
Abstract
BACKGROUND:
Study aims to evaluate whether vancomycin dosing from published dosing algorithms correlate with the attainment of target troughs of 10 to 20 mg/L.
METHODS:
NICU patients who received minimum three doses of vancomycin and had a trough level met inclusion criteria. Dosing information was retrospectively evaluated to determine which published dosing regimen was followed. Dosing algorithms used were matched to NeoFax/Harriet Lane, renal-function directed dosing, and weight-directed dosing, in which the latter two can be found in Pediatric and Neonatal Lexi-Drugs. Primary outcome was percentage of troughs within therapeutic (10 to 20 mg/L) and subtherapeutic (less than 10 mg/L) levels.
RESULTS:
Of 97 troughs evaluated, NeoFax/Harriet Lane accounted for 86.6%, renal-function directed accounted for 5.1%, and weight-directed dosing accounted for 18.5% of dosing algorithms. NeoFax/Harriet Lane, renal-function directed, and weight-directed dosing attained therapeutic levels between 10 to 20 mg/L at a rate of 60.7%, 60%, and 50% of the time, respectively. With respect to initiation of therapy, a higher dose of 15 mg/kg versus 10 mg/kg attained therapeutic levels (p < 0.001; OR 11.22; 95% CI, 3.96 to 31.81), while a serum creatinine value below 0.5 mg/dL attained subtherapeutic levels (p = 0.028; OR 0.068; 95% CI, 0.006 to 0.74).
CONCLUSIONS:
NeoFax, Harriet Lane, and renal-directed dosing from Pediatric and Neonatal Lexi-Drugs achieved target troughs within the 10 to 20 mg/L range more often than weight-directed dosing from Pediatric and Neonatal Lexi-Drugs. Initiating therapy at a higher dose and patient serum creatinine value above 0.5 mg/dL were factors significantly associated with a 10 to 20 mg/L range.
Keywords
Introduction
Vancomycin is one of the commonly used antibiotics in the neonatal population as part of an empiric regimen for suspected sepsis or as targeted treatment for a documented infection. There is variability within the neonatal population between term and preterm neonates in various pharmacokinetic parameters that affect vancomycin dosing, such as volume of distribution and glomerular filtration rate [1–4]. Furthermore, in view of the increase in the mean inhibitory concentration (MIC) of Methicillin resistant Staphylococcus aureus (MRSA) isolates, there is concern that current dosing algorithms will lead to suboptimal vancomycin exposure and potential treatment failure, predicted by low area-under-the-concentration-time-curve (AUC) for a 24 hour time period to MIC ratios (AUC24/MIC) in the neonatal and general pediatric population [1, 6]. Dosing information from current product labeling is generalized and suggests longer dosing intervals in preterm neonates, however does not provide specific recommendations of how to adjust [6]. Published references, such as NeoFax, Harriet Lane, Pediatric and Neonatal Lexi-Drugs recommend neonatal dosing regimens according to various combinations of postmenstrual age (PMA), postnatal age (PNA), gestational age, and serum creatinine in order to recommend a weight-based milligram per kilogram (mg/kg) dose and a corresponding dosing interval [6–10].
Trough levels are recommended to monitor for potential toxicity and adverse effects, and also as a surrogate marker for pharmacokinetic efficacy for specific medications such as vancomycin. It is recommended to obtain a trough at steady state, which is 30 minutes prior to the fourth dose of vancomycin, and repeated as clinically necessary [7]. Maintaining drug levels within the published target therapeutic range is paramount in achieving its desired antimicrobial efficacy and simultaneously minimizing the risk of the development of bacterial resistance in the neonatal intensive care unit (NICU) and the occurrence of potential side effects, such as nephrotoxicity and ototoxicity. Current therapeutic drug level monitoring recommendations have been extrapolated from the adult population, which target a trough level of 10 to 15 mg/L for most infections, and a higher trough of 15 to 20 mg/L for more severe infections, including MRSA bacteremia, infective endocarditis, osteomyelitis, meningitis, pneumonia, complicated skin and soft-tissue infections, and bone and joint infections [11]. Among coagulase-negative Staphylococcus aureus (CoNS) which is considered pathogenic in the neonatal population, the target trough range has been increased from 5 to 10 mg/L to 10 to 15 mg/L, reflecting increased resistance [12].
Current editions of NeoFax and Harriet Lane (20th edition) have identical dosing and recommend a dosing interval on the basis of PMA and PNA, and a weight-based dosage based on the type of infection being treated. Both references recommend 10 mg/kg/dose for bacteremia and 15 mg/kg/dose for meningitis and pneumonia, with the target trough of 15 to 20 mg/L for meningitis, pneumonia, and MRSA bacteremia [7, 8]. Pediatric and Neonatal Lexi-Drugs provide neonatal dosing algorithms that are renal-function directed (Bradley 2016, Capparelli 2001, Red Book [AAP 2015]) or weight-directed (Red Book [AAP 2009]) [9, 10]. The renal-function based dosing recommends a mg/kg dosage and corresponding dosing interval on the basis of different serum creatinine levels for neonates of gestational age >28 weeks and≤28 weeks [9, 10]. Weight-directed dosing takes into account body weight and PNA.
Prospective and retrospective studies have been conducted in order to propose or evaluate the use of different dosing regimens, using the percentage of treated neonates with goal therapeutic troughs, goal therapeutic peaks, and result of initial and follow-up hearing tests as primary and secondary outcomes, respectively [12–16]. The aim of this study was to evaluate dosing regimens that were utilized in a sample of treated neonates to determine the potential association between dosing regimen utilization and therapeutic trough level attainment.
Methods
The retrospective study was conducted in the level III NICU at NewYork-Presbyterian Brooklyn Methodist Hospital. The research population consisted of any patient admitted to the NICU from January 1, 2012 to December 31, 2014 who received at least three doses of vancomycin and had an initial appropriately drawn trough level. Vancomycin levels were excluded from evaluation if obtained greater than one hour prior to administration of the next scheduled dose of vancomycin or if taken earlier than one hour immediately prior to the third dose or later. The PNA and PMA of the neonates were noted, as well as the mg/kg dosage and dosing interval that were utilized to determine which published dosing regimen they followed. Of note, the dosing that was utilized for a given trough may follow more than one published dosing regimen due to the overlap of ranges provided by different algorithms. Institutional review board approval was granted.
The primary outcome was the proportion of first trough levels within the target therapeutic range of 10 to 20 mg/L, as well as within the specific component 10 to 15 mg/L and 15 to 20 mg/L therapeutic ranges, and subtherapeutic range of less than 10 mg/L. The secondary outcomes were the achievement of troughs within the therapeutic range based on different prescribing variables including gestational age, PNA, PMA, dosing weight, serum creatinine, and dosing regimens.
Statistical analysis
Descriptive statistics were calculated for study variables. Categorical variables were reported in numbers and percentages. The continuous variables were reported as mean and standard deviation. Group differences were examined using Chi-square test or Fisher’s exact test for categorical variables, and Student’s t-test for continuous variables. A logistic regression model was designed in order to estimate the factors most likely to impact vancomycin trough attainment. Statistical analysis was performed using SPSS 21.0 (IBM SPSS statistics, New York, USA); p-value < 0.05 was considered significant.
Result
Eighty-eight neonates were screened, of which 74 met inclusion criteria, and a total of 97 vancomycin initial troughs were evaluated (Fig. 1). Table 1 summarizes commonly used published vancomycin dosing references. The demographics utilized for comparison included gender, birth weight, dosing weight, GA, PNA, PMA, serum creatinine, indications for treatment, therapy, and dosing and monitoring. Using the Chi-square test or student’s t-test, male gender, birth weight, dosing weight, GA, PMA, serum creatinine, listed indications for treatment, therapy, treatment duration, number of doses, concomitant use of gentamicin therapy, and early trough obtained before third dose were not statistically significant; however, PNA at dosing and trough values were statistically significant (p < 0.05), as shown in Table 2. From these, 86.6% were dosed in accordance to NeoFax (2015) and Harriet Lane (20th Edition), 18.5% in accordance to weight-directed dosing, and 5.1% in accordance to the renal function-directed dosing regimen (Table 3).
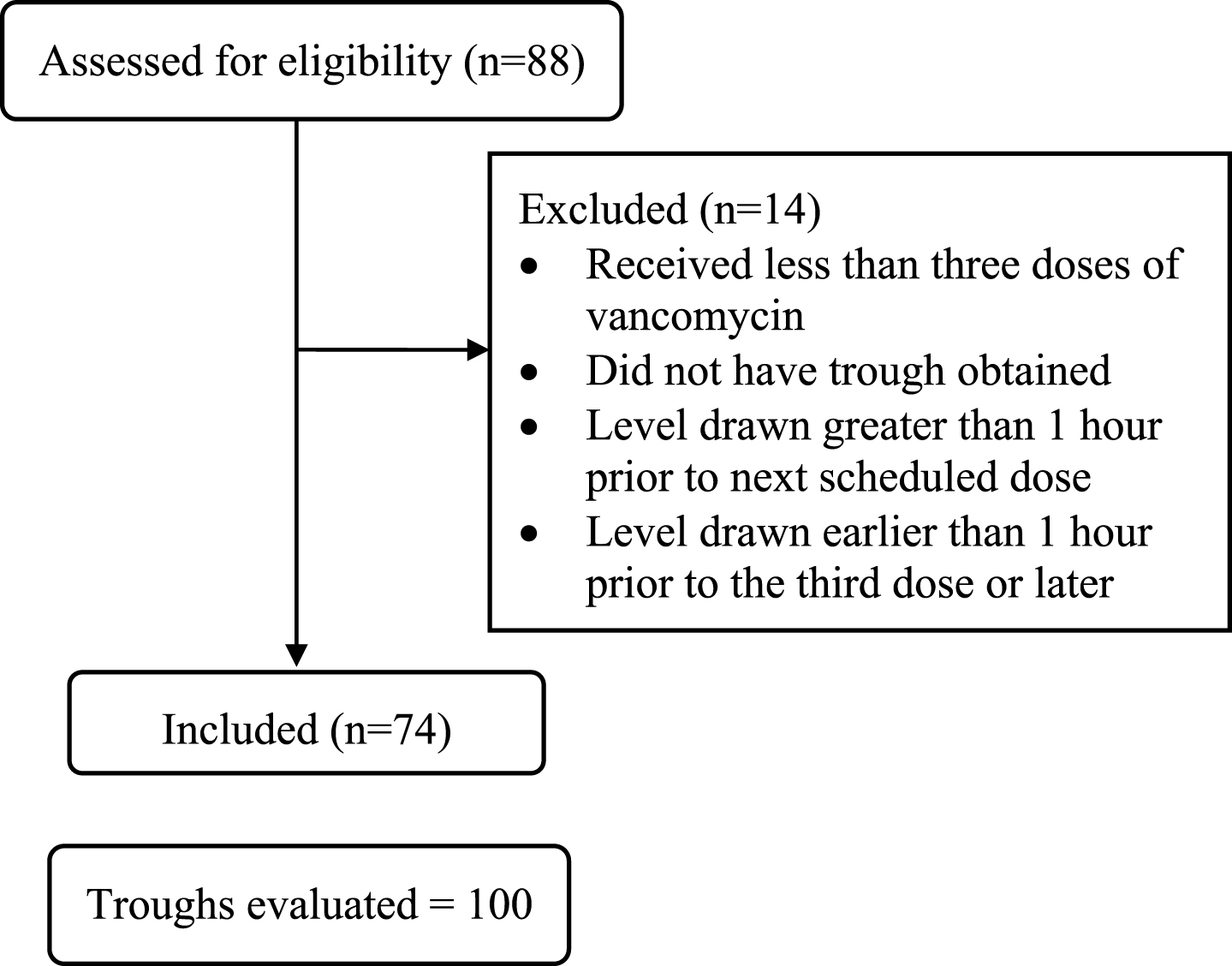
Patient selection.
Reference vancomycin dosing algorithms
Patient demographics
Data expressed as n (%), unless otherwise specified. *Mean±SD. NS, non significant.
Trough attainment by different utilized published dosing algorithms
Note: There were a total of 97 troughs evaluated; however, dosing regimens may overlap between references. Data expressed as n (%), unless otherwise specified. NS, non significant.
Among the 84 troughs dosed in accordance to NeoFax and Harriet Lane, 39.3% were less than 10 mg/L and 60.7% were within the 10 to 20 mg/L target range. Within the therapeutic range based on NeoFax/Harriet Lane dosing, 69.7% of troughs were 10 to 15 mg/L and 30.3% were 15 to 20 mg/L. Among the five troughs that were attained based on renal-functional directed dosing, 40% were less than 10 mg/L and 60% were within the 10 to 20 mg/L range, with 100% in the 10 to 15 mg/L range. Trough attainment with weight-directed dosing showed that 50% were less than 10 mg/L and 50% were within the 10 to 20 mg/L range. Within the therapeutic range of troughs dosed based on weight-directed dosing, 88.9% were in the 10 to 15 mg/L range and 11.1% were in the 15 to 20 mg/L range (Table 3). Using the Chi square test, there were no statistical differences in trough attainment between the dosing references.
Patient factors or dosing regimens in relation to trough attainment were analyzed as secondary endpoints (Table 4). Of all examined variables, only vancomycin dose and serum creatinine value were significant factors that affected trough attainment. Using a higher dose of 15 mg/kg as compared to 10 mg/kg, regardless of dosing intervals, resulted in therapeutic trough attainment in 74.1% of cases and yielded significant target trough attainment of 10 to 20 mg/L (X2 25, p < 0.0001, odds ratio [OR] 11.22, 95% confidence interval [CI], 3.96 to 31.81) compared to only 14% of cases who received lower vancomycin dosing of 10 mg/kg (OR 0.088; 95% CI, 0.03 to 0.25) (Table 4). There was no statistical difference between the two dosing regimens and attaining low and high therapeutic troughs of 10 to 15 mg/L and 15 to 20 mg/L, respectively. Serum creatinine level also affected vancomycin trough attainment (X2 16.4, p < 0.001) (Table 4). Serum creatinine values less than 0.5 mg/dL were associated with a subtherapeutic trough (p = 0.028; OR 0.068; 95% CI, 0.006 to 0.74) whereas higher values of serum creatinine were not significantly associated with low trough attainment.
Trough attainment based on different variables
Data expressed as n (%), unless otherwise specified. *Chi2 value computed based on count percentage within dose category.
Among troughs evaluated, there was a similar proportion of troughs within the target range of 10 to 20 mg/L across the different dosing algorithms assessed, with a very low occurrence of trough levels within the higher 15 to 20 mg/L end of the target range that is currently advocated for more severe infections. The majority of troughs evaluated were subtherapeutic. With respect to different patient variables in target trough attainment, dosing vancomycin therapy with 15 mg/kg/dose allowed more levels to reach the 10 to 20 mg/L range as compared to 10 mg/kg. In addition, patients with serum creatinine values upon vancomycin initiation less than 0.5 mg/dL seemed to be significantly associated with levels less than 10 mg/L, whereas patients with higher serum creatinine values did not significantly attain subtherapeutic troughs.
The occurrence of a greater proportion of troughs within the target range when the higher recommended weight-based dosage was employed is an interesting finding. Published dosing regimens recommend the higher 15 mg/kg/dose dosing for meningitis and pneumonia and lower 10 mg/kg/dose dosing for bacteremia and other infections at a dosing interval determined by PMA and PNA. However, a higher target trough range of 15 to 20 mg/L is currently recommended for meningitis, pneumonia, as well as MRSA bacteremia and other serious infections in the adult population. Currently there are no data to correlate the adult trough range of 15 to 20 mg/L with an AUC/MIC ratio greater than 400 in the neonatal population. However, in this study, the higher trough range was seldom achieved when dosed at 10 mg/kg/dose. In clinical practice, the selection of an initial weight-based dosage on the basis of the type of infection suspected may lead practitioners to dose on the lower end of the dose range, leading to a higher likelihood of a subtherapeutic initial trough. This scenario becomes clinically relevant in neonates who are being empirically treated and are subsequently found to have a true infection, thus making appropriate initial dosing paramount.
It is also important to note that there was a very low incidence of vancomycin troughs in the supratherapeutic range above 20 mg/L. Of the 84 troughs that were dosed in accordance to NeoFax and Harriet Lane, only 3 troughs were in the supratherapeutic range (mean 23.4±3.3 mg/L). A post-hoc analysis of these supratherapeutic levels revealed that two of the three elevated troughs occurred in neonates with multi-organ failure requiring vasopressor and inotropic support, and in a third neonate receiving concurrent acyclovir, a known nephrotoxic agent (Table 5).
Characteristics of patients with supratherapeutic trough (n = 3)
This retrospective study had several limitations. As a retrospective study, only possible associations could be made. Levels measured immediately prior to the third or later dose were accepted as trough levels. However, due to variability in the pharmacokinetic parameters between term and preterm neonates, levels taken prior to immediately before the third dose may not have been taken at steady state, and thus may be somewhat lower than expected than if taken prior to a subsequent dose instead. Additionally, there was no suitable adequate comparator to perform statistical analysis in order to determine if following a specific published dosing regimen over another produced a greater proportion of target therapeutic troughs, as there were a disproportionate number of troughs dosed in accordance to one published dosing regimen over another. Finally, this study did not assess trough attainment with clinical outcomes such as clinical improvement or the occurrence of adverse outcomes.
The findings from this retrospective study echo the finding of other dose algorithm evaluation studies that purport current published dosing regimens for the use of vancomycin may not achieve target trough levels in a reliably high proportion of treated neonates [12–16]. Higher vancomycin dosage of 15 mg/kg and a serum creatinine greater than 0.5 mg/dL are factors more likely to achieve a therapeutic trough level in 10 to 20 mg/L range. Further investigation is warranted to determine the optimal dosing of vancomycin in the neonatal population.
Disclosure statement
The authors declare no conflict of interest.
Footnotes
Acknowledgments
No academic, charitable, or commercial acknowledgements to report.