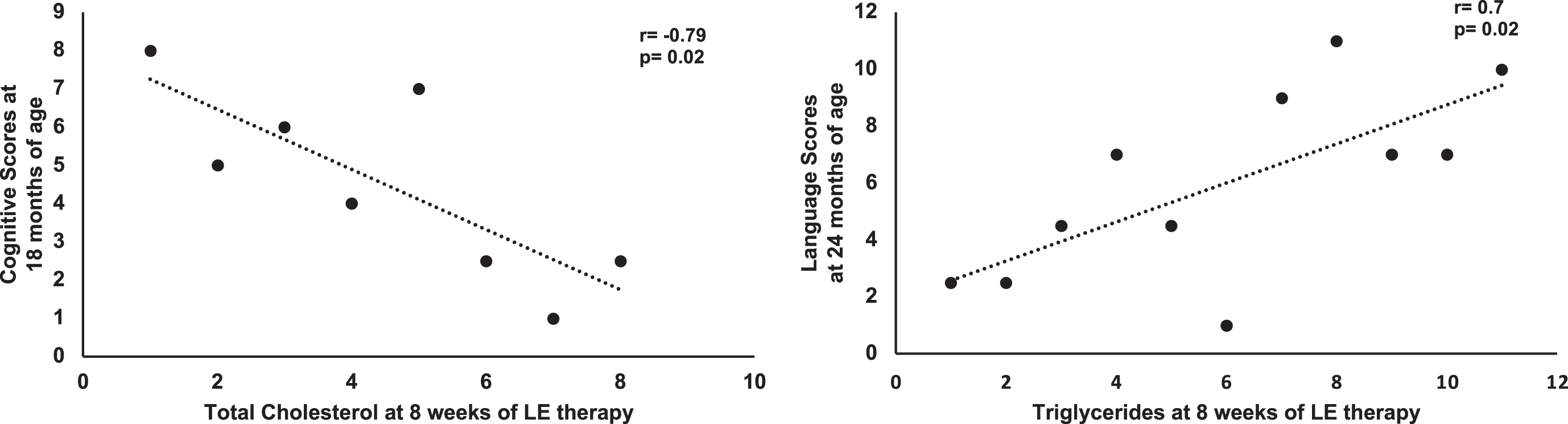
Spearman rank correlation graph showing the significant relationships between plasma lipoprotein concentrations and neurodevelopmental test (Bayley III®) scores at 8 weeks of lipid emulsion therapy. p < 0.05 was considered statistically significant. LE = lipid emulsion.
Despite numerous reported advantages of using FishLE as monotherapy in infants and children, concerns about dosing and composition of FishLE remain. These include concerns for adverse neurodevelopmental outcomes due to caloric restriction and the lower contents of linoleic acid and alpha linoleic acid in FishLE compared to SoyLE. One way to address these concerns could be the administration of a combination of FishLE and SoyLE, thereby balancing these benefits and concerns. To our knowledge, this is the first study to examine the effects of a combination of FishLE at 1 gr/k/day and SoyLE at 1-2 gr/k/day on the lipid and fatty acid profiles in the plasma of premature infants.
As expected, due to the lipid infusion rate of each group, we found that the FishLE+SoyLE group received close to 60 g/kg more of total cumulative IV lipids during LE therapy and approximately 70 g/kg more than the FishLE group during their entire hospital stay. Our results support current data that FishLE alone does not contribute to the development of fatty acid deficiencies and may aid in its reversal [20].
We found that concentrations of ω-6 fatty acids tended to decrease overtime regardless of lipid type/cumulative intake. This may be beneficial, as high levels of ω-6 fatty acids have been associated with reduced levels of docosahexaenoic acid in the brain [21, 22]. Despite differences in plasma fatty acid profiles overtime, at the end of the 8-week study period, the concentrations of almost all fatty acids were similar between groups. Although the FishLE+SoyLE population showed decreases in linoleic acid and alpha-linolenic acid overtime, studies have suggested that the presence of arachidonic acid, eicosapentaenoic acid, and docosahexanoic acid in FishLEs may diminish the requirements for these essential fatty acids [23].
In contrast, the ω-3 fatty acids eicosapentaenoic acid and docosahexaenoic acid, both critical for early neurodevelopment, were lower at baseline in infants in the FishLE+SoyLE but had a significant increase overtime and by 8 weeks had similar concentrations as those in FishLE group. These differences between groups might be due to enteral feedings used prior to enrollment in this study, which could be attributed to the types of enteral feeds (human milk or formula) and PN they received. However, both groups had a high number of NPO days during lipid emulsion therapy and therefore, their enteral intake was minimal. It is likely that infants in the FishLE+SoyLE group were younger and although had similar CGA at entry, ω-3 fatty acids might be lower at lower postnatal days and increased as postnatal age increased.
In regards to long term neurodevelopment we found no correlations between FFA levels alone or in combination, or change over time with any neurodevelopmental outcomes after adjusting for day of life and cumulative lipid intake. Although no differences were observed in neurodevelopmental test scores between groups, we noted that patients in the FishLE+SoyLE group were also more likely to receive speech, physical, and/or occupational therapy when compared to the FishLE group. Speech and fine motor delays are common in children born preterm and the possibility that FishLE as monotherapy reduces these delays warrants further investigation. We speculate that higher ω-3 fatty acids, specicially eicosapentaenoic acid and docosahexaenoic acid at baseline may contribute to these differences. It remains to be determined why infants in the FishLE+SoyLE group had lower ω-3 fatty acids and the length of this lower concentrations as we don’t have FFA from birth to enrollment.
Despite FishLE+SoyLE receiving higher cumulative lipid intake, we did not find any differences in growth and plasma lipid profiles. There were differences in DB between groups with lower concentrations at baseline, peak (75% lower in FishLE+SoyLE vs FishLE) and both groups improved overtime. Additionally, it is important to highlight that the FishLE group had a DB change of 5 mg/dL while the FishLE+SoyLE group had a change of 1 mg/dL from start to end of LE therapy. These findings are likely due to the compassionate nature of this clinical trial, the patients that received FishLE alone were older and sicker than those in the FishLE+SoyLE group. Furthermore, only two out of 17 infants (12%) in the FishLE+SoyLE group received both lipid emulsions throughout the entire therapy. This was because at the time of enrollment in the compassionate trial, the FDA protocol had a safety measure to discontinue SoyLE and continue with FishLE alone if the infant’s DB increased beyond 4 mg/dL; therefore, the majority of infants in FishLE+SoyLE group were those that received SoyLE and FishLE simultaneously at any given time. Nonetheless, infants who continue to receive SoyLE in combination with FishLE do not have worse liver function as previously thought and perhaps FishLE intake alone or in combination provides the beneficial effects for cholestasis. Additionally, we compared the monthly average and total cumulative enteral caloric intake at 2–4 weeks before therapy started, 4 weeks and 8 weeks of therapy, during the entire length of their therapy, and their entire hospital stay, we found no significant differences between groups. These results suggest that caloric restriction may not be a major barrier to the use of FishLE as long as carbohydrates are increased if lipids are restricted to achieve a beneficial liver function.
This study has several important limitations that need to be taken into consideration. First, there was a large Hispanic population found in both groups and this may not be an equal representation of all racial/ethnic groups. Another limitation faced in this study was high loss to follow up, especially in the FishLE group. This complicates interpretation of the long-term outcomes we attempted to assess as we may have lost some of the sicker infants. Finally, we could not obtain maternal fatty acid or lipid profile information to examine if any of the differences observed in our infants may be due to differences in the transport of lipid metabolites that occurs between the fetus and its mother during gestation. These differences make it difficult to separate the relative contributions of prenatal factors versus severity of illness versus LE therapy on the outcomes examined. However, these infants were enrolled at a mean 50 days of life and antenatal factors may have less of a contribution to the long-term outcomes.
In conclusion, we did not find evidence for substantial differences in lipid profiles and short-term clinical outcomes in infants exposed to higher cumulative amounts of FishLE+SoyLE versus those exposed to lower cumulative amount of IV lipids to include FishLE alone. Plasma concentrations of almost all fatty acids were similar between groups at the end of the study period and there were no differences in caloric intake nor growth between the groups.
Footnotes
Acknowledgments
We would like to thank the Pediatrics Research Coordinator, Robin Tragus, NICU dietitians Rachel Jacob, R.D., Elizabeth Lavender, R.D. and the NICU pharmacists, Kay Greene and Nicole Greene for their support in identifying these patients for enrollment in the study.
Financial disclosure statement
The authors have no competing financial interests in relation to the work described.
Other disclosure statements
University Health System Research Grant and Discretionary funds from the Division of Neonatology at University of Texas Health Science Center at San Antonio.