
Abstract
OBJECTIVES:
Neonatal seizures are significant cause of neonatal mortality and morbidity. Current study was planned to study prevalence of adverse outcomes in neonatal seizures and identify its predictors.
METHODS:
This observational descriptive study was carried out on 220 neonates with seizures. Neonates who succumbed to illness/ death before investigations, or whose maternal records were incomplete were excluded. Blood sugar, serum calcium, serum electrolytes, and USG skull were done in all patients. CT scan, MRI and inborn errors of metabolism profile were done as and when indicated. Adverse outcomes were defined as death, phenobarbitone non responders, or abnormal examination at discharge. Antenatal, perinatal and neonatal predictors of adverse outcomes in neonatal seizures were evaluated.
RESULTS:
Out of 220 neonates with seizures 76(34.5%) had adverse outcomes. Very low birth weight babies (≤1500 gm) [OR 1.27(CI 0.57–2.84)], microcephaly [OR 5.93 (CI 0.55–64.41)], Apgar score≤3 at 5 minutes [OR 11.28(CI 14.18–30.45)], seizure onset within 24 hours [OR 5.99(CI 12.43–14.78)], meningitis [OR 2.63(CI 0.08–6.39)], septicemia [OR1.22(CI 0.45–3.31)] and abnormal cranial USG [OR 7.95(CI 12.61–24.22)] were significant predictors of adverse outcomes in neonates with seizures.
CONCLUSION:
Prematurity, very low birth weight, birth asphyxia, meningitis, septicemia and abnormal USG could predict adverse outcomes in neonatal seizures. Improved antenatal and neonatal clinical practices may help reduce adverse outcomes in these patients.
Introduction
Neonatal seizures are most frequent during the first week of life. Incidence of neonatal seizures is 1–5/1000 live births in Western countries [1]. National Neonatal Perinatal Database (NNPD) collected from 18 centres in India reported an incidence of seizures as 10.3/1000 live births [2]. Clinically neonatal seizures can be categorized into tonic, clonic, myoclonic or subtle and reflect pre, peri- or postnatal insult on developing central nervous system (CNS). Common causes of seizures in full-term neonates include hypoxic-ischemic encephalopathy, stroke, cerebral malformations, and metabolic disorders. In preterm neonates, intra-ventricular hemorrhage (IVH), periventricular leukomalacia (PVL), and infections happen to be the leading causes [3–6].
Neonatal seizures carry a significant risk of death or subsequent disability and can independently confer adverse neurodevelopmental outcomes like cerebral palsy, epilepsy and developmental delay in high-risk neonates. Recent studies have shown a decline in mortality rates and also a reduction in long term squeal, prognosis being worse in preterms than term neonates [6, 7]. Neonatal factors namely, prematurity (≤32 weeks), very low birth weight (≤1500 gm), microcephaly, macrocephaly, Apgar score≤3 at 5 minutes, seizure onset within 24 hours of birth, meningitis and septicaemia were identified as significant predictors of adverse outcomes which include mortality, neurological impairment and epilepsy [8–10]. Abnormal radiological and EEG findings were also found to be strongly associated with adverse outcomes in neonates with seizures [10–11]. Refractory neonatal seizures requiring multiple anticonvulsants and phenobarbitone refractoriness are other adverse outcomes that were predicted by seizure type, background EEG and neurologic examination [12, 13].
Worldwide around 2.6 million neonates die every year. Despite all the measures being taken for reducing neonatal mortality, more than 60 countries are not likely to meet the target of sustainable development goals (SDG) [14]. Developing countries are struggling to bring down neonatal mortality rates and to achieve survival without neurological impairment [15]. Seizures being the significant contributor to neonatal illnesses, an understanding of adverse outcomes and their predictors in neonatal seizures may help in identifying the preventable causes in these countries and plan interventions accordingly. Thus, we planned the study with objectives of determining the proportion of neonatal seizures with adverse outcomes and to find the predictors of adverse outcomes in neonatal seizures.
Participants and methodology
This observational study was conducted in intramural Neonatal Intensive Care Unit (NICU) of department of Pediatrics in a tertiary care medical college-affiliated hospital over a period of 18 months (November 2017 to April 2019). A written informed consent was obtained from the parents or guardian of the participant. An approval from the ethical committee of the institute was obtained before enrolling the study participants.
All the neonates who got admitted to intramural NICU with neonatal seizures, witnessed by the treating doctor were included in the study. Neonates who succumbed to illness before investigations and those with poor maternal records were excluded.
Detailed methodology
All the babies with neonatal seizures were managed as per NICU protocol. A complete evaluation of the neonates was done that included a detailed search for ante-partum and intra-partum risk factors, birth details, and neonatal examination. Blood sugar, serum calcium, and ultrasonography (USG) cranium was done in all neonates. Cerebrospinal fluid (CSF) examination, computed tomography (CT) scan, magnetic resonance imaging (MRI) and inborn errors of metabolism (IEM) panel was done as and when indicated.
Adverse outcomes in neonatal seizures were defined as death during hospital stay, phenobarbitone non- responders, and babies who were neurologically abnormal at discharge. Phenobarbitone non-responders were the neonates who did not respond to intravenous phenobarbitone even after 40 mg/kg of drug in three aliquots (20 mg/kg, followed by 2 doses of 10 mg/kg each) and required second line anticonvulsant. A baby was labelled to be neurologically abnormal at discharge, if was not able to accept breast feeds, and/or had tone abnormalities and/or abnormal neonatal reflexes. The outcome was assigned after confirmation by two independent consultants who were not directly involved in the study.
Sample size
Considering the proportion of neonates with adverse outcomes as 25%of all neonatal seizures, α error of 5%, 95%level of confidence, precision of 12%, sample size was calculated to be 51 neonates with adverse outcomes. To get 51 neonates with adverse outcomes, we had to enrol a total of at least 204 neonates with seizures. We decided to enrol 220 neonates for the study.
Statistical analysis
The data was entered into MS Excel and was analysed using SPSS 20.0 software. Descriptive statistics was applied for estimating proportion. For analysing the predictors of adverse outcomes, the likely variables were analysed initially in a univariate model. Variables with P values < 0.05 were further analysed using the logistic regression model, and independent variables were identified after controlling co-variates.
Results
During the period of enrolment (February 2018 to September 2018) we had total of 3,514 admissions in our intramural NICU, out of which 284 had neonatal seizures. Sixty-four neonates were excluded and 220 neonates were enrolled in the study. Of 220 neonates included in the study, 144 (65.4%) had seizures without adverse outcomes and 76 (34.6%) neonates had seizures with adverse outcomes (Fig. 1).
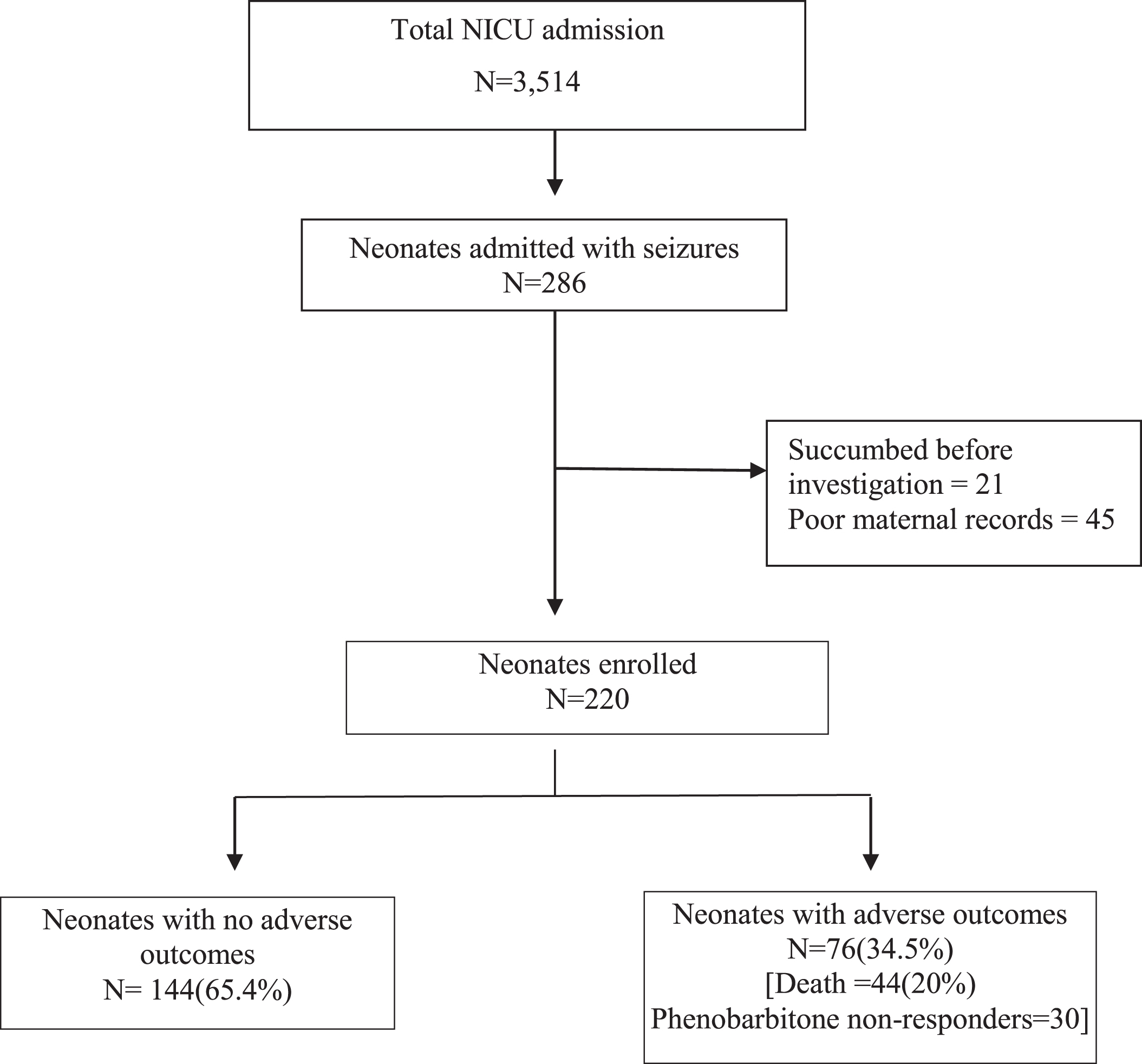
Outcome of neonates with seizures during study.
Baseline parameters of the neonates are shown in (Table 1). Among these mean gestational age (30.21 vs 34.35; P value 0.016), mean head circumference (30.22 vs 31.17; p value 0.010), Apgar score at 5 minutes (5.55 vs 8.56; p = 0.000), age at onset of seizures (37.37 vs 60.28; p value 0.001) and sPO2 (90.83 vs 93.44; p = 0.001) were significantly less in neonates with adverse outcomes than those without adverse outcomes.
Baseline parameters of neonates with seizures
*P-value < 0.05 is significant. Independent t-test for comparison of the mean (SD) HR- heart rate, RR- respiratory rate, Temp- temperature, Spo2-arterial oxygen saturation.
Among antenatal and intra-natal factors (Table 2), maternal age less than 18 years (OR 1.95; CI-0.55–6.99) and being primigravida (OR 1.23; CI-0.68–2.20) were associated with adverse outcomes. Neonates with gestational age≤32 weeks, microcephaly, macrocephaly, APGAR score≤3 at 5 min, seizure onset within 24 hours, bulging anterior fontanel, presence of septicemia and congenital brain malformation had higher odds of having adverse outcomes. Abnormal radiological investigations including ultrasound as well as CT scan were also found to be significantly associated with adverse outcomes. Abnormal MRI was also seen in significantly higher numbers in neonates with adverse outcomes, but odds could not be calculated as it was not done in any of the babies without adverse outcomes (Table 3).
Antenatal and intranatal predictors for adverse outcomes in neonatal seizures
*P value < 0.05 significant; # significant Omnibus test for Odds ratio. LSCS- Lower segment cesarean section.; CI- Confidence interval.
Neonatal predictors of adverse outcomes in neonatal seizures
*P value < 0.05 significant, # significant Omnibus test for Odds ratio HC- head circumference CI- Confidence interval.
1The predictors which were found to be significant after univariate analysis were further analysed using multivariate analysis and adjusted odds ratio was calculated for these factors as depicted in Table 4. Presence of microcephaly (adjusted odds ratio 5.93, CI 0.55–64.41); APGAR≤3 at 5 min (adjusted OR 11.28; CI 4.18–30.45): seizure onset within 24 hours (adjusted OR 5.99; CI 2.43–14.78); presence of septicemia (adjusted OR 2.63; CI 1.08–6.39) and abnormal USG skull (adjusted OR 7.95; CI 2.61–24.22) were found to be significant predictors of adverse outcomes in neonatal seizures.
Multivariate analysis of predictors of adverse outcomes in neonatal seizures
*Significant adjusted odds ratio, HC- head circumference, USG –ultrasound, CI-confidence interval.
Present study showed that 34.5%of the neonates admitted with seizures had adverse outcomes in the form of phenobarbitone non-responsiveness, mortality, and abnormal neurological examination at discharge. Microcephaly, Apgar≤3 at 5 min, seizure onset within 24 hours, presence of septicemia and abnormal USG skull were significant predictors of adverse outcomes in neonatal seizures.
In our study, 20%of neonates with seizures expired during hospital stay. This number is comparable to the studies by Anand, et al. [9] and Ronen GM, et al. [16] who reported 17.2%and 24%mortality, respectively. Overall incidence of adverse outcomes is higher in our study as we also included phenobarbitone non-responsiveness and abnormal neurological examination at discharge as poor outcome. Spagnoli et al. reported phenobarbitone refractoriness in 20%of neonatal seizures, with seizure type, background EEG and neurological examination to have correlation with this [13]. Neonates who have difficult to control seizures are likely to suffer recurrent hypoxic damage, leading to worse prognosis in these babies.
Prematurity and very low birth weight are significant predictors of adverse outcomes in neonatal seizures. The results are in line with studies by Al Momen et al. [7], Anand et al. [9], Iwami et al. [17] and Malmquist et al. [18]. Hypoxic-ischemic encephalopathy (HIE) has also been found to be one of the significant predictors of adverse outcomes in neonatal seizures. Lai et al. reported that Apgar score of 0–3 at 5 minutes had 100%association with adverse outcomes [10]. Similar observations were made by Cavallin, et al. and Chen, et al. in a cohort of asphyxiated neonates [19, 20].
Maternal age less than 18 years and primigravida were found to be associated with adverse outcome in contrast to study by Gebremariam, et al. [21], where neonates born to mothers with > 5 children had poor outcome. We did not have mothers aged > 35 years in our study cohort. Other antenatal risk factors namely, short stature and chorioamnionitis were significantly more in neonates with adverse outcomes, but due to lesser number of mothers with these conditions, statistically significant association with adverse outcomes could not be derived.
Various intrapartum factors which were comparable among both the groups were placental abruption, cord prolapse, intrapartum fever, the prolonged second stage of labour, and mode of delivery as against a previous study that reported multiple gestation (OR1.74), previous cesarean section (OR1.35), and prolonged second stage (OR1.81) as significant predictors of neurological outcome in neonates with seizures [21].
Bulging fontanel was present in 14 babies with adverse outcomes as compared to 5 babies in the other group, hydrocephalous being the most common cause. Congenital malformations were also associated significantly with adverse outcomes. This was similar to study by Sheth, et al. [22]. Authors reported that congenital malformations were seen in 5–9%of neonates with seizures and these disorders had a poor neurodevelopmental prognosis. Intraventricular haemorrhage was also associated with neurological impairment at later stage [23]. Abnormal radiological investigations, like USG cranium and CT brain were associated adverse outcomes. Severe EEG and radiological (USG and CT) abnormalities have been significantly associated with adverse outcomes previously also [9].
Significant variation has been reported in predictors of adverse outcomes among neonates with seizures. This may be due to difference in the population of enrolled participants in terms of gestational age, underlying aetiologies as well as the investigations performed and the outcomes addressed. Garfinkle, et al. developed a five-point scoring system which could predict adverse outcomes with 81%sensitivity and 84%specificity [24]. Pisani, et al. also devised a scoring system using six variables that could serve as prognostic indicator after neonatal seizures [25]. Development of prediction rules or scoring systems where significant predictors can be used to assess prognosis can be the step ahead.
Strength of our study is the assessment of wide range of antepartum, intrapartum and neonatal risk factors for assessment of prognosis. Also, we included phenobarbitone non-responsiveness as one of the adverse outcomes, which has not been widely studied. Major limitation of our study is it being localized to single hospital catering to urban slum. Extensive multicenter studies focussing on development of prediction rules may be of further help in determining adverse outcomes in neonates with seizures. These predictors can be used to plan early interventions for managing at risk babies.
Disclosures
There is no conflict of interest. No funding was involved in the study. The study conformed to all the ethical standards.