
Abstract
Pneumothorax in preterm infants is associated with an increased risk of chronic lung disease, intraventricular hemorrhage and mortality. In mechanically ventilated preterm infants, for the management of tension pneumothorax if needle aspiration is not successful a thoracostomy is needed. In the last two decades management of tension pneumothorax has changed from the use of traditional chest tubes to percutaneous pigtail catheter thoracostomy (PPCT) as the most commonly used technique. When compared to placement of traditional chest tubes, PPCT is touted as being faster requiring, less analgesia and less training for proficiency and having fewer complications. There are only infrequent reports of complications with this procedure. Here, a rare complication, which previously has only been reported at autopsy, is described in an extreme preterm with prompt diagnosis and early management.
Keywords
Abbreviations
Percutaneous pigtail catheter thoracostomy
Pleural pigtail catheter
Introduction
The incidence of pneumothorax in preterm infants has been decreasing after increased use of maternal steroids, early administration of surfactant and reduced need for mechanical ventilation [1]. Pneumothorax is associated with an increased risk of intraventricular hemorrhage, chronic lung disease and mortality [1]. In the presence of hemodynamic or respiratory compromise, the management options include needle aspiration and chest tube placement. Instead of needle aspiration, use of venous catheters or angiocaths, which can be left in place, for a short period of time and even attached to an underwater seal, is an equally effective alternative [2]. Due to the rapidity, ease of placement, and apparent lack of complications, the standard chest tube placement using blunt dissection, has been supplanted, in many centers by the percutaneous pigtail catheter thoracostomy (PPCT). Here we describe a unique complication encountered in an extreme preterm infant with tension pneumothorax with the use of PPCT.
Case summary
A premature infant born to a 22-year old Caucasian woman, with a history of chronic abruption and longstanding oligohydramnios due to prolonged rupture of the membranes for over 6 weeks. An hour prior to delivery, the mother received steroids, antibiotics and Magnesium. She went on to deliver a male infant precipitously at 25 weeks’ gestational age, who needed mechanical ventilation. He had Apgars of 5 and 7 at 1 and 5 minutes respectively and birth weight of 640 grams. The patient had intra-tracheal surfactant but was switched from a conventional ventilator to a high frequency oscillator, secondary to high mean airway pressure requirements and poor oxygenation. A chest X-ray showed a left tension pneumothorax and needed immediate needle aspiration due to decompensation. (Fig. 1A) Due to re-accumulation of air, an 8.5 Fr pigtail catheter was placed percutaneously in the left pleural cavity using a Seldinger technique. A follow up film showed complete resolution and adequate placement of pigtail catheter. (Fig. 1B, C) There was improvement in clinical status, but an echocardiogram confirmed the suspicion of pulmonary hypertension, with suprasystemic pulmonary pressures. In addition, an echogenic indentation of the left ventricle (LV) could be seen due to the pigtail pleural catheter (PPC) coursing from the pleura through pericardial space (Fig. 2). Under echocardiographic guidance, a bubble study using agitated saline injected into the chest tube, showed immediate opacification of the pericardial space, confirming communication between the catheter and pericardium. When the pigtail catheter was pulled back by 0.75 cm there was improved LV filling without compression defect with hemodynamic improvement.

(A) Plain AP Chest radiographs showing left pneumothorax on left with mediastinal shift. (B) Chest AP radiograph showing resolution of pneumothorax after placement of pigtail pleural catheter with optimal placement. (C) Lateral chest radiograph with optimal placement of PPC and adequate resolution of pneumothorax.
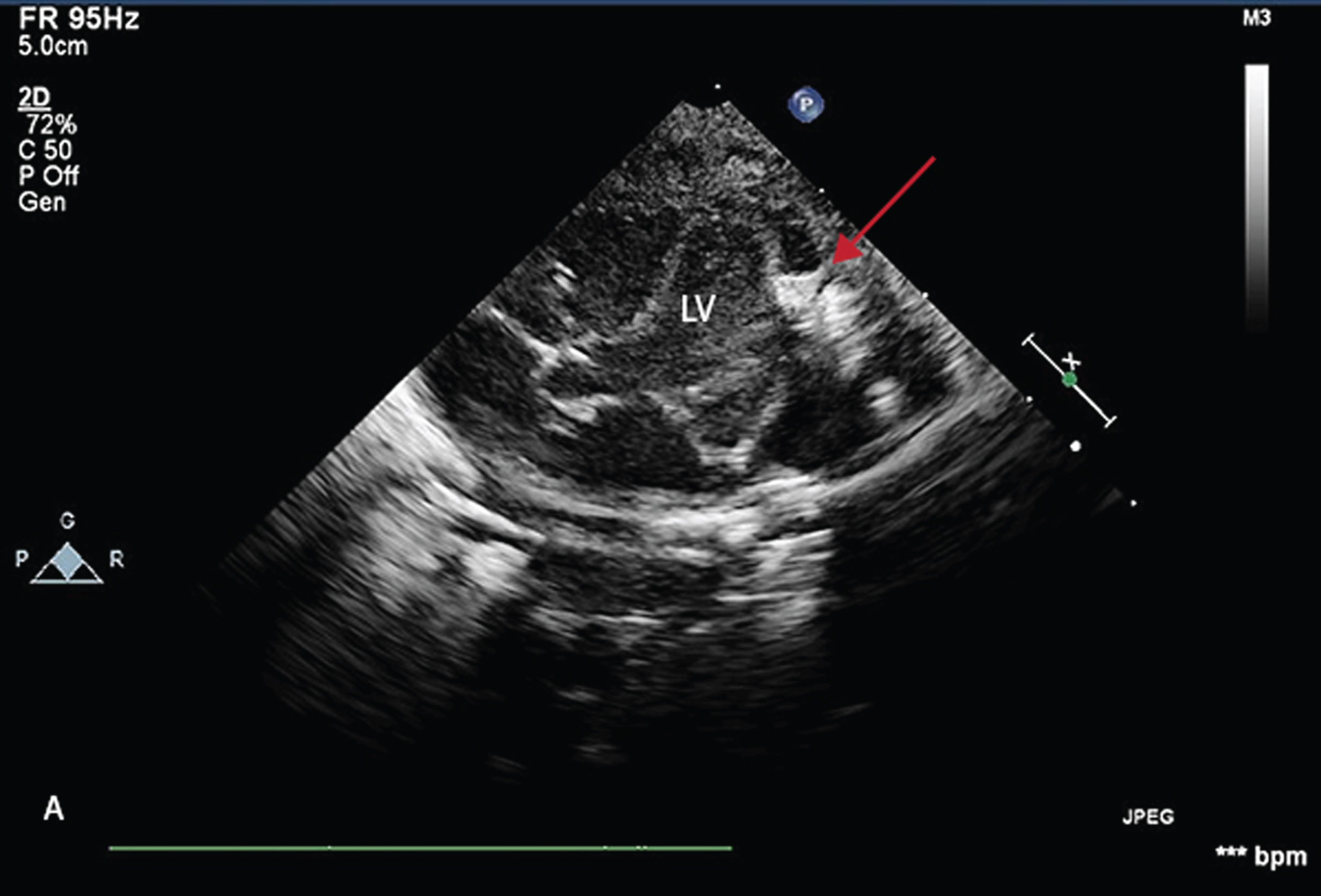
Echocardiogram Subcostal view: Echocardiogram showing catheter placed in pericardium and indenting left ventricular wall (arrow).
The patient subsequently had a routine hospital course and was discharged home at a corrected gestational age of 41 weeks with discharge weight of 2925 and needed minimal home oxygen, as the family was moving to a higher altitude. At follow-up at 18 months the patient was weaned off oxygen by six months and had mild, predominantly motor delay, on a Bailey III neurodevelopmental assessment.
The spectrum of severity of pneumothorax ranges from an asymptomatic one noted incidentally on a chest radiograph, to a large tension pneumothorax causing respiratory failure. Management depends on severity, but a tension pneumothorax requires urgent decompression. Traditional techniques of draining a pneumothorax including use of a trocar to place chest tubes have been abandoned. Thoracostomy, utilizing blunt dissection has complications, is considered time consuming and has limitations due to its need for extensive training for new learners.
Initial reports by Furman in 1986, showed that PPCT, using a modified Seldinger technique, was less traumatic, quicker and with less complications when compared to standard tube thoracotomy [3]. Using an airtight plastic bag attached to the insertion needle to confirm pleural placement, it showed similar benefits in small children [4]. After its utility was later confirmed in neonates with pneumothoraces and pleural effusions, PPCT is now widely used and has been shown to be equally effective and with shorter procedure time in children and neonates with pneumothorax or pleural effusion [5, 6].
The common complications of PPCT are failure to drain, dislodgement, kinking, hemorrhage and infection [7, 8]. It is possible that it is more common than recognized, as clinical and radiological findings are non-specific and difficult to ascertain in critically ill patients. More recently there have been reports of lung lobe perforation, pericardial and mediastinal injury in preterm infants. Unfortunately these complications are not detected until autopsy [7, 8].
In infants, due to the thin chest wall, the proximity of vital tissues and the fragility of the pleura and lung tissue, make these complications more likely. When using PPCT, after insertion of the needle and introduction of the guide wire perforation of pleura, lung parenchyma, pericardium and other viscera is possible in extreme preterm infants. It is a likely, but not often reported cause for bronchopleural fistula. Fatal complications like air embolism can occur when the lung is punctured and gas bubbles could enter a pulmonary vein and lead to cerebral, coronary and other forms of air embolism. This could happen when the atmospheric pressure exceeds the pulmonary venous pressure during inspiration or by causing a broncho-venous fistula or due to a paradoxical embolism and is not often diagnosed [9, 10]. Even after an uneventful removal of a pleural pigtail catheter, patients have developed tension hemothorax, requiring evacuation [11].
Bedside point of care ultrasonography by non-radiologist clinicians is becoming more popular and is considered part of basic medical education. Ultrasound (US) guidance for placement of wire-guided PPCT is associated with a decreased risk of complications [10, 13]. In a report of a preterm infant who had persistent desaturation where clinical examination, trans-illumination and chest radiography did not detect a pneumothorax, a chest US showed evidence of a pneumothorax that was promptly treated [14].
In the case described above even after clinical improvement and radiological resolution of the pneumothorax, diagnosis of this complication would not have been detected, if an echocardiogram had not been done. Every medical procedure is fraught with potential complications and every effort is made to mitigate this risk. Limiting the depth to which the wire is advanced would be an option but the chances of having a subcutaneous placement could possibly increase. Another possible option would be to utilize bedside US for all PPCT. In this case the pericardial penetration was identified when the indentation of the LV was noted on echocardiogram and then confirmed by the bubble study, with prompt intervention to manipulate the PPC and subsequent improvement of hemodynamic status and ultimate survival of the infant. Every effort should be made to prevent or reduce the occurrence of pneumothorax and lung injury in the first place by practicing gentle resuscitation and low tidal volume ventilation.
Funding source
No funding was secured for this study.
Financial disclosures
No financial relationships relevant to this article to disclose.
Conflict of interest
No conflicts of interest to disclose.