
Abstract
Peripherally inserted central catheters (PICC) are the mainstay of central venous access in preterm infants, and one of the common procedures performed in neonatal intensive care unit (NICU). Complications of PICC include infection, mechanical dysfunction, thrombosis, migration, and extravasation of the infusate. In this report, we describe a case of PICC inserted from an upper extremity with migration into the inferior vena cava (IVC) and the hepatic vein associated with extravasation of the total parenteral nutrition (TPN) into the peritoneum and the liver. This case highlights the vigilance required not only to insert but for the maintenance of PICC to prevent complications associated with migration of PICC.
Keywords
Introduction
PICC are widely used in the NICU for long-term venous access mainly to deliver total parenteral nutrition. Common sites of PICC insertion in neonates are veins in the upper extremity, lower extremity and in the scalp. Recent studies showed no difference in the overall incidence of catheter related complication rate between upper extremity and lower extremity PICC insertion sites but extravasation was more often with lower extremity insertion [1, 2]. Catheter migration and extravasation of infusate into the pleural space, pericardial space, abdominal cavity, and spinal canal has been reported previously as a complication of PICC [3]. In most of the reported cases the central catheter was inserted in the lower extremities but in our patient catheter tip migrated into the IVC from an upper extremity inserted PICC, which is unusual and has not been reported earlier.
Case report
An Asian baby boy born to 30-year-old G4P0031 mother with severe preeclampsia at 28 weeks of gestation by cesarean section. Baby was appropriate for gestational age with birth weight was 980 grams. Apgar was three and seven at first and fifth minutes. Baby required intubation in delivery room and was extubated at seven days after which he was stable on room air CPAP. A single lumen one French (28 G, Premicath, Vygon, Germany) PICC was inserted on the right upper extremity on fifth day of life for the central venous access. Position of tip of the catheter was confirmed with x-ray, and radiologist reported the tip at the junction of the right atrium and the superior vena cava (SVC) (Fig. 1). Patient received a forty-eight-hour antibiotic course for presumed sepsis at admission and was treated for PDA with improvement around end of first week of life. The infant otherwise had a stable course for the first two weeks of life and continued to receive TPN through the PICC.
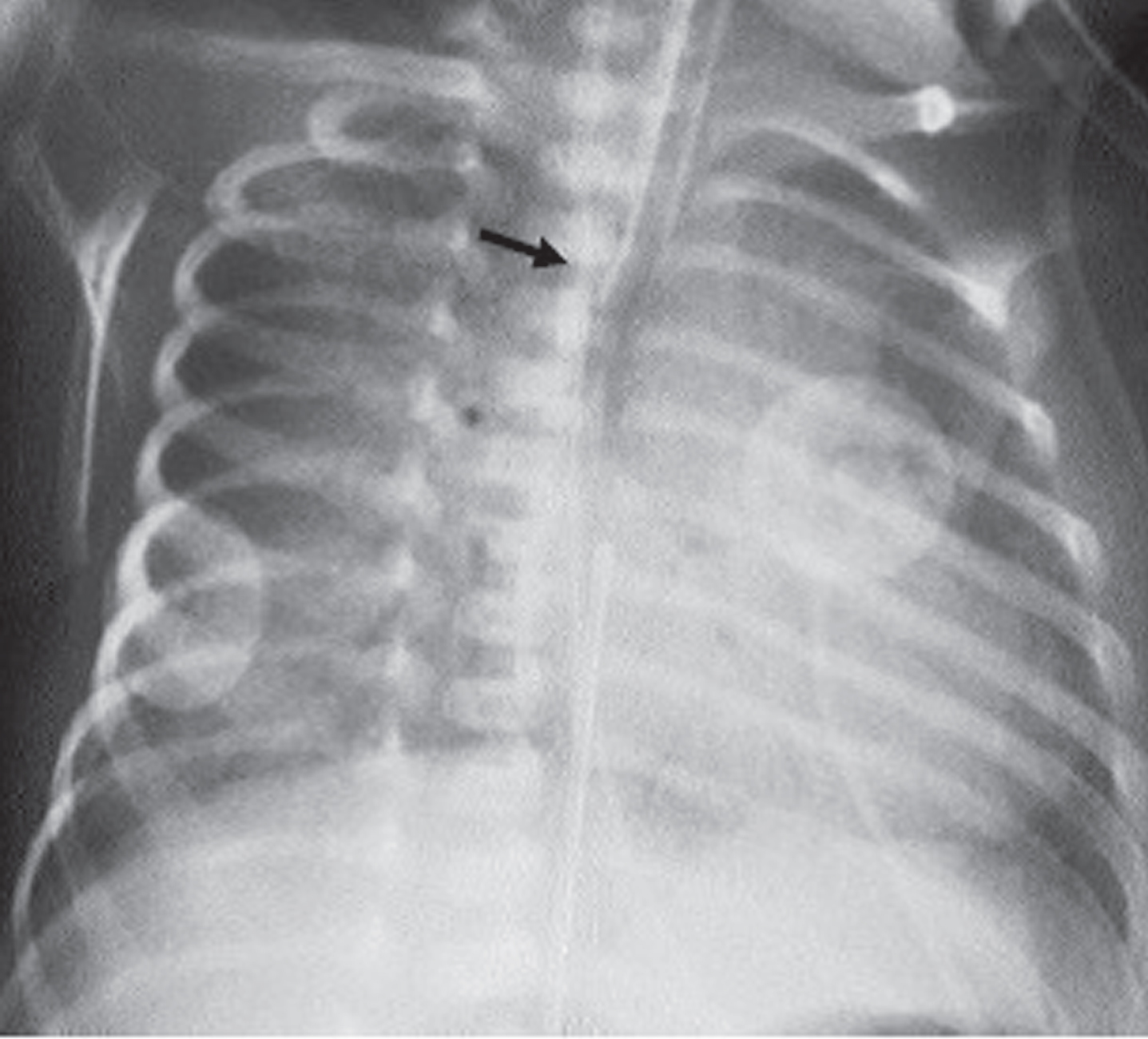
PICC tip at the junction of SVC and right atrium (Black arrow).
On fifteenth day of life, the patient became hemodynamically unstable with hypotension requiring fluid resuscitation and vasopressors associated with increasing respiratory distress and apneic episodes requiring intubation. There was no fever or hypothermia during the course of this acute illness. On physical examination, the baby was lethargic, and hypotonic with abdominal distension and absent bowel sounds. Sepsis work up revealed bands of 17% , thrombocytopenia with platelets of 119,000/ml, elevated CRP of 13.6 as well as elevation of liver enzymes as compared to most recent previous values (Table 1). Initial abdominal x-ray showed distended loops of bowel without free air in abdomen or pneumatosis. A clinical diagnosis of sepsis and/or necrotizing enterocolitis was made. Conservative management with antibiotics, fluids, nil per os, and evaluation by serial abdominal x-ray was started. Twelve hour follow-up abdominal x-ray revealed area of hyperlucency over the liver, suspicious for free air. Pediatric surgery team agreed with the possibility of free air and placed an intraperitoneal Penrose drain. During drain placement 200 ml of thick milky fluid consistent with TPN was drained from the peritoneum and was send for analysis. It had glucose concentration of 850 mg/dl, cholesterol concentration of 65 mg/dl, triglyceride concentration of 170 mg/dl, and LDH concentration of 53 units/liter. The TPN patient was receiving at the time was composed of Dextrose 18gm/kg with GIR 12.5 mg/kg/min, protein 4gm/kg, lipid 3gm/kg along with electrolytes. TPN infusion rate was 5.2 ml/hr and lipid at 0.6 ml/hr providing 140 ml/kg/day of total fluid.
Pertinent laboratory investigations before and after patient’s clinical deterioration
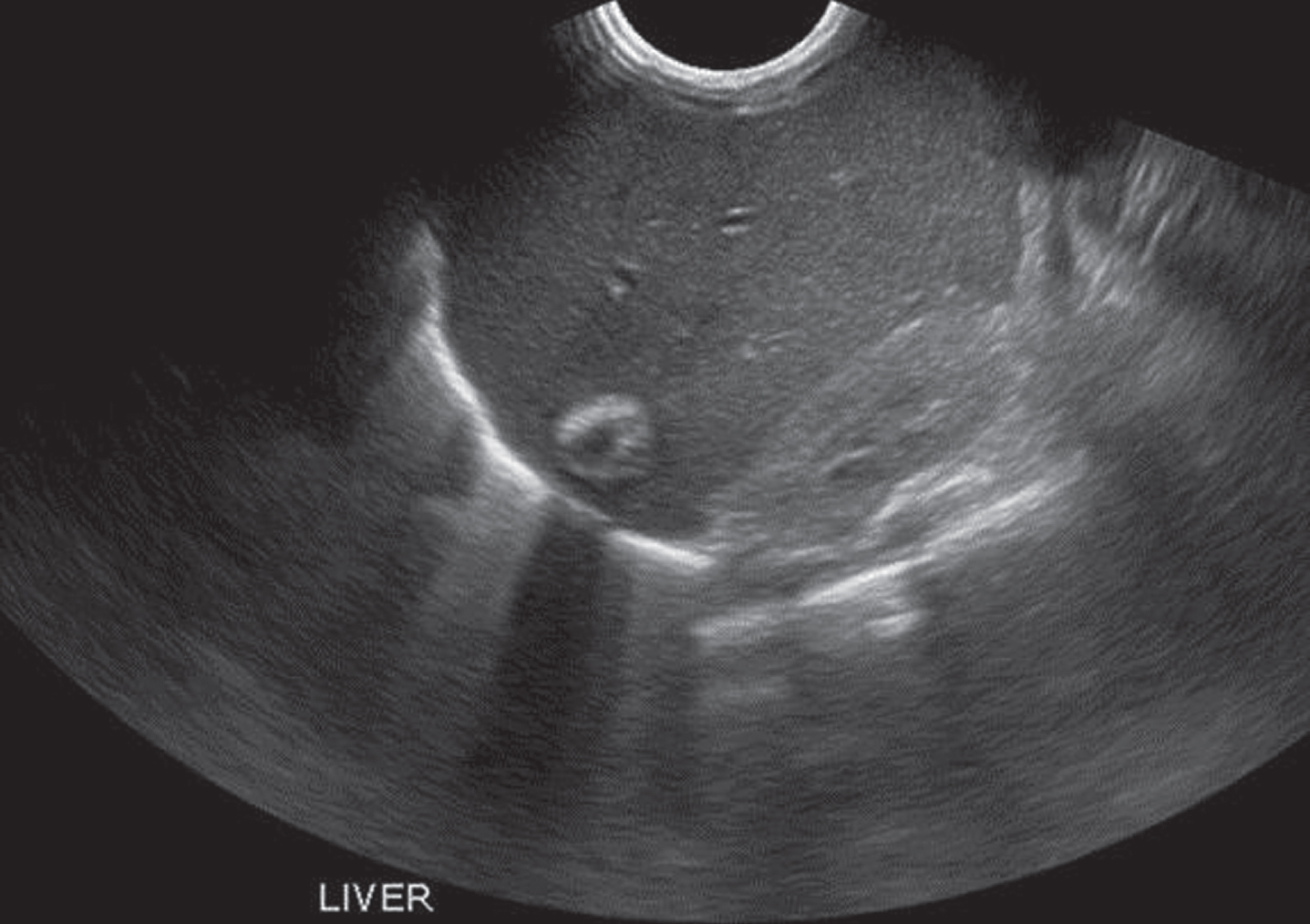
There was interval improvement of abdominal distention after drain placement. Patient’s platelet count further decreased to 57,000/ml and platelet transfusion was given along with fresh frozen plasma. Further review of the x-rays with the pediatric radiologist showed the PICC tip to be in the IVC overlying the hepatic shadow (Fig. 2). Ultrasound of abdomen reported a right hepatic cyst measuring about 3 cm×3 cm×4 cm (Fig. 3). PICC was removed TPN infusion was stopped. The hepatic cyst was drained by an interventional radiologist under ultrasound guided aspiration. Twenty ml of brownish fluid was drained and sent for analysis and culture. The initial blood culture drawn when the baby got sick, the peritoneal fluid, and the fluid culture from the cyst grew Staphylococcus epidermidis.

Catheter tip migration into the IVC and the hepatic vein (black arrow). The white arrow shows the hyper lucent cavity over hepatic shadow mimicking free air.
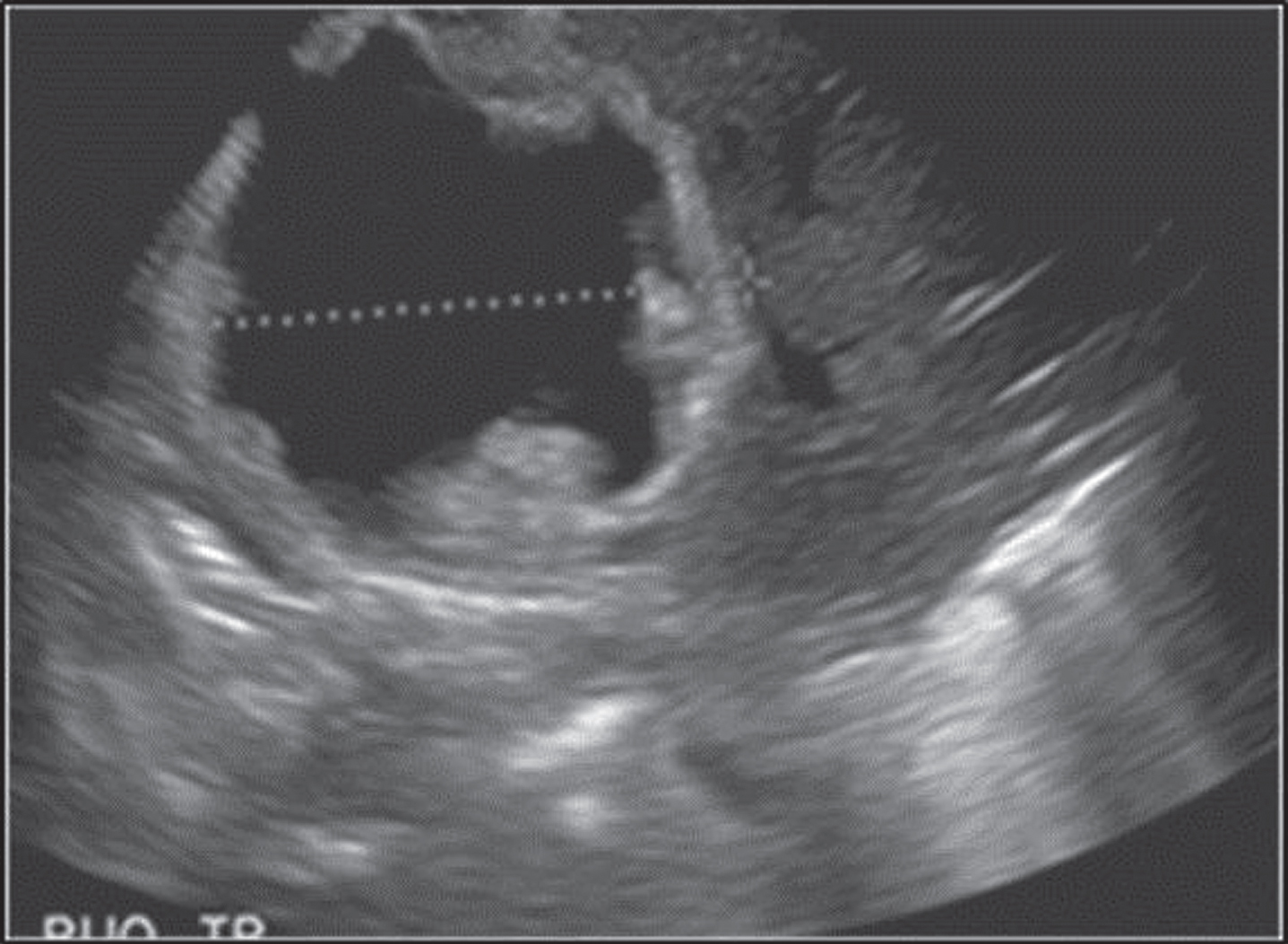
Right hepatic cyst measuring 3 cm×3 cm×4 cm on the first ultrasound.
Baby was managed with IV antibiotics over a total course of four weeks. Repeat aspiration of cyst was done with complete resolution of cyst after about 3 weeks, and normalization of hepatic enzymes upon discharge. Another PICC was inserted at the left upper extremity for further nutrition care after repeat blood culture was negative. Repeat liver ultrasound before discharge showed newly developed calcification at the previously site of cystic cavity within right hepatic lobe (Fig. 4). A clinical diagnosis of migration of PICC into hepatic vein from the inferior vena cava resulting in parenteral fluid extravasation into the liver parenchyma leading to liver abscess and into the peritoneal cavity.
Resolution of the right hepatic cyst with leftover calcifications before discharge.
We report a case of migration of PICC inserted from upper extremity causing extravasation of TPN in the liver parenchyma leading to formation of hepatic abscess and fluid in the peritoneal cavity. Appropriate initial PICC placement does not ensure that the catheter will stay in place as migration of catheter is one of the complications associated with PICC. This can be associated with flow of blood which can cause both the distal migration of a previously optimally placed central catheter as well as spontaneous correction of the malposition catheters [4]. Other caused that may cause PICC migration include straightening of previously coiled catheter, poor catheter fixation at skin surface, or movements at the joints. Arm movements have been shown to have a significant effect on the position of the tip of PICC with variation of up to two centimeter [5]. Catheters placed in the basilic or cephalic veins below the level of elbow are likely to move towards the heart when the elbow is flexed or the arm is adducted with an additive effect with both flexion and adduction [6].
Cases of TPN extravasation into the peritoneum have been described in the past by different authors. Meeks et al., had described the intrahepatic extravasation of parenteral nutrition fluid likely related to from arterial placement of PICC [7]. Two cases of abdominal extravasation from inferior vena cava placed PICC mimicking necrotizing enterocolitis have been reported [8]. In most of these cases the extravasation occurred from lower extremity inserted central lines migrating into abnormal vasculature.
In our case, we postulate that the tip of the catheter migrated from the SVC or right atrium into the IVC, and then into one of the hepatic veins leading to extravasation of hyperalimentation into the liver leading to formation of hepatic abscess and ascites. However, it is difficult to postulate when the PICC tip migrated since the baby was clinically stable and receiving fluid and medications through the line over ten days without any symptoms. Since the peritoneal membrane has good absorptive characteristics and as the rate of fluid administration through the PICC was low, our patient did not present with symptoms earlier. Slow extravascular infusion of fluid in the low resistance extra-peritoneal space may not be promptly detected in the absence of a high index of suspicion. This complication was noted in our patient on investigation done as part of septic work up once the baby became sick. Further, the extravasation of TPN into the liver parenchyma and peritoneal cavity led to formation of a hepatic cyst and subsequently abscess infected with Staphylococcus epidermidis associated with septicaemia. Staphylococcus epidermidis is an opportunistic pathogen and can proliferate in indwelling medical devices like intra venous catheters and cause bacterial sepsis in vulnerable patients [9]. Bansal et al., described PICC migration and extravasation of fluid in association with S. epidermidis sepsis. The authors postulated local S. epidermidis phlebitis as a cause for catheter displacement and resultant extraluminal migration [10]. S. epidermidis identified in the blood, peritoneal, and cystic fluid of our patient indicates that this infection may have played a role in our patient.
Proper positioning of PICC tip is routinely confirmed after initial placement with an x-ray and adjustments are done thereafter as indicated. After initial confirmation, line position is assessed on subsequent films often required for other diagnostic purpose. However, routine use of imaging to only evaluate PICC position in asymptomatic patients has not been a standard practice given the concern associated with excessive radiation exposure in this population. At our institution, we do evaluation of PICCs, mainly insertion site and external parts of the PICC as well as dressing change in accordance with New York State Regional Perinatal Care Centers PICC bundle [11].
Awareness, high index of suspicion and early recognition of this complication is essential to prevent delay in the diagnoses and also avoid the need for major surgical interventions and associated poor outcomes. Monitoring for migration of PICCs by tracking length of external catheter, evaluating insertion site for any tension or kinking and, assuring integrity of dressing is crucial in early detection of such complication [12]. High index of suspicion coupled with imaging obtained promptly in any symptomatic patients or any patient where catheter tip migration is suspected will likely prevent such potentially fatal complication.
Disclosure statements
The authors have no conflict of interest related to the manuscript.