
Abstract
Kasabach-Merritt syndrome is a rare life-threatening clinical presentation in neonatal period. it is characterized by giant hemangioma and serious thrombocytopenia. The diagnostic criteria include: 1) hemangiomas on skin, 2) thrombocytopenia or coagulopathy, 3) hemangioma on internal organs diagnosed by ultrasonography, computed tomography or magnetic resonance imaging, and 4) excluding reasons, such as idiopathic thrombocytopenic purpura or hypersplenism.
Placental chorioangiomas are the most widespread non-trophoblastic benign tumor-like lesions of placenta. The clinical signs are associated with tumor size. Chorioangiomas larger than 4-5 cm may lead to various maternal and fetal complications.
Here, a female premature infant was diagnosed with placental chorioangioma and liver hemangioma during antenatal period. She developed heart failure secondary to non-immune hydrops fetalis in the neonatal period. The atypical giant hemangioma and coagulopathy suggested the diagnosis of Kasabach-Merritt syndrome. The macroscopic and histopathological examination of the placenta confirmed the diagnosis of chorioangioma. The patient died due to purpura fulminans despite the treatment with prednisolone and propranolol that was started on the second day of life. We are presenting this rare case where placental chorioangioma leading to non-immune hydrops fetalis co-existed with Kasabach-Merritt syndrome.
Keywords
Introduction
Kasabach Merritt Syndrome (KMS) is characterized by the combination of rapidly growing vascular tumor, thrombocytopenia, microangiopathic hemolytic anemia and consumptive coagulopathy [1]. The diagnostic criteria include hemangiomas on skin or internal organs, thrombocytopenia or coagulopathy, hemangioma supported by such monitoring methods as ultrasonography, computed tomography or magnetic resonance imaging, and excluding reasons, such as idiopathic thrombocytopenic purpura or hypersplenism.
Placental chorioangiomas more than the size of 4-5 cm may lead to various maternal, fetal and neonatal complication like non-immune hydrops, microangiopathic hemolytic anemia, thrombocytopenia and cardiac failure. The mortality rate is high [2]. In our case, the atypical giant hemangioma in liver and coagulopathy suggested the diagnosis of KMS in postnatal period. Because of the rarity in literature related to the co-existence of placental chorioangioma leading to non-immune hydrops fetalis and KMS developing due to giant liver hemangioma in antenatal period, our case was presented.
Case
A female infant born to a 23-year-old mother at 32 weeks of gestation through cesarean section. The infant was diagnosed with non-immune hydrops fetalis and was intubated immediately after delivery. The patient was diagnosed with hemangioma in the liver. The placenta had chorioangioma. Birth weight was 1915 g (10–25% percentile), length was 43 cm (25% percentile), and head circumference was 31 cm (25–50% percentile). Apgar scores were 4 at the 1st and 5 at the 5th minutes. Physical examination revealed widespread subcutaneous edema. On abdominal examination, liver and spleen were palpable 6 cm and 3 cm below the coastal margin, respectively. Because the echocardiography demonstrated the findings of heart failure and pericardial effusion in the patient receiving mechanic ventilation, dopamine (10 mcg/kg/min) was started for inotropic support. On the ultrasonography (USG) of lungs, minimal fluid was determined in pleura.
White blood cell count was 8600/mm3, hemoglobin was 9.5 g/dL, hematocrit was 27.3% (36–55%), and platelet count was 63000/mm3 (range 175,000–500,000/mm3). Biochemical markers were determined as follows: serum aspartate aminotransferase (AST) was 3559 U/L, serum alanine aminotransferase (ALT) was 483 U/L, albumin was 2 g/dL, d-dimer concentration was >20μg/ml (normal range <1μg/ml), prothrombin time (PT) was 46 sec (11–15 sec), international normalized ratio (INR) was 5 sec (range 1–1.5 sec), activated partial thromboplastin time (aPTT) was 115 sec (range 40–72 sec), thrombin time was 47 sec (14–21 sec) and fibrinogen was 30 mg/dL (range 200–400 mg/dL). Apheresis thrombocyte suspension and fresh frozen plasma were started to be given to the patient as supportive treatment. On peripheral smear test, schistocytes consistent with microangiopathic hemolytic anemia and fragmented erythrocytes were observed (Fig. 1). No thrombocytopenia was detected in maternal blood count. On abdominal USG, hemangioma with irregular margins, developing in hypo and isoechoic areas and in size of 2.5×3.5 cm was determined in the right lobe of liver. No operation or embolization was performed due to coagulopathy, and pediatric hematology and pediatric oncology departments were consulted.

The presence of schistocytes and fragmented erythrocytes on a peripheral blood smear test.
With the thought of KMS, a treatment modality, including pulse-steroid at the doses of 30 mg/kg for the first 3-day followed by 20 mg/kg/day for 3-days, 10 mg/kg/day for 3 days period and 2 mg/kg/day for a total of 1 month. Propranolol (2 mg/kg/day) was also started. On the macroscopic investigation of placenta, while a nearly medium-hard, grayish-white mass (pale-yellowish partly) in size of 4×3.5×3.5 cm was observed, the tumor was seen to be composed of vascular endothelial cells in the histopathological examination (Fig. 2). Immune histochemically showed tumor cells in cluster domain (CD) 34, cytokeratin (CK) 18 and smooth muscle actin (SMA) positive (Fig. 3). Despite supportive therapeutic efforts, the patient had widespread ecchymosis due to disseminated intravascular coagulopathy (DIC) died on the 9th day of life (Fig. 4).

A medium-hard, grayish-white mass of 4×3.5×3.5 cm, with some pale-yellowish parts was seen in the histopathological examination.
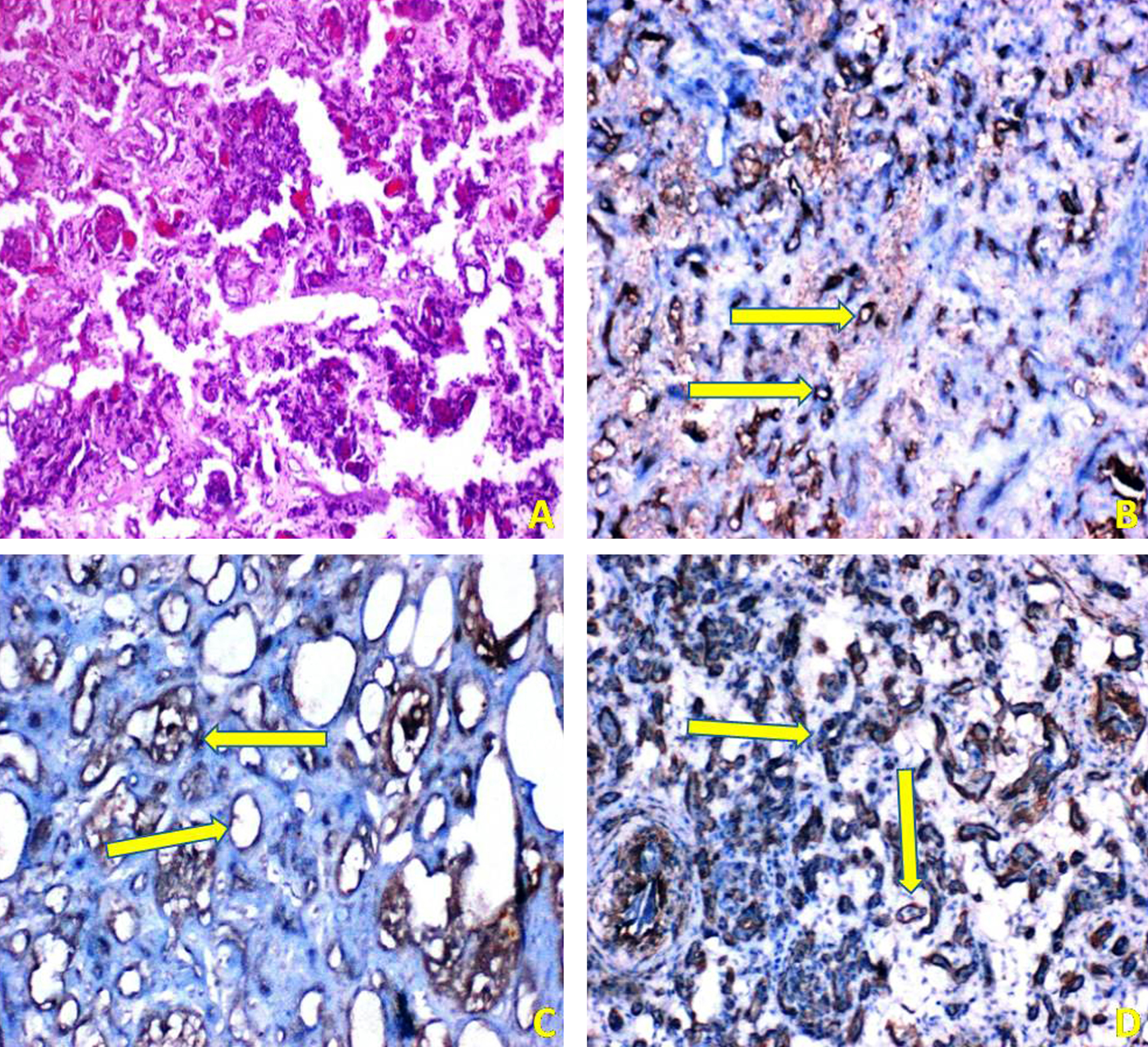
An immunohistochemical study, a) cells with hematoxylin Eosin stain, b) cluster domain 34 positive cells, c) cytokeratin 18 positive cells, d) smooth muscle actin positive cells (arrows).

Presence of widespread ecchymosis due to disseminated intravascular coagulopathy.
KMS was described by Kasabach and Merritt in 1940 [3]. While 80% of cases are diagnosed within the first year of life. Mortality rate ranges between 10 to 37% . The treatment of KMS is a challenge. The primary signs of KMS are the presence of giant hemangioma and lower thrombocyte count. KMS develops among 1% of the cases with hemangioma [4]. While giant cutaneous hemangiomas are easy to be detected on physical examination, the determination of visceral hemangiomas may be overlooked. The risk of hemorrhage due to hemangioma, and coagulopathy are present during the neonatal period. Mortality is higher especially in the cases commencing within the intrauterine period for leading to premature births. These patients typically have prolonged PTand aPTT, decreased fibrinogen concentration and increased d-dimer level. It is essential to screen for hemangiomas via imaging techniques.
The mechanism of KMS is related to the thrombocyte activation due to the abnormal proliferation of endothelium inside the hemangioma, the microthrombi formed by thrombocytes with fibrin and the consumption coagulopathy arising from the reduction of coagulation factors due to consumption. In our case, there was a decompensated DIC with thrombocytopenia, prolonged PT, aPTT, thrombin time, low fibrinogen, and increased d dimer level.
Optimal treatment remains unclear. Although various treatment regimens including steroids, chemotherapeutics such as vincristine, adriamycin and cyclophosphamide, vascular embolization, propranolol, interferon, radiotherapy and surgery have been experimented, no effective therapeutic modality has been suggested yet [5]. Because of prolonged time in achieving responses to the treatment with a single agent, combined treatment modalities are chosen. Corticosteroids are the first step regime in the treatment of KMS. The effects are seen in nearly two weeks, and 30–50% of all patients respond to the treatment [6]. As a matter of fact, pulse steroid treatment started in our patient early, however it was not effective in preventing disseminated intravascular coagulopathy induced by the tumor. Propranolol is a non-selective beta blocker that can enable the inoculation of hemangiomas and has frequently been used in the treatment of benign infantile hemangiomas particularly in recent years. In literature, there are cases reporting that tumoral structures have been shrunk due to the use of steroids, vincristine and propranolol in the treatment of kaposiform hemangioendothelioma showing frequent co-existence with KMS [7]. The most significant treatment modality of KMS or multiple liver hemangiomas is the resection of tumors surgically. As with our patient, however, it is unlikely to remove the tumor during a state of coagulopathy.
Placental chorioangiomas are the commonest non-trophoblastic benign tumor-like lesions of placenta. Especially the tumors over 4 cm can be detected with routine obstetric USG, while tiny chorioanginomas are generally determined incidentally. The incidence is more common in females than male infants. Premature births due to arteriovenous shunts in placenta, and complications such as fetal anemia, intrauterine growth restriction, polyhydramnios, non-immune hydrops fetalis and heart failure may be associated with placental chorioangiomas [8]. When compared to multiple pregnancies, smaller chorioangiomas are encountered in single pregnancies and with preeclampsia. Therefore, the risk of placental hypoxia increases in the presence of chorioangiomas [9]. Although a single pregnancy was present in our case, the presence of giant chorioangioma is a rare condition. The diagnosis of placental chorioangiomas should be supported with the pathological investigation of placenta in postnatal period. Heart failure due to giant chorioangioma in our patient developed in intrauterine period and presented with non-immune hydrops fetalis. We consider that placental chorioangioma accompanied by KMS with a higher mortality even when developing as a single disorder contributed to the progressive course of the disease. In literature, as in our patient, another case of coagulopathy accompanied by a giant placental chorioangioma in a neonate was reported [10]. However, this current case is different because of the presence of liver hemangioma. To the best of our knowledge, such a coexistence has not been reported yet.
In conclusion, KMS and non-immune hydrops fetalis are conditions with fatal potential in neonatal period. In these cases, there are treatment difficulties. Multidisciplinary approach is very important for successful management of complications associated with these clinical conditions.