
Abstract
The mechanisms of perinatal stroke are poorly understood but preclinical studies point to the crucial role of perinatal inflammation. Carotid artery occlusion represents a very rare and severe cause of perinatal stroke. We describe two cases diagnosed with extensive ischemic stroke due to carotid artery occlusion. In both cases, we demonstrated placental vasculopathy. High levels of C-reactive protein in mother and/or neonates suggested inflammatory mechanism as a potential trigger. Both cases underwent hypothermic treatment without complications because of initial diagnosis of perinatal asphyxia. The prognosis at the time of the last follow up was severe including cerebral palsy, epilepsy and cognitive impairment. Our cases contribute to the actual debate on pathogenic mechanisms and treatment options for this rare condition.
Introduction
Perinatal arterial ischemic stroke includes a variety of conditions in which blood flow disruption in a cerebral artery, occurring between 20 weeks of fetal life and 28 days of postnatal life, damages a focal area of cerebral tissue [1]. Clinical signs occurring in the neonatal period with MRI evidence of acute stroke [2, 3] define neonatal arterial ischemic stroke (NAIS). NAIS must be distinguished from presumed perinatal arterial ischemic stroke in which clinical manifestations present after the neonatal period (usually motor asymmetry after few months of life) and which is associated to brain imaging evidence of remote infarction, which could have occurred in the perinatal period [4].
Carotid artery occlusion is a very rare and severe cause of NAIS, less than 20 cases have been reported so far, representing 0.5% of all documented causes [5 –16]. The clinical presentation can be nonspecific with early seizures within a general clinical picture of encephalopathy [17]. Thus, encephalopathy resulting from large vessel occlusion and massive hemispheric ischemia can be misdiagnosed as hypoxic ischemic encephalopathy [18]. Moreover, birth asphyxia is a risk factor for perinatal stroke and the two conditions may coexist. Nowadays neonates fulfilling criteria of post asphyxia encephalopathy undergo hypothermic treatment, but hypothermia is not at present recommended for perinatal stroke. In the literature, there is no clear consensus on the best treatment for NAIS; possible options such as antithrombotic therapy and therapeutic hypothermia are at present not included in the International Guidelines [19]. However, the adult literature discusses on their use in severe cases such as large and/or multiple embolic strokes in the setting of extra cerebral large vessels thrombosis [20].
The mechanisms of NAIS have been considered multifactorial but recently research pointed to systemic and local inflammation as fundamental independent risk factors [21 –23]. These results have important implications for the management of patients, since infection and inflammation could be the target of neuroprotective treatments.
The aim of the present study was to contribute to the to the actual debate on pathogenesis and treatment options for NAIS by reporting on maternal and perinatal risk factors and long-term outcome of two neonates with carotid artery occlusion who were treated with hypothermia.
Methods
Out of a population of 104 neonates enrolled in the neonatal intensive care unit of the University Hospital of Padua for hypothermic treatment between February 2009 and December 2016, two suffered from carotid artery occlusion and stroke. Maternal and neonatal data, placental histology and brain and arterial MRI data were collected. Our institutional criteria of enrollment for hypothermia have been previously described. The follow-up program for neonates managed with hypothermia at our Institution includes neurological examination at 1, 3, 6, 9, 12, 18, 24, 36 months, and at 4 and 5 years of age and also standardized assessment of development with the Griffiths Mental Development Scales.
The coagulation panel adopted at our institution includes: prothrombin time, partial thromboplastin time, protein S activity and antigen, protein C activity and antigen, APC sensitivity ratio, Leiden factor V° mutation, prothrombin gene mutation G20210A, coagulation factors II-VIII-IX-XI, fibrinogen, plasminogen activator, plasminogen activator inhibitor, anti-cardiolipin antibodies (IgG and IgM), anti beta2 glycoprotein 1 antibodies (IgG and IgM).
The hospital ethical committee approved the retrospective review of the clinical records, imaging and cognitive data for this study.
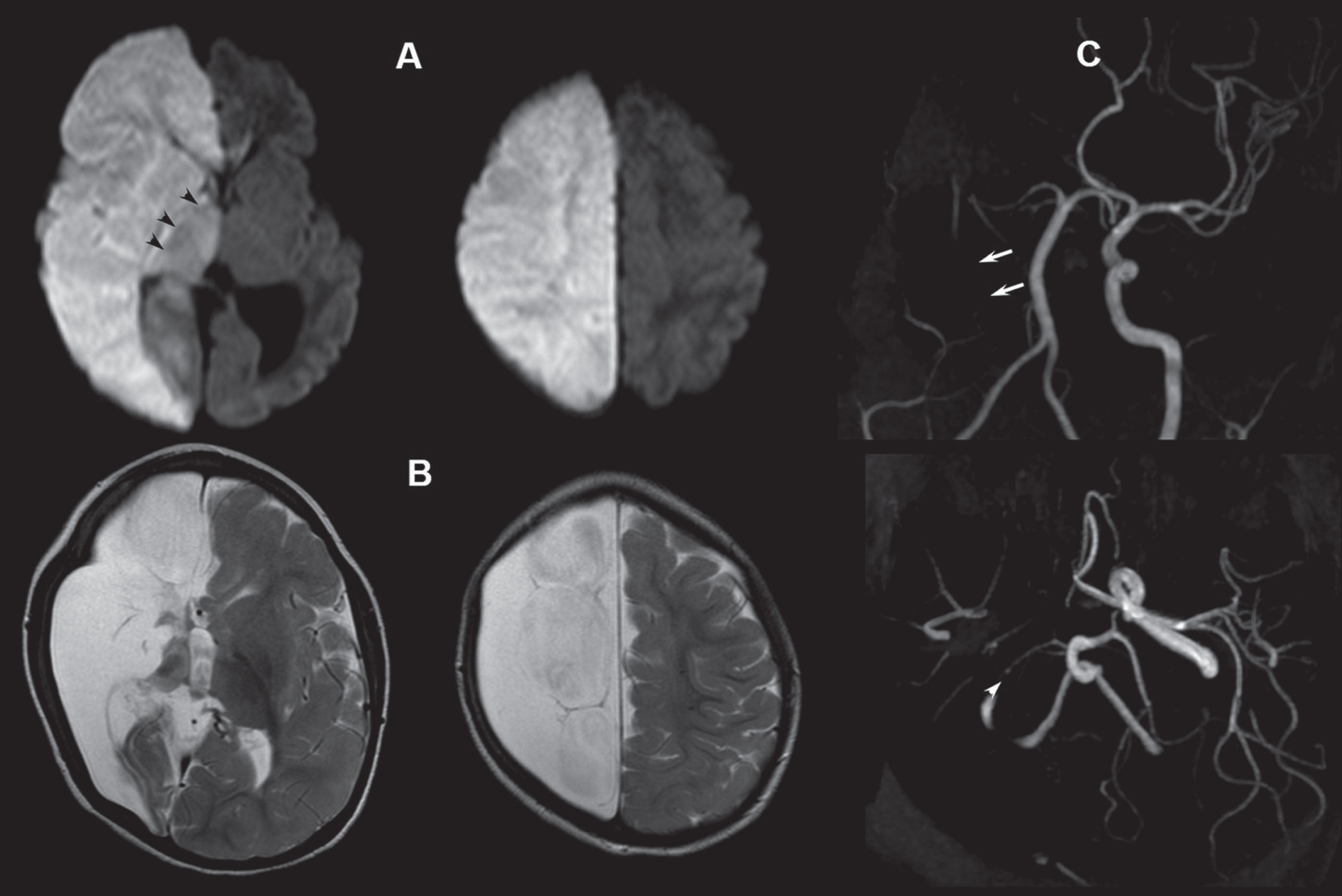
Hemispheric ischemic area with no recanalization of right internal carotid artery. Legend: A) Diffusion weighted images one day after birth showing hyperintensity of the right hemisphere consistent with ischemia. The right thalamus (black arrowheads) and the right cerebral peduncle (not shown) are also hyperintense suggesting that the stroke was recent but not hyperacute (prenatal stroke?). B) Axial T2-weighted images at the age of 2 months showing the evolution of the ischemic regions of the right hemisphere into diffuse encephalomalacia and atrophic right thalamus. C) MR angiography at the age of 2 months showing the persisting absence of the right internal carotid artery (short arrows) and the narrowing of the right posterior cerebral artery (arrowhead) due to decreased metabolism (the same artery was pseudo-hypertrophic during the acute phase because of compensatory activation, not shown).
Case 1
A female infant was born at 40+4 weeks in a first level hospital, following an uneventful pregnancy. She underwent emergency cesarian section due to dynamic dystocia and a pathological cardio-tocographic tracing. Birthweight was 2900 g (10th centile), length 52 cm (50th centile) and head circumference 35 cm (50th centile). Apgar scores were 6-7-7 (1’–5’–10’). She needed positive pressure ventilation with laryngeal mask for respiratory depression at birth. Funicular pH was 7.01 and BE -16.2. Troponin level was 0,29 ug/l (normal values 0–0,045). She developed moderate encephalopathy (Sarnat score 2). At three hours of life, she developed focal seizures. Phenobarbital was started with good seizure control. She also had a high temperature (CT 38.2°C) from the first day of life and persistently elevated level of C-reactive protein (14,2 mg/dl at birth and 21,2 mg/dl at 24 hours). Her platelet count was 100.000 m3; she was treated with antibiotics. Hemoculture was negative. She was promptly transferred to a central hospital where therapeutic hypothermia was started at 5:30 hours of life. Cranial ultrasounds on the first day of life showed diffuse hyperechogenicity on the right hemisphere and median line shift to the left. Brain CT scan revealed an extensive ischemic area in the right hemisphere, involving anterior and middle cerebral artery territories, and showed a marked cerebral regions shift to the left; a thrombus in the right carotid artery was also identified. Magnetic resonance imaging (MRI) performed on the same day confirmed the extensive stroke involving the right hemisphere, sparing the occipital areas and showed brain swelling resulting in an 8 mm shift to the left of the median cerebral regions. The intracranial tract of the right internal carotid artery was poorly visualized on magnetic resonance angiography. Diffusion-weighted imaging revealed Wallerian degeneration of the corticospinal tract along the brainstem, suggesting prenatal vascular insult (Fig. 1). Supra-aortic vessels echo Doppler, performed on day 2, revealed internal right carotid artery occlusion just after its origin, with preservation of the right subclavian and anonymous artery. Supra-aortic vessels echo doppler and T1W fat-sat sequence on day 6 MRI showed an unchanged thrombosis of the right internal carotid with no evidence of carotid wall dissection. Coagulation studies showed reduced levels of protein C and protein S, subsequently normalized at the age of 10 months.
The histological examination of the placenta showed a thrombotic process of the fetal vessels. Laboratory tests performed on maternal blood were unremarkable except for an elevated level of C-reactive protein (78.99 mg/L) and a high level of anti-cardiolipin antibodies (IgG 22.44 GPL, normal values <15.00).
MRI follow-up at 2 and 15 months of age showed the expected evolution of the hemispheric ischemic area with no recanalization of the right internal carotid artery (Fig. 1).
At 15 months, there was an additional evolution of the ischemic lesion involving the right hemisphere, sparing the thalamus and part of the occipital and temporal lobes. The right internal carotid artery as well as the anterior and middle right cerebral arteries had not re-canalized (images not shown).
At one year, the developmental assessment with the Griffiths Mental Development Scales indicated impairment (<3° percentile) in all subscales (locomotors, personal-social, hearing and language, eye-hand co-ordination and performance). Motor functions were the most impaired, with impact on the maturation of all other functions. Language repertoire was poor, the visual contact was rare and interaction abilities were impaired. The child developed focal epilepsy at the age of 3 years, well controlled by carbamazepine.
At 4 years, the neurological examination revealed bilateral spastic cerebral palsy with a more severe impairment of the left side, cognitive deficit, strabismus and low vision.
Case 2

Extra and intra-cranial occlusion of the left internal carotid, stenosis of right posterior cerebral artery and, in lesser extent, of the right sylvian branches. Legend: A) Axial diffusion weighted images at the age of 2 days showing acute ischemia in the left hemisphere (temporal-mesial and basal occipital lobes were partially spared, not shown); note the concomitant ischemia in the contralateral occipital lobe; a further small acute ischemia was observed in the right inferior parietal lobule in the supply territory of the middle cerebral artery, not shown, suggesting a multi embolic pathogenesis. B) Axial T2-weighted images at the age of 12 days showing the evolution into encephalomalacia of the ischemic regions. C) MR angiography at the age of 2 days showing the occlusion of the left internal carotid artery; note the pseudo-hypertrophy of the left intracranial arteries, more evident at the level of the middle cerebral artery branches (*). Note also the distal occlusion of the right posterior cerebral artery (arrowhead), consistent with a multi embolic pathogenesis.
A female infant born at 38+4 weeks by Cesarean section due to pathological cardio-tocographic tracing. Pregnancy elapsed with intrauterine growth restriction from 34th week gestation. Birth weight was 2730 gr (10th centile), length was 47 cm (10th centile) and head circumference was 33.5 (10–25th centile). Apgar scores were 5–8–8 (1’–5’–10’). Funicular pH was 6.94, EB -19.6 mmol/L. At birth, she presented hypotonia, apnea and cyanotics, and required resuscitation with endotracheal suction of stained amniotic fluid. She had moderate grade encephalopathy (Sarnat score 2). Therapeutic hypothermia begun at 4:30 hours of life. The troponin level on day 1 was high (0.451 ug/L), but returned to normal range on day 3. The electrocardiogram showed signs of transient myocardial ischemia. There was an increased level of C-reactive protein (19 mg/L at birth, increased at 40 mg/L at 24 hours of life) for which she received antibiotic therapy. Hemoculture was negative. During the first day of life the electroencephalographic monitoring showed electrical seizure patterns both in left temporal regions and, independently, in right occipital regions, with absent or subtle clinical correlate. She received phenobarbital treatment and seizures ceased. Transcranial ultrasounds performed on day 1 showed periventricular hyperechogenicity, particularly in the parietal region. The MRI performed on day 2 showed multiple strokes: a large left hemisphere ischemia involving both the middle and anterior cerebral territories and other ischemic lesions in the territories of right middle cerebral artery. Willis circle study showed extra and intra-cranial occlusion of the left internal carotid, stenosis of the right posterior cerebral artery and, to a lesser extent, of the right sylvian branches (Fig. 2).
The coagulation panel was normal for gestational age. The placenta was small and showed various wide, white areas, suggesting ischemic origin. Coagulation studies performed on maternal blood showed increased levels of IX factor, XI activity, fibrinogen and plasminogen activity, while lupus anticoagulant, antinuclear and anti-phospholipid antibodies were negative.
The MRI follow-up at 22 days of life showed regular evolution of the ischemic areas. Magnetic resonance angiography revealed initial re-canalization of intracranial left internal carotid. Clinical follow up at one year of age using the developmental assessment with Griffiths Mental Development Scales showed impairments (<3° percentile) in 4/5 subscales (locomotors, personal-social, eye-hand co-ordination and performance), while linguistic abilities were adequate. Motor was the most affected function; all non-motor functions where motor disabilities could have an interference on the tests were also slightly involved but, with good interaction abilities. At 2 years of age, Griffiths Mental Development Scales showed an adequate development of linguistic and personal/social abilities. Motor functions persisted in being severely impaired (<3° percentile) due to right hemiparesis.
At 4 years, clinical examination revealed unilateral spastic cerebral palsy (right hemiplegia), cognitive impairment and difficulties in modulation of emotional states.
The two cases of neonatal arterial ischemic stroke reported in the present study occurred because of fetal-placental thromboembolic events associated with carotid artery occlusion, a rare but severe cause of neonatal arterial ischemic stroke. Perinatal inflammation, probably induced by infection was a common mechanism in both cases. Indeed, they had persistently an elevated level of c-reactive protein and underwent antibiotic treatment; case 1 had also fever and her mother had elevated level of C-reactive protein.
Both cases had evidence of maternal hypercoagulable status. The mother of case 1 had high levels of anti-cardiolipin antibodies. The mother of case 2 had increased levels of IX factor, XI activity, and fibrinogen and plasminogen activity. Follow-up studies were not performed precluding the possibility of confirming a permanent thrombophilia status. Moreover, in both cases histological examination of the placenta showed thrombotic/ischemic changes suggesting placental vasculopathy. MRI evidence of Wallerian degeneration of the corticospinal tract along the brainstem suggested a prenatal vascular insult in case 1 while pregnancy elapsed with intrauterine growth restriction from 34th week in case 2.
Other etiologies specifically implicated in the occlusion of large extracranial vessels such as the internal carotid artery, were ruled out in our patients. Traumatic dissection of the internal carotid artery, can occur secondary to traumatic events during delivery, particularly in the case of fetal macrosomia and shoulder dystocia [5, 9]. In rare cases, spontaneous carotid artery dissection may be an intrinsic fetal and placental vascular disease. Both our cases underwent cesarean section. In the case with emergency cesarean section and dynamic dystocia, brain MRI and magnetic resonance angiography investigations did not detect signs of traumatic injury to the carotid artery wall. They did not have fetal subarachnoid and intraventricular hemorrhage therefore other causes of carotid artery occlusion such as vascular spasms were unlikely [11].
In view of new treatment strategies, it is important to understand causative events underlying perinatal stroke. The hypothesis of a multifactorial etiology involving maternal, placental, fetal and neonatal risk factors is at present a major focus of research [5]. The most recent evidence, however, points to maternal-fetal inflammation as the single most important independent mechanism of NAIS [20]. Infection/inflammation can explain the co-occurrence of other important risk factors for stroke. Indeed, birth asphyxia, is also a powerful inducer of sterile inflammation and inflammation has a pro-coagulant effect. Our two cases of perinatal arterial ischemic stroke from carotid occlusion confirm the role of pre/perinatal inflammation, within a multifactorial etiology. We searched and found signs of inflammation even in the case with absent fever as well as additional risk factors such as maternal thrombophilia, placental vascular pathology and hypoxic ischemic encephalopathy.
One other interesting feature of the present study is that we recruited our two cases from a prospective single center cohort of patients, fulfilling criteria for therapeutic hypothermia; they constituted about 2 % of the total population of patients recruited. Both of them had a combination of carotid artery stroke, depression at birth with metabolic acidosis and encephalopathy. In the first hours of life, the diagnosis of hypoxic ischemic encephalopathy was hypothesized, making them eligible for hypothermic treatment. This treatment is not at present recommended for perinatal stroke; however, the clinician’s decision after the diagnosis of stroke was to continue the treatment, monitoring closely all possible side effects. We could not prove possible benefits; however, therapy was without complications.
Perinatal stroke in the context of carotid artery occlusion represents the most severe type of arterial ischemic stroke occurring in the perinatal period. Prognosis is worse than other types of NAIS [5]. Accordingly, both our cases developed cerebral palsy. Moreover, in both cases re-canalization of affected arteries did not occur. Treatment of perinatal stroke is a challenge for clinicians. The main issue in stroke management is to preserve brain tissue by restoring cerebral blood flow; the treatment of choice in adults is systemic thrombolysis with tissue plasminogen activator, in a 3- to 4.5-hour time window. In children and even more in neonates, there is no consensus on both intravenous thrombolysis as well as endovascular therapy of arterial stroke, because of the substantial lack of data on efficacy and safety [25].
Furthermore, in neonates, timing is a crucial issue considering that stroke often occurs before birth, as in our cases, hindering any acute strategy. In addition, International Guidelines for treatment of perinatal arterial ischemic stroke do not recommend anticoagulation in arterial stroke [26]. Even if stroke recurrence is negligible in NAIS, neonates may undergo thrombus propagation particularly when spontaneous recanalization does not occur in the first week of life. Anticoagulation therapy was recently introduced in neonatal cerebral sinovenous thrombosis [26], to prevent thrombus propagation, but not in arterial ischemic stroke. Considering the outcome severity and the lack of recanalization of occluded vessels in our patients, we question if antithrombotic therapy could have been of benefit. Indeed, our cases confirm that NAIS subtypes have different prognosis. Stroke subtype should guide a decision-making tailored to the patient. In conditions with the worst prognosis, such as carotid artery occlusion, particularly when recanalization does not occur, or thrombosis progresses, anticoagulation could be an option.
Conclusions
Our study points to the importance of searching for carotid artery thrombosis in the work up of perinatal stroke, particularly when atypical presentation and/or multiple vascular territories are involved. Information on placental pathology as well as on maternal thrombophilia must be part of the routine workup. Perinatal inflammation must also be appreciated both in mothers before birth and in neonates, because of its importance in pathogenesis and of its implications for prevention and management. The poor long-term prognosis in perinatal stroke due to carotid artery occlusion prompts further research efforts, to evaluate treatment strategies that could improve the outcome.
Disclosure statements
Financial disclosure statement: no authors declared potential or actual interests are disclosed.
Statements of human rights: For this type of study, formal consent is not required.