
Abstract
BACKGROUND:
Neonatal antibiotic use is associated with a greater risk of nosocomial infection, necrotizing enterocolitis, and mortality. It can induce drug-resistant pathogens that contribute to increased neonatal morbidity/mortality, healthcare costs, and length of stay. Prior to the antibiotic stewardship program, decisions to obtain blood cultures and empiric antibiotics for possible Early-onset Sepsis (EOS) in late preterm and term infants upon NICU admission were provider-dependent rather than algorithm-based. We aimed to decrease empiric antibiotic prescription from 70% to 56% (20% decrease) in infants ≥34 weeks gestation admitted to the NICU.
METHODS:
The stewardship initiative comprised the following practice changes: (1) use of the Neonatal Sepsis Risk Calculator (SRC); and (2) a 36-hour time-out for prescribed empiric antibiotics. Data was retrospectively collected and analyzed for inborn infants pre-intervention (January 2015–December 2015; n = 263) and post-intervention (August 2016–September 2017; n = 279). Data regarding compliance with the new antibiotic guideline were collected and disseminated to the team every week. Overlap between CDC guidelines and calculator recommendations were studied.
RESULTS:
Pre-and post-intervention outcomes were analyzed using chi-square tests. There was a significant post-intervention reduction in the rate of both antibiotic prescriptions (29.4% decline; 70.3% vs. 49.6%; p < 0.001) and sepsis evaluations (24.3% decline; 90.9% vs. 68.8%; p < 0.001). No difference (p = 0.271) in culture-positive EOS cases was observed. There was 92% overlap in blood culture recommendations and 95% overlap between antibiotic recommendations when current CDC guidelines were compared to the SRC.
CONCLUSION:
A significant reduction in antibiotic use and sepsis evaluations was achieved for late preterm and term infants upon NICU admission. No clinical deterioration occurred in post-intervention infants who did not receive antibiotics. There is significant overlap between CDC guidelines and SRC recommendations.
Introduction
Antibiotics are the most commonly prescribed medication in the neonatal intensive care unit (NICU) [1]. Yet, the Centers for Disease Control and Prevention (CDC) report that 25–50% of all antibiotics prescribed in the U.S. are unnecessary [2]. This is alarming because inappropriate antibiotic use is associated with the development of antibiotic resistant organisms as well as an increased incidence of ototoxicity [3], necrotizing enterocolitis, and death [4]. Moreover, alteration of the gut microbiome following antibiotics is linked to adverse long-term outcomes, including childhood obesity [5] and asthma [6]. Additionally, mother and infant often have to be separated during antibiotic treatment which adversely affects breastfeeding and bonding practices [7]. To prevent serious consequences such as these, the federal government released a National Action Plan in 2015 to establish antibiotic stewardship programs in all acute care hospitals and reduce 20% of inappropriate antibiotic use in inpatient settings by 2020.
In the NICU, antibiotic usage frequently begins soon after birth to combat Early-onset Sepsis (EOS), defined as bacteremia or bacterial meningitis that occurs prior to 72 hours of age [8]. The bacteria [most commonly Group B Streptococcus (GBS), followed by Escherichia Coli] [9] are believed to be transferred from mother to infant before or during delivery [10]. Because neonates often have non-specific EOS symptoms that can make diagnosis and timely treatment challenging, it is common practice upon NICU admission to obtain blood cultures and initiate a 48-hour antibiotic treatment while culture results are pending. Despite a reduction in EOS incidence over the last decade, a sepsis evaluation for suspected EOS remains one of the most commonly performed NICU workups. Furthermore, substantial variation in EOS-risk identification, evaluation, and antibiotic prescription continues to exist among healthcare providers [11]— especially for infants born at 34 weeks gestational age (GA) or older. Therefore, the primary aim of this NICU quality improvement (QI) initiative was to reduce unnecessary EOS antibiotic usage by 20% in this population of infants.
Methods
The NICU Antibiotic Stewardship QI Initiative involved three distinct phases: 1) development of a QI team and determination of the pre-intervention EOS antibiotic usage rate; 2) selection of interventions and pre-intervention planning, including leadership support and staff education; and 3) intervention implementation and pre-/post-analysis. The local Institutional Review Board determined that this quality improvement initiative did not qualify as human subject research.
Phase 1: Development of a QI team and determination of pre-intervention antibiotic usage rate
Development of a NICU antibiotic stewardship QI initiative team
An interdisciplinary NICU Antibiotic Stewardship QI Initiative Team was established with a representative(s) from each of the following specialties: neonatologists, neonatal-perinatal medicine fellows, a pediatric infectious disease physician, an infection prevention expert, a neonatal clinical pharmacist, a pharmacist dedicated to antibiotic stewardship practices, health informatics and technology personnel, as well as NICU nursing leaders and staff. Biweekly Team meetings were held to identify opportunities for improving clinical EOS evaluation and antibiotic prescribing practices. The Team developed an EOS guideline based on a new evidence-based intervention and made plans to roll it out following comprehensive NICU provider education and training. (The Team would later modify the guideline in order to incorporate a second intervention nine months after the EOS guideline was first initiated in the NICU.)
Setting
This QI Initiative was implemented at a level III NICU that admits approximately 650 infants per year. All inborn infants at 34 6/7 weeks GA or younger are admitted directly to the NICU after delivery until medically-appropriate discharge to either the Mother/Baby Unit (MBU) or home. Indications for the NICU admission of late preterm and term infants (GA 35 0/7 weeks and older) include respiratory distress, symptomatic or refractory hypoglycemia, temperature instability, and a prenatal diagnosis or suspicion of congenital anomalies.
Baseline EOS management – pre-intervention
Each month, about 20 infants in the EOS population of interest (those born at 34 weeks GA or older) are admitted to the NICU. Prior to the Antibiotic Stewardship QI Initiative, a large proportion of these infants (i.e., those who presented with respiratory distress, hypoglycemia, or temperature instability) received a limited sepsis evaluation [complete blood count (CBC) with differential and blood culture upon admission].
The standard empiric antibiotic regimen included four doses of Ampicillin 100 mg/kg IV every 12 hours and two doses of Gentamicin 4 mg/kg IV every 24 hours. Antibiotics were usually discontinued after 48 hours, but could be extended at the discretion of the provider for up to 7 days, even in culture-negative infants (e.g., infants with subtle clinical signs, abnormal chest X-ray/CBC). This practice resulted in a high antibiotic usage rate.
Also, all infants born to mothers with suspected or proven chorioamnionitis were treated with empiric antibiotics for 48 hours, as recommended by the CDC. Asymptomatic infants who had exposure to chorioamnionitis were allowed to remain in the MBU during antibiotic treatment.
Determination of pre-intervention antibiotic usage rate
The 2015 calendar year was selected as the study time frame for the pre-intervention cohort. A detailed retrospective medical record review between January and December 2015 revealed a baseline antibiotic usage rate of 70% in the EOS population of interest. This finding determined that the post-intervention rate must be 56% or lower to achieve a 20% decrease. Therefore, the primary aim of the NICU Antibiotic Stewardship QI Initiative was to reduce EOS-related antibiotic usage by 20% (from 70% to 56%) in infants born at 34 weeks GA or older.
Phase 2: Selection of interventions and pre-intervention planning
Intervention and rationale #1: Early-onset sepsis risk calculator
A multivariate Neonatal Early-onset Sepsis Risk Calculator (SRC) was created in 2014 to provide clinicians with an evidence-based tool for determining EOS risk in infants 34 weeks and older [12]. The SRC was developed using analytic risk stratification methods based on perinatal risk factors as well as clinical presentation. Recently published research has demonstrated the SRC’s success in safely reducing unnecessary antibiotic administration in various clinical settings [13, 14], and its online access makes it readily available to clinicians everywhere (https://neonatalsepsiscalculator.kaiserpermanente.org/).
Prior to the creation of the SRC, two sets of national medical and federal agency-endorsed EOS management guidelines for clinicians were published by the CDC [15] and the American Academy of Pediatrics’ Committee on the Fetus and Newborn (AAP COFN) [16]. As a result, a wide variation in EOS evaluation practices exists across the country, and this lack of consistency was reflected in a 2017 survey of U.S. nurseries. Of the 81 nurseries polled within the Better Outcomes through Research for Newborn Network, 65% used either the CDC’s 2010 Perinatal GBS guidelines or the AAP COFN Statements to evaluate neonates, 14% used the SRC, and only 3% used clinical observation alone [11].
Another concern related to current EOS evaluation and management practices involves the CDC guidelines which recommends administration of empiric antibiotics to all infants born to mothers suspected of maternal chorioamnionitis. Although maternal chorioamnionitis can increase EOS risk, the actual incidence of EOS in this population is low. Therefore, this blanket approach may result in the unnecessary treatment of several low-risk infants [17].
Intervention and rationale #2: 36-hour antibiotic time-out
The use of automated blood cultures has made it possible to detect bacterial growth within 24–36 hours from incubation [18–20]. Shorter time to obtain blood culture results enables the institution of shorter durations of empiric antibiotic coverage. Therefore, the Team planned to decrease the empiric antibiotic coverage to 36 hours (from 48 hours). This automatic 36-hour time-out was identified as a second Antibiotic Stewardship QI Initiative intervention.
Pre-intervention planning, leadership support, and staff education
Support for this Antibiotic Stewardship QI Initiative from hospital leadership and administration was easily obtained due to system-wide focus on improving antibiotic usage practices. The next Team priority was NICU healthcare provider education because conventional EOS practice decisions had been primarily dependent on provider preferences.
The Team hosted several education sessions to share baseline data and discuss the newly developed EOS guideline and SRC intervention with NICU physicians, fellows, residents, nurse practitioners (NNPs), and nursing staff. They were also educated in detail about the SRC and its appropriate use in various clinical scenarios. A shortcut to the SRC link was installed in all NICU computers for easy access, and the CDC national incidence of 0.5/1000 live births was used as the SRC’s pre-test probability. The electronic medical record (EMR) was modified to embed pop-up boxes to record SRC scores within inpatient progress notes. In addition to ensuring EOS documentation, the pop-up boxes also served to reinforce providers’ use of the SRC intervention, enable comparisons to CDC recommendations, and document rationale if the EOS guideline was not followed.
Nine months later, the Team modified the EMR again prior to rolling out the 36-hour time-out intervention. The EMR admission antibiotic order was adjusted to allow only 36 hours of empiric antibiotic prescription, consisting of three doses of ampicillin 100 mg/kg every 12 hours and one dose of gentamicin 5 mg/kg [21]. The Team also conducted education sessions for NICU staff before implementing the 36-hour time-out.
Phase 3: Intervention implementation and pre-/post-implementation analysis
Intervention #1: Early-onset sepsis risk calculator – August 2016
The new EOS guideline with the SRC intervention was formally implemented in August 2016. Every week, the EMR progress notes of eligible infants were reviewed to monitor accuracy of SRC scores, documentation completeness, and EOS guideline compliance. This information was compiled into compliance reports that deidentified infants, but included admitting provider names, specified whether or not each provider was compliant with the guideline, and listed the EMR-documented reason for deviation, if applicable. These reports and antibiotic usage data were shared with all attending physicians, fellows, NNPs, and leadership staff on a weekly basis via email. Quarterly antibiotic usage progress reports were disseminated to NICU leadership as well as nursing staff.
There were a few instances of discrepancy between CDC and SRC recommendations in well-appearing late preterm infants whose only risk factor was inadequate receipt of antenatal GBS prophylaxis (the CDC advised blood culture but SRC advised clinical observation only). Providers were advised to adhere to CDC recommendations until January 2017 when the guidelines were modified to follow SRC recommendations exclusively.
Intervention #2: 36-hour time-out – May 2017
The Team implemented the 36-hour Antibiotic time-out in May 2017 (Fig. 1). All infants were reevaluated at 36 hours to determine if the initial antibiotic order required extension based on culture results and/or clinical status. Reeducation sessions were conducted for physicians as well as nursing staff with this modification of the EOS guideline.
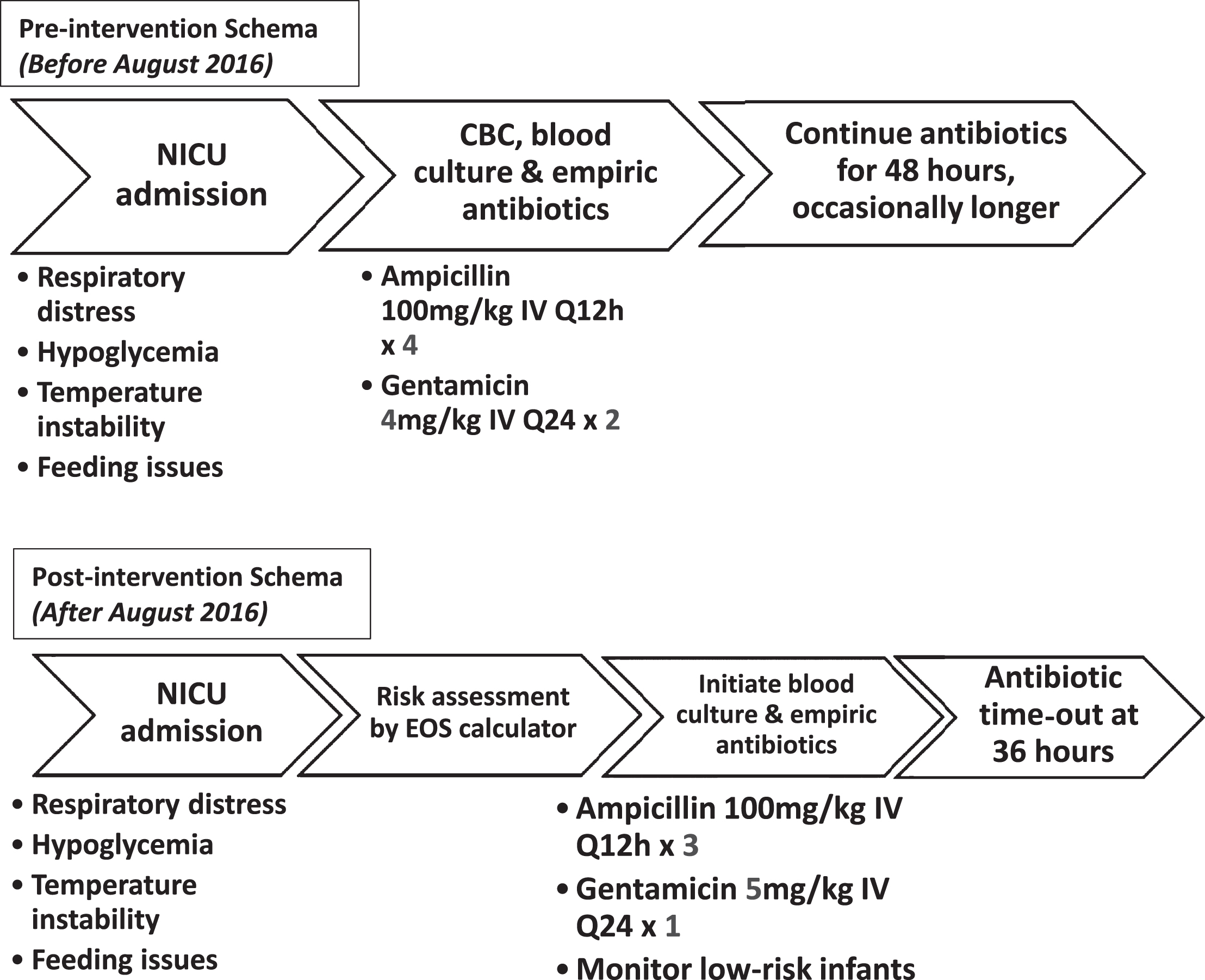
EOS antibiotic prescription regimens pre-and post-intervention.
Overall, 25 months of data were collected on the EOS population of interest (infants born at 34 weeks GA or older) throughout the 32-month Antibiotic Stewardship QI Initiative study period. The pre-intervention group included all inborn infants admitted between January 2015 and December 2015 (months 1–12), and the post-intervention group included infants admitted from August 2016 through September 2017 (months 20–32). No data was collected between January 2016 and July 2016 (months 13–19). During this interim period, the Team planned intervention strategies and provided staff training. As part of their training, providers were able to use the SRC, albeit inconsistently, prior to its formal implementation in August 2016.
EOS population and data collection
The medical records of 671 inborn infants were reviewed for eligibility, and a total of 539 infants were included in the analyses (Fig. 2). Maternal and infant EMRs were reviewed for data pertaining to demographics, perinatal EOS risk factors, clinical findings, SRC scores, cultures, antibiotic use, and average length of stay (ALOS). The information was entered into a secure Research Electronic Data Capture (REDCap) database [22]. SRC scores were calculated and recorded for all infants at birth, after the NICU admission clinical exam, and, if admitted from labor and delivery, at 4 hours of life (HOL) as well. Infants who did not automatically qualify for NICU admission (i.e., 35weeks GA and older) at birth and were transferred from the MBU later often lacked complete vital sign documentation at 4 HOL; hence, a clinical score at 4 HOL was not able to be performed on these infants. CDC recommendations based on EMR data were also entered into REDCap.

EOS population studied pre-and post-intervention.
EOS definition
EOS was defined as a pathogenic bacteria-positive blood culture collected in the first 72 hours of life. Blood cultures that were positive for Coagulase-negative staphylococci or other common skin-commensal bacteria from clinically stable infants who were not treated with systemic antibiotics were considered to be a contaminant and were not included as EOS cases.
Primary and secondary outcomes
The antibiotic prescription rate for suspected EOS was evaluated as the primary outcome. Secondary outcomes included the proportion of infants undergoing initial sepsis evaluation, clinical deterioration in untreated infants, repeat sepsis evaluations, extension of antibiotics beyond 72 hours of life (HOL), untreated infants with positive culture, as well as overlap and discrepancies between current CDC guidelines and SRC recommendations.
Process and value measures
Compliance with the EOS guideline was used as a process measure, and ALOS was tracked as a value measure.
Concomitant hospital antibiotic stewardship initiative
Of note, at the same time that the NICU Antibiotic Stewardship QI Initiative Team implemented the EOS guideline in August 2016, the hospital’s Labor and Delivery Department also began its own antibiotic stewardship initiative. They instituted the National Institute of Child Health and Human Development Workshop’s Triple I diagnostic criteria recommendations [23]. The Triple I diagnostic criteria seek to provide clinicians with an improved method for evaluating the risk of chorioamnionitis.
Statistical analysis
Descriptive statistics were used to summarize data with frequencies and percentages for categorical variables and means and standard deviations (SD) or medians and interquartile range (IQR) for continuous variables. Comparisons between maternal and infant characteristics were tested using Chi-square analysis. Pre-and post-group comparisons for antepartum antibiotic use, sepsis evaluations, antibiotic prescription, antibiotic administration beyond 72 HOL and compliance with the new EOS guideline were tested using independent groups Student’s t-test or Mann-Whitney U test depending on normality of data. SRC scores were not normally distributed, thus the Spearman rank correlation coefficient or Mann-Whitney U test were used to test the associations of SRC scores with positive blood cultures, antibiotic use and ALOS. Compliance with CDC guidelines and SRC recommendations were analyzed descriptively with overlap and discrepancies. A p-value <0.05 was considered statistically significant. Statistical process control with our primary outcome measure of antibiotic prescription rate for suspected EOS was displayed on a p-chart. Analyses were conducted with SPSS (version 22.0) (IBM Corp. Released 2013. IBM SPSS Statistics for Windows, Version 22.0. Armonk, NY: IBM Corp) and Excel, version 15.32 (Part of Microsoft Office 365 Professional Edition) with QI macros. Microsoft; 2017.
Results
EOS population characteristics
Table 1 describes EOS population characteristics. There was no significant difference between pre-and post-intervention groups relative to demographics, mode of delivery, gestational age, weight, GBS status or Apgar scores.
EOS population sample characteristics
EOS population sample characteristics
*Independent t-tests used for data shown as means. All other data, shown as frequencies was analyzed using the Chi-square method. EOS: Early-onset Sepsis; IQR: interquartile range.
The distribution of SRC scores was evaluated by non-parametric testing, and no significant differences were found between pre-and post-intervention groups at any time points (Table 2). In both groups, SRC scores at birth as well as on admission were significantly higher among infants with documentation of suspected chorioamnionitis (median score at birth 0.1 vs. 0.6, median score on admission 3.08 vs. 0.27; p < 0.001). Birth SRC scores were not associated with sepsis evaluation (p > 0.05), antibiotic prescription (p > 0.05), or bacteremia (p > 0.05) (Tables 3 and 4). Higher clinical SRC scores on admission were associated with blood culture acquisition and antibiotic prescription. However, these scores did not correlate with positive culture results. Higher birth and clinical SRC scores on admission correlated with a longer NICU ALOS (Table 4).
SRC score distribution in pre-and post-intervention groups
SRC score distribution in pre-and post-intervention groups
SRC: Sepsis risk calculator; HOL: hours of life.
Correlation between SRC scores and clinical practice patterns (Mann-Whitney)
SRC: Sepsis risk calculator.
Correlation between SRC scores and clinical practice patterns (Pearson Coefficient)
*Correlation is significant at the 0.01 level (2-tailed). The above table compares correlation between SRC scores at birth and on admission with obtaining blood culture, culture-proven EOS, antibiotic use in 72 hours as well as length of stay. Higher SRC scores at birth and on admission correlated with longer average length of stay in both pre-and post-intervention groups. EOS: Early-onset Sepsis; SRC: Sepsis risk calculator; HOL: hours of life; ALOS: Average length of stay.
Primary outcome
A 29.4% decline in antibiotics prescribed for suspected EOS was exhibited in the post-intervention group (p < 0.001) (Table 5 and Fig. 3). Figure 3 shows a p-chart based on univariate antibiotic prescription data over the 32-month Antibiotic Stewardship QI Initiative.
Comparison of antepartum and postnatal antibiotic pre-and post-intervention
Comparison of antepartum and postnatal antibiotic pre-and post-intervention
*Calculated only for infants who stayed in the NICU beyond 72 hours of life. EOS: Early-onset Sepsis; HOL: hours of life.

Control p-chart demonstrating decreasing antibiotic prescription rate per month. Upper and lower confidence limits demonstrate 3-σ variation per month. • Data points during months 25 to 37 indicate a sustained decrease in antibiotic use following the implementation of the stewardship program. EOS: Early-onset Sepsis calculator.
After the practice change, there was a decline in the proportion of infants receiving antibiotics. This decline was sustained for several months until the end of the study period.
The changes in clinical practices resulted in a 24% decrease in blood cultures obtained for an EOS evaluation (p < 0.001) (Table 5). There was a significant decrease in both the number of repeat sepsis evaluations beyond 72 HOL (p = 0.022) and extension of systemic antibiotics (p = 0.012). However, no significant difference in culture-proven EOS between groups was observed. There was one case of EOS in the post-intervention group, and the infant was treated with empiric antibiotics according to SRC recommendations.
Process and value measures
The post-intervention group was also evaluated for compliance with the practice change. Out of 276 cases, 220 (79.7%) were compliant with sepsis evaluation and 248 (89.9%) were compliant with SRC antibiotic recommendations. ALOS was studied as a value measure; and there was no significant difference between pre-and post-intervention groups (p = 0.822) (Table 1).
Comparison of SRC and CDC recommendations
In 94.8% (511/539) of cases, the SRC and the CDC guidelines had identical recommendations for antibiotic use (Table 6). There was a 92% (496/539) overlap in recommendations for obtaining blood culture.
Comparison of CDC and SRC recommendations for EOS antibiotic treatment
Comparison of CDC and SRC recommendations for EOS antibiotic treatment
*Denotes number on instances with overlapping recommendations. SRC: Sepsis risk calculator; EOS: Early-onset Sepsis.
A comparison of the data pre-and post-EOS guideline implementation revealed a 29.4% decline in antibiotic usage in infants born at 34 weeks GA or older. Therefore, the NICU Antibiotic Stewardship QI Initiative’s primary aim of a 20% reduction was achieved and exceeded. Routine use of the EOS guideline was also associated with a significant decrease in the number of blood cultures drawn on infants in the EOS population of interest as well as fewer repeat sepsis evaluations and prolongation of antibiotics beyond the initial NICU admission order. These three additional findings may be an indirect benefit of using an objective, algorithm-based SRC risk assessment versus a subjective provider preference-based determination. We believe that educating the providers about the evidence-based SRC and the current literature supporting its use, instilled a greater sense of confidence in their initial EOS evaluation and management, thereby decreasing their previous tendency to repeat sepsis evaluations for those infants with initial negative blood cultures.
While use of the SRC has been prospectively studied at an academic newborn nursery [13, 24] as well as through retrospective reviews [13], prospective data from this QI initiative augments existing evidence by demonstrating successful SRC utilization in infants admitted to a level III NICU of a community-based teaching hospital that also serves as a major regional referral center. To our knowledge, no studies or QI projects have prospectively evaluated the SRC in infants between 34-and 35-weeks GA within the high-risk setting. Also, no studies to date have compared SRC recommendations against the CDC’s 2010 Perinatal GBC guidelines for every eligible infant. Our comparison showed an extensive overlap. Of the 539 EMR cases that were reviewed, the SRC and CDC were 92% congruent in their recommendations to obtain blood cultures, and 95% congruent in recommending empiric antibiotics. Despite the substantial overlap, a significant reduction in sepsis evaluations and antibiotic prescriptions was achieved.
Perhaps the greatest concern associated with the SRC is delay in EOS identification and antibiotic treatment [25, 26]. During the QI study period, there were only five cases of culture-proven EOS: four cases during pre-intervention and one during post-intervention. The EOS case in the post-intervention group was identified as high EOS-risk by the SRC, and treated with empiric antibiotics according to SRC recommendations. Thus, no EOS cases were missed as a result of incorporating the SRC into our EOS guideline. Additionally, the provision of continuous monitoring in the NICU greatly reduced the risk that clinical deterioration would not be detected in time.
Another concern addressed in the literature involves the lack of studies assessing the SRC’s potential effect on long-term outcomes, including ALOS [26]. Although this was beyond the scope of our Antibiotic Stewardship QI Initiative, we did evaluate ALOS as a value measure and found no significant difference between pre-and post-intervention groups. However, our data was not matched for other cofounding factors that could impact ALOS due to our retrospective comparative cohort.
Our NICU Antibiotic Stewardship QI Initiative can be a model for other institutions to use when implementing similar practices in their NICUs. Hospital and NICU leadership support for the initiative was relatively simple to obtain as it aligned with our health care system’s focus on antimicrobial stewardship, including infection control and minimizing drug-resistant strains. We found that leadership support made it easier for us to implement changes and track progress.
Staff education and tracking EOS guideline compliance were the most labor intensive and time-consuming tasks of the QI initiative. However, sharing of weekly feedback reports with providers helped to create continued awareness of the new EOS guideline. We also felt inclusion of provider names in the reports along with information about the providers’ compliance was integral to ensuring successful integration of the new practice and enhanced conformity in the NICU.
Modification of the EMR was key to reinforcing SRC use and facilitated documentation. It also ensured consistency of antibiotic ordering and reduced errors when the second intervention was rolled out. The 36-hour time-out was easily implemented in our NICU. We did not note any concern among providers, and none of the infants’ antibiotics were extended to 48 hours for a “rule-out EOS” diagnosis. Moreover, no infants experienced clinical deterioration because of the shortened duration of antibiotics.
The authors also witnessed that the careful evaluation of EOS sepsis risk and judicious use of antibiotics required by the new EOS guideline positively affected how providers diagnosed and treated other conditions. The Antibiotic Stewardship QI Initiative actively reinforced and consistently promoted good stewardship practices in the NICU.
This QI study has several limitations. It is limited in that we report only one center’s experience coupled with a relatively short post-intervention period. Also, because of the lack of local data regarding the EOS incidence in our NICU population, we used the national incidence of EOS (0.5/1000 live births) as the pre-test probability for the SRC.
We were only able to achieve approximately 90% compliance with the EOS guideline following implementation of the NICU Antibiotic Stewardship QI Initiative. The authors believe that this may have been due to a learning curve among physicians and expect it to improve over time. Yet, this also provided us with additional opportunities to reeducate the staff and share data with the rest of the team.
Interestingly, we found that recorded SRC scores did not correlate with positive cultures. However, this could be due to limited sample size and low incidence of EOS in the era of GBS screening and antepartum antibiotics.
Next steps include the transition to random audits and quarterly antibiotic use data that will be shared with NICU physicians and nursing staff. Our health informatics team is assisting us in incorporating the SRC directly into our EMR, in addition to the pop-up documentation boxes. We are also in the process of collecting longitudinal EOS incidence data in order to accurately predict risk in our population.
Finally, we are working toward extending use of the EOS guideline into the MBU for well-appearing infants with chorioamnionitis. Challenges for this step include education of community pediatricians and substantial nursing support to perform frequent vital sign checks while the infants stay with their mothers.
Future studies should include a cost analysis. In addition to the incalculable value to the infant due to less painful procedures, as well as an intact microbiome and uninterrupted maternal bonding, a reduction of EOS antibiotic usage should translate to decreased healthcare costs associated with nursing procedures, laboratory testing, and medication costs.
Conclusions
Incorporation of the SRC and 36-hour antibiotic time-out in a tertiary care NICU was feasible, well-received, and did not contribute to any missed EOS diagnoses, delayed treatment, or clinical deterioration. Furthermore, there was an associated 29.4% decline in antibiotic usage in infants born at 34 weeks GA or older.
We also noted a significant overlap between CDC and SRC recommendations for empiric antibiotic use in this population.
Funding
No commercial or grant funding support was received for this QI initiative.
Disclosure statement
All authors have no financial relationships relevant to this article to disclose.
Footnotes
Acknowledgments
The authors would like to acknowledge the Russell Center for Research and Innovation Summer Research Internship Program for their assistance in providing personnel support for data collection and Yi Li, MS for her support with statistical analysis.