
Abstract
BACKGROUND:
To describe amplitude-integrated encephalogram (aEEG) characteristics of neonates with neonatal abstinence syndrome (NAS).
METHODS:
This is a prospective observational study. Newborns exposed to prenatal opioids and their gestational matched controls were included. A single-channel aEEG was obtained using Olympic 6000 CFM monitor. The background activity (continuous/discontinuous), the amplitudes (μV) and the presence of sleep-wake cycle (SWC) were documented.
RESULTS:
A total of 59 infants, 23 with NAS and 36 controls were enrolled. All aEEG were completed within 48 hours of life prior to initiation of treatment. Birth weight and gestational age were similar in both groups. An aEEG was abnormal (discontinuous pattern and/or absent SWC) in 78 % (18/23) of infants with NAS versus only 25% in control group (9/36), [OR 10.8, CI (2.7–46.5) P < 0.001]. 61% of infants with NAS had discontinuous pattern [OR 7.8, CI (2–32) P = 0.001] and 39% had absence of sleep-wake cycle [OR 7.1, CI (1.4–39.4) P = 0.007].
CONCLUSIONS:
A majority of infants with NAS have abnormal aEEG activity.
Abbreviations
amplitude-integrated electroencephalogram;
neonatal intensive care unit;
neonatal abstinence syndrome;
length of stay;
sleep-wake cycle
Introduction
Maternal use/abuse of substances i.e. opioids, benzodiazepines, barbiturates, during pregnancy can lead to neonatal abstinence syndrome (NAS), which is described as a constellation of physiological symptoms in a newborn with acute withdrawal from opioids after birth [1]. There has been a recent surge in abuse of opioids (illicit or prescription)in The United States, including women during pregnancy, while abuse of Methamphetamines and cocaine have had only a modest increase [2]. The most common treatment modalities for opioid addiction available for pregnant women are long acting synthetic opioid methadone [3] or buprenorphine [4] which is a partial mu-opioid agonist and kappa-opioid antagonist. These medications are also known to cause neonatal abstinence syndrome of variable severity [5]. There are concerns regarding short-term and long-term neuro-developmental effects on newborns exposed to such substances in-utero [6, 7]. With the recent increase in opioid use among the pregnant women and the concurrent increase in infants with neonatal abstinence syndrome, there is an ardent need to identify newborns most at risk of poor development and learning difficulties [8, 9]. There is a need for evaluating the effects of maternal substance abuse on neonatal brain electrical activity.
The modality of an aEEG has proven validity and sensitivity to detect brain activity in both term and preterm newborns [10, 11]. It is simple to apply and can be used for prolonged continuous limited-channel EEG monitoring [12, 13]. Normative aEEG measurements for term and preterm infants have been published [14, 15]. Tracings on an aEEG can reveal abnormal brain activity that otherwise would be unrecognized, such as subclinical seizure activity or transient background alterations [16]. We postulate that an aEEG will detect brain wave abnormalities in opioid exposed infants.
Objective
To assess the aEEG brain wave characteristics in infants with neonatal abstinence syndrome secondary to in-utero opioids exposure.
Methods
This is a single-center prospective observational case-control study conducted from July 2015 through October 2016. Institutional review board approved the project and a certificate of confidentially was obtained.
Study was conducted at Regional One Health hospital neonatal intensive care unit (NICU). This NICU serves as the regional perinatal center with active delivery service. All newborns with prenatal history of opioid exposure are admitted to NICU for observation and or treatment if needed. Infants with maternal history of illicit (i.e. methadone, marijuana, heroin etc.) and or prescription opioids were eligible for study. Maternal urine drug screening, infant’s urine, and umbilical cord drug screening were recorded.
Inclusion Criteria: (a) Study subjects were infants with a maternal history of prescription or illicit opioid use during pregnancy. (b) Control subjects were healthy gestational age-(GA) matched infants without a history of prenatal opioid exposure.
Exclusion Criteria included:(a) Infants with congenital or acquired brain anomalies (brain malformations, any grade intra-ventricular hemorrhage, periventricular leukomalacia or cerebral hemorrhage), perinatal acute hypoxic event, seizure disorders or an acute illness during this admission. (b) Neonates more than 48 hours of life. (c) Neonates who received either opioids and or benzodiazepines prior to study enrollment.
After identifying a potential study or control subject, an informed written consent was obtained from the mother or a legal guardian within 24–36 hours of life.
aEEG procedures
All infants underwent a bedside aEEG recording with Olympic CFM6000 monitor (Natus Medical Inc., San Carlos, CA). Single channel recording was obtained with hydrogel electrodes placed in bi-frontal (FP1 and FP2) positions. Skin preparation was done according to the established procedure. A continuous 4 to 6 hours recording was completed during routine infant care. Application of aEEG electrodes and data recording were performed by research staff trained in appropriate placement of the aEEG leads and aEEG monitor.
Basic aEEG analysis
Interpretation of the aEEG was done by a study neonatologist experienced in interpretation of aEEGs and blinded to the patient’s clinical status. Each aEEG strip was reviewed after discarding recordings with impedance exceeding 20 kΩ or artifacts. Interpretation of aEEG recordings were based on standard technique as described in the Natus CFM manual as well as the data published and validated in the literature [17]. The minimum and maximum amplitude (μV), presence of sleep-wake cycle (SWC), and bandwidth variability was recorded. A normal aEEG trace was defined as having all of the following: (1) Lower amplitude margins > 5μV, (2) An upper amplitude margin of > 10μV, (3) bandwidth variability between 5–15μV and (4) Presence of SWC, defined as sinusoidal elevations of baseline trace lasting longer than 20 minutes. An abnormal trace was described as following: (1) Discontinuous pattern: An upper amplitude margin > 10μV with lower margin <5μV. (2) Absence of SWC: No identifiable sinusoidal trace in continuous aEEG recording, Fig. 1(A–D).
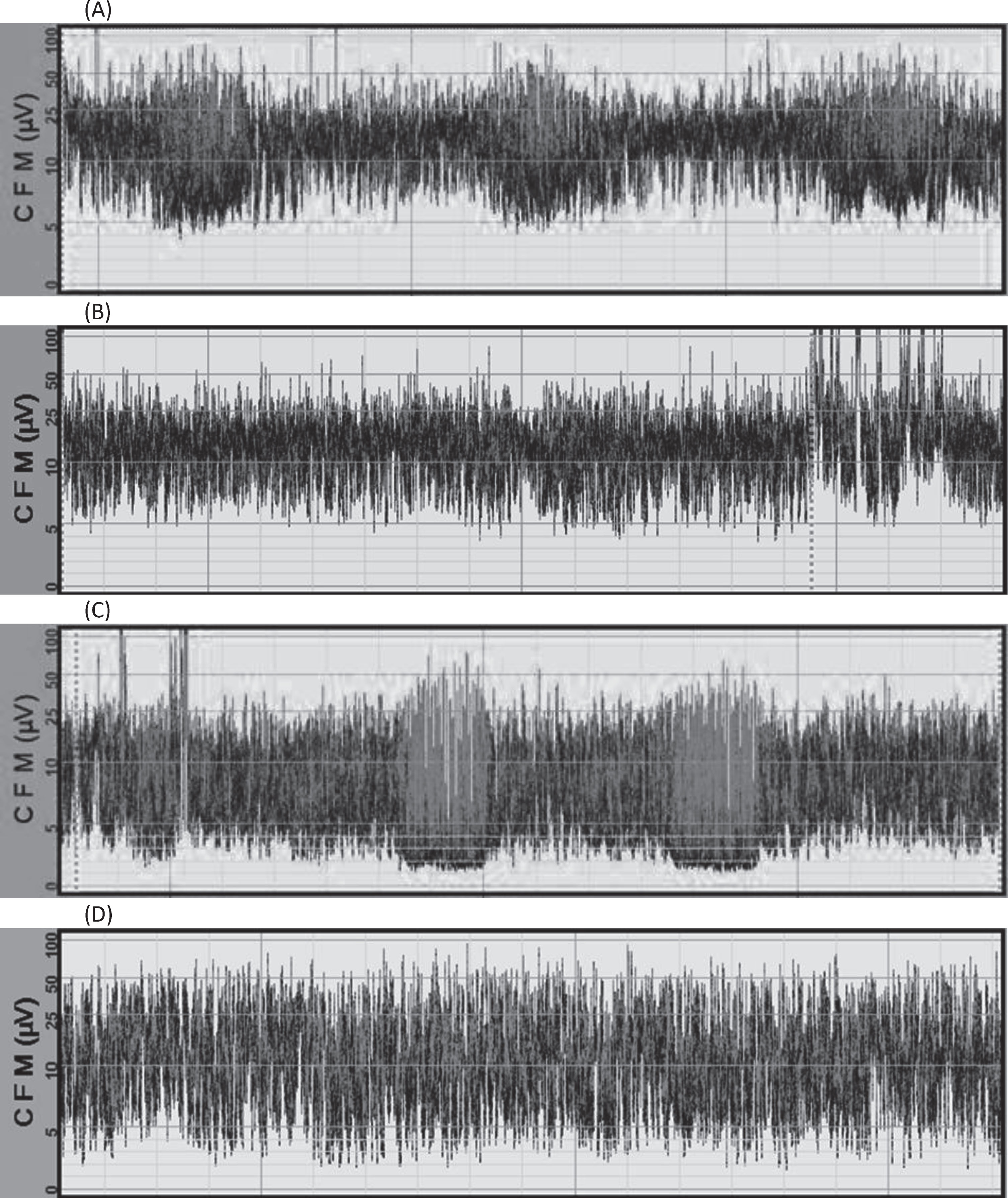
(A): Patient with continuous variability and presence of sleep-wake cycle. (B): Patient with continuous variability and no sleep-wake cycle. (C): Patient with discontinuous variability and presence of sleep-wake cycle (D): Patient with discontinuous variability and no sleep-wake cycle. [Dotted (...) lines on aEEG are infant care markers].
Comparisons between groups were performed with the t-test or Mann–Whitney U-test as applicable and with χ 2-test for categorical variables. A logistic regression model was used to determine predictors for discontinuous variability and absence of sleep-wake cycle correcting for prematurity (gestational age less than 37 weeks) and a diagnosis for NAS. The odds ratio was reported with 95% confidence interval. The level of significance was set at P < 0.05.
Results
A total of 59 infants were enrolled for the study, 23 infants with neonatal abstinence syndrome and 36 infants as their gestational age matched controls. Gestational age, birth weight and gender were similar in both groups. Compared to control subjects, mothers of infants with NAS were older, identified as Caucasian white, and were more likely to be active tobacco smokers, Table 1. Among the NAS infants, 18 (78%) mothers were enrolled in opioid maintenance programs during pregnancy, of which 12 mothers were enrolled in methadone and 6 mothers were enrolled in buprenorphine treatment programs. Concurrent use of other prescription or illicit substances was seen in the study group. Benzodiazepine and cannabinoids being the most common. There were two mothers who also had a history of concurrent cocaine abuse. In the study group, urine drug screening was available for 96 % (n = 22) of mothers and for 100% (n = 23) of NAS infants. While only 31% (n = 11) of mothers and 11% (n = 4) of infants in control group had a urine drug testing available; all of which were reported as being negative.
General Characteristics
General Characteristics
AA: African-American, CI: Confidence interval; LOS: length of stay; PNC: prenatal care. Values are expressed as mean±s.d. or median (interquartile range) or n (%). P-Values derived from Wilcoxon-Mann-Whitney test or χ 2 test.
Results of all aEEG characteristics are shown in Table 2. Infants underwent an aEEG recording within 21.6±16.8 hours of life, and prior to the initiation of NAS treatment. In our study group, 78% of NAS infants had an abnormal aEEG trace, with either a discontinuous pattern (61%) or an absent SWC (39%) and six (23%) study infants had both. None of the aEEG tracings showed an evidence of seizures.
aEEG Characteristics
CI: Confidence interval; DOL: day of life; SWC: sleep-wake cycle. Values are expressed as mean±s.d. or n (%). P-Values derived from Wilcoxon-Mann-Whitney test or χ 2 test.
Furthermore, to evaluate the possible effect of prematurity on the aEEG findings we devised a logistic regression model controlling for the prematurity (GA < 37 weeks). We saw that having NAS, increased the odds of not having a SWC; (p = 0.03) and increased the odds of having a discontinuous pattern (p = 0.01). Table 3.
Abnormal aEEG findings based on risk factors
NAS: neonatal abstinence syndrome. Logistic regression model.
We have shown in our pilot study that a majority (78%) of our infants with NAS had an abnormal tracing on an aEEG with either a discontinuous background activity or absence of a sleep-wake cycle within first 48 hour of life.
Infants exposed to opioids in-utero exhibit aberrant neuro-physiological behaviors and these sign or symptoms are the basis for various NAS scoring tools. Despite their widespread acceptance, these tools are not designed to predict neuro-developmental and behavioral outcomes of infants with neonatal abstinence syndrome [18, 19]. At the same time, there are other potential factors that can affect newborn outcomes like type (high versus low dose) and duration of different opioids, presence of polysubstance use, and genetic/epigenetic and socio-economic factors [6 , 20–25]. Pending any other objective assessment tool available to assess NAS infants as well as to possibly predict neurological outcomes, an aEEG is a promising modality. It can be performed at bedside, is very well tolerated by infants, and provides a continuous longitudinal cerebral monitoring without disrupting routine clinical care [26].
The ideal timing of aEEG is debated but if done between 36 and 48 hours of life, the results are very predictive and are validated for use in critically ill infants [27]. Another aspect of timing for aEEG during acute illness is the recovery of abnormal aEEG trace overtime [11 , 28]. In our study, we performed the initial bedside aEEG within first two days of life and prior to initiation of treatment for NAS with morphine. By doing this, we approached the validated timing as well as removing potential drug’s effects on aEEG activity. Thus, we can assume that the aEEG pattern was exhibited without external influences and reflects infant’s true brain activity.
Much experience for clinical utility of the aEEG has been amongst infants with hypoxic-ischemic encephalopathy (HIE) [16 , 29], but it has also been studied in a variety of other neonatal pathologies in term as well as preterm infants for assessment of background abnormalities or seizure activity [17]. Multiple follow up studies among the high-risk infants show that abnormalities seen on aEEG background activity, such as discontinuous and or burst-suppression, will reliably predict risk for poor neurological impairment because of a high sensitivity and specificity [12, 16]. Disturbances of background activity on an aEEG that is obtained within hours of birth, as well as abnormalities persisting over time are also highly predictive of poor neurological outcomes [10 , 31]. Authors even recommend that an abnormal aEEG background activity be used for counseling parents regarding infant’s neurological status [32, 33].
Another important assessment parameter on an aEEG is presence or absence of SWC [27 , 35] Deviations in the structure or time spent on various elements of sleep-wake cycles on conventional EEGs (cEEG) are used to predict abnormal development in children [36]. Sleep studies done in infants with NAS also showed abnormal patterns with a decrease in time spent on quiet sleep with increase in time spent on active sleep coinciding with the degree & type of opioid exposure, need for treatment for NAS, and a marked increase in the plasma concentration of the endogenous opioid peptides [37 –39]. Authors speculate that these effects of prenatal substances like heroin and cocaine/crack effect infant’s sleep structure and are potentially secondary to: change in mass organization and excitability of groups of neurons, perturbation of endogenous opiates, reorganization of the brain, and possibly fewer interhemispheric neuronal connections as a consequence of fetal exposure [40 –42]. Among extreme premature infants (25–27 weeks), a cycling pattern on an aEEG resembling sinusoidal waves are seen with subsequent maturation into distinct sleep-wake cycles at post-menstrual (PMA) ages of 35–37 weeks [43 –46]. In term [47], as well as preterm infants [10], an absence or a delay in the maturation of SWC appears to be a very specific sign of brain damage. In our study 39% infants with NAS had absence of SWC on their aEEG, even after controlling for prematurity (<37 PMA).Thus we can state that an absence of SWC on aEEG is a predictor of unfavorable outcomes in NAS infants.
This is a pilot study with ongoing recruitment and planned long-term developmental assessments with standardized tests. This study has several strengths. This is a prospective case-control study with gestational age matched healthy controls. Exposure to opioids in infants with NAS was confirmed with urine and umbilical drug screenings. All recordings were assessed by a single study neonatologist experienced at evaluating aEEGs thus retaining a consistent approach for all infants. We have shown that bedside amplitude encephalogram can be an adjunctive tool for assessment of infants with NAS.
Our study has several limitations. This is a single center study and presently we do not have follow up data on neuro-developmental outcomes. We are presenting data from the initial aEEGs that were obtained within the first two days of life. However, we are assessing the repeat aEEG recordings which were obtained during NAS treatment and off NAS treatment as well as a pre-discharge aEEG recording. The outpatient neurodevelopment data will be collected and once completed, we will be able to assess whether the aEEG normalized overtime and if it will correlate that with the neurodevelopmental outcome.
In conclusion, a bedside aEEG is a reliable tool for the assessment of infants with NAS and for screening newborns with prenatal opioid or benzodiazepine, and other poly drug exposures. Since many studies in neonates have shown that abnormal background activity and absence of SWC predict short and long-term neurodevelopmental outcomes, we postulate that aEEG can be utilized in assessment of infants with neonatal abstinence syndrome.
Funding source
The project was in part supported by funds from The Department of Pediatrics/Division of Neonatology, UTHSC, Memphis TN.
Conflict of interest
The authors have indicated they have no potential conflicts of interest to disclose.