
Abstract
BACKGROUND:
Preterm-born children are at higher risk for impaired linguistic abilities than are their term-born peers. The aim of the current study was to determine early predictors for delayed linguistic skills in very preterm-born preschool children.
METHODS:
Between January 2005 and November 2010 all very preterm infants born at < 32 weeks gestation in Tyrol were prospectively enrolled (n = 421); 248 of them had a detailed examination at the age of five years including cognitive assessment (Wechsler Preschool and Primary Scale of Intelligence, third edition (WPPSI-III) or Snijders-Oomen Nonverbal Intelligence Tests (SON-R)) as well as a screening test for language skills (Bielefelder screening for early diagnosis of reading problems and weak spelling (BISC)). The association between pre-and postnatal factors and poor performance on the BISC assessment was analyzed by means of logistic regression analysis.
RESULTS:
Of the 248 children 79 (31.8%) showed delayed literacy precursor skills. Male sex, gestational age, retinopathy of prematurity (ROP) grades 3–4 and low maternal education were predictive for delayed linguistic skills at 5 years of age in the multivariate analysis.
CONCLUSION:
This study identified predictors for delayed literacy precursor skills. These data support the finding that in very preterm infants pre-and perinatal as well as sociodemographic factors account for linguistic skills in the preschool period.
Abbreviations
Bielefelder screening for early diagnosis of reading problems and weak spelling Chronic lung disease Intracranial hemorrhage Necrotizing enterocolitis Periventricular leukomalacia Retinopathy of prematurity Small for gestational age Snijders-Oomen Nonverbal Intelligence Test Wechsler Preschool and Primary Scale of Intelligence, third edition
Introduction
In European countries 1.1% – 1.6% of live births are very preterm [1]. The number of neonates surviving very preterm birth has gradually increased due to advances in perinatal and neonatal care. However, increasing survival is linked to an increased awareness for morbidity with regard to the cognitive and behavioral outcomes of these children [2]. In addition, previous research has shown that very premature birth is associated with deficits in preschool abilities [3]. Particularly delays in vocabulary and grammar competence and communication skills are reported [4 –6]. Even in the absence of major disabilities lower linguistic achievement of premature children remains evident [7]. Moreover, it has also been shown that impaired linguistic skills at a preschool age have an impact on long-term educational, behavioral, and social problems [8, 9]. However, little is known about biological and environmental predictors for linguistic problems in preterm infants that may enhance early detection of impairment und improve efficacy of interventions during critical periods of development.
The aim of this study is to characterize risk factors for impaired literacy precursor skills of preterm-born children. To the best of our knowledge, this is among the largest studies to investigate this issue in a geographically defined cohort of very preterm-born children at a preschool age.
Methods
Participants
The study survey area was Tyrol, a state in western Austria with 680000 inhabitants and about 7000 live births per year. All infants born before 32 completed weeks of pregnancy at Innsbruck Medical University Hospital, the only neonatal intensive care unit in the geographical region, were enrolled (study period January 2005 to November 2010). During the study period there were 421 live births. Of these children 25 died and 55 were non-residents or moved out of the region. Ten children with severe disabilities, classified according to Wood et al. [10], who were not able to perform any tests, were excluded. Consequently, 331 children were invited for a detailed follow-up visit. A total of 83 parents (25.1%) refused the invitation, leaving 248 patients who formed the study population (Fig. 1). None of the patients in the study population had hearing problems requiring a hearing aid.
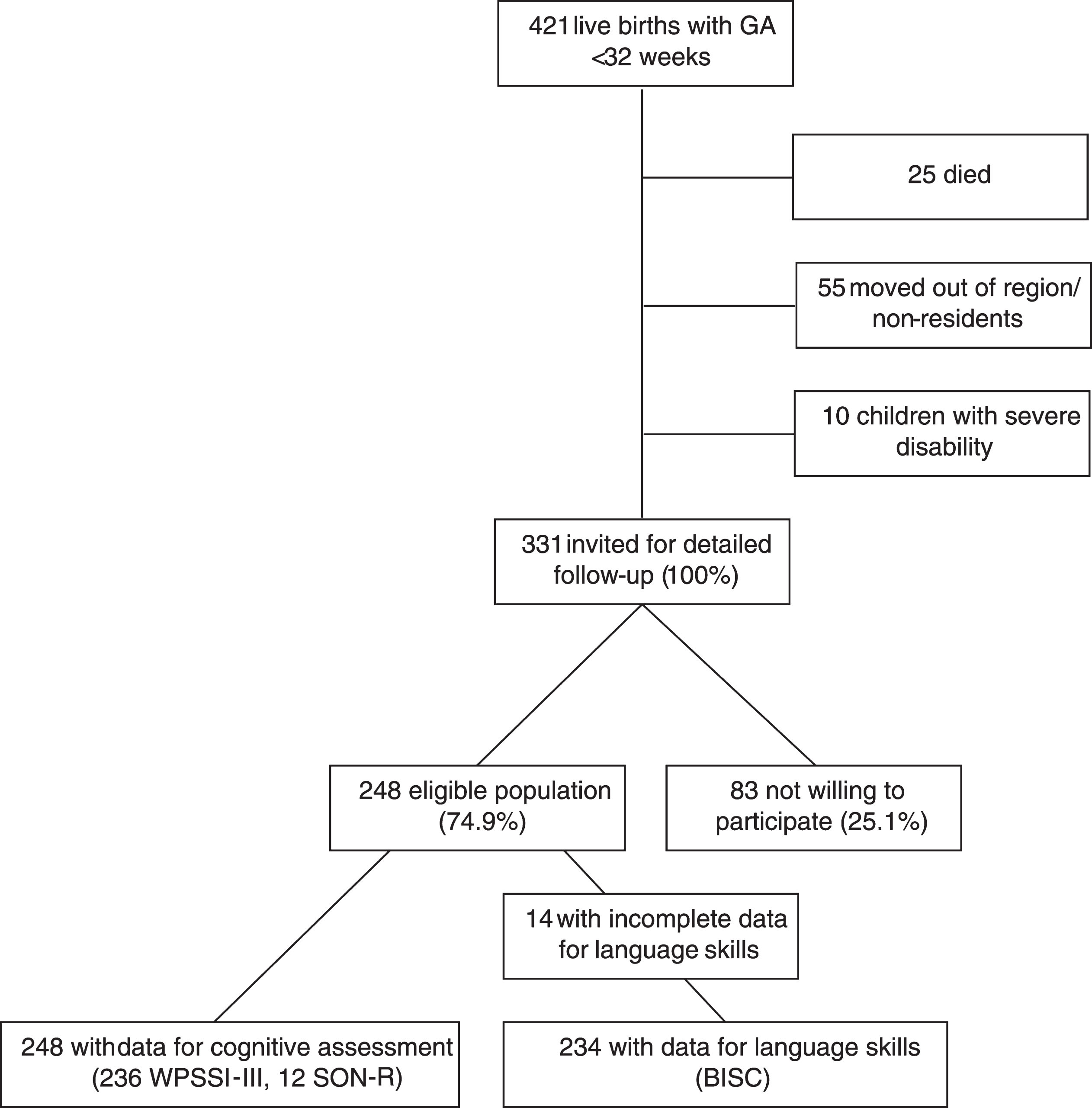
Flow-chart for inclusion of very preterm infants. GA: gestational age; IQ: intelligence quotient; WPSSI-III: Wechsler Preschool and Primary Scale of Intelligence, third edition; SON-R: Snijders-Oomen nonverbal intelligence test.
Participants compared to non-participants were less likely to have a mother with an education of < 12 years (p < 0.001). There was no difference regarding maternal age, smoking in pregnancy, antenatal steroid use, gestational age, birthweight, sex, small for gestational age (SGA), preterm premature rupture of membranes (PPROM), early-and late-onset sepsis, chronic lung disease (CLD), intracerebral hemorrhage (ICH), severe retinopathy of prematurity (ROP) and necrotizing enterocolitis (NEC).
All clinical data were prospectively collected. Maternal and neonatal data included maternal age, maternal years of education, smoking in pregnancy, antenatal steroid use, gestational age (full weeks of gestation), birth weight (grams), SGA, multiple birth, sex, postnatal surfactant use, diagnosis of early-and late-onset sepsis, CLD, ICH, NEC, and severe ROP. Gestational age was calculated from the first day of the last menstrual period. This was compared with assessment of gestational age by ultrasound scans performed before 24 weeks. If there was a difference of more than one week between menstrual and ultrasound assessment, the scan assessment was preferred. Growth charts developed by Fenton et al. [11] were used to classify infants as SGA at birth, defined as a birth weight lower than the 10th percentile for sex and gestational age. PPROM was defined when the rupture of membranes occurred before 37 weeks of gestation and more than 24 h before the onset of labor. CLD was defined as oxygen dependence at 36 weeks postconceptional age. NEC was defined according to Bell’s criteria [12] and was classified as medical (clinical symptoms and signs plus evidence of pneumatosis on abdominal x-ray) or surgical (histological evidence of NEC on surgical specimens of intestine). ICH was classified according to the method of Papile et al. [13]. Infants with cystic periventricular leukomalacia (PVL) included those with ultrasonographic findings suggesting cystic degeneration of periventricular white matter. Ultrasound examinations were routinely performed on the second and fifth day of life, thereafter every week and finally every second or third week. A diagnosis of early-onset (≤72 hours after birth) or late-onset (>72 hours) sepsis required signs of generalized infection, a positive blood culture and antibiotic therapy for five or more days. Information on smoking habits and years of education was obtained during the stay at the neonatal department. Smoking habits in pregnancy (yes/no) were based on self-reported data.
Follow-up/Neurodevelopmental outcome
All children with a gestational age of < 32 weeks are regularly invited for follow-up visits until they enter school. The follow-up visit at 5 years of age includes an interview with the children’s mothers or other primary caregivers, a physical and neurological examination, assessment of cognitive development using the German version of the Wechsler Preschool and Primary Scales of Intelligence (WPPSI-III) [14]. In children with German not being their mother tongue and other language difficulties, the Snijders-Oomen Nonverbal Intelligence Test (SON-R) was used [15].
On the WPPSI-III, six of the core-subtests were administered (Block Design, Information, Matrix Reasoning, Vocabulary, Symbol Search, Coding), and then verbal intelligence quotient (IQ), performance (IQ) and the processing speed quotient were calculated from the subscales. Estimated full-scale IQ was measured using a reliable and valid short form of the WPPSI [16, 17]. Each scale or index is age-standardized, with a mean of 100 (SD, 15) and a scale of < 85 (>1 SD below the mean) indicating delay and a scale of < 70 (>2 SDs below the mean) indicating significant delay.
Cognitive delay was defined as a full-scale IQ < 85 in either the WPSSI-III or the SON-R test. Children in whom a score could not be calculated because of severe mental delay were also classified as having delayed cognitive abilities.
In addition, the children were assessed individually with the Bielefelder screening (BISC) for early diagnosis of reading and spelling difficulties [18]. The BISC is based on the assumption that an inadequately trained phonological awareness as well as attention and memory problems in preschool age are responsible for impaired literacy skills such as reading and spelling in school. This diagnostic tool is based on several different tasks (e.g. repeating pseudo-words, rhyme identification, naming the colors of uncolored or incongruent objects, segmenting syllables, sound-to-word). Each subtest contains ten items and one risk point can be reached. According to the BISC manual a score of up to two risk points is normal, three indicates a marginal threshold and a score of four or higher indicates later reading and spelling difficulties. For statistical analysis two groups were formed (≤ two risk points normal performance group and > two risk points poor performance group).
Children in whom a score could not be calculated because of severe delay in language performance (n = 14) were also classified as having delayed language skills and added to the poor BISC performance group.
All cognitive tests were performed by one of the three experienced psychologists.
The study was approved by the Ethics Committee of the Medical University of Innsbruck (study No. AN2013-0086 333/4.2).
Statistical analysis
Data analysis was performed with SPSS software, version 20.0, for Windows (SPSS Inc., Chicago, IL, USA). Categorical data were compared using the chi-squared or Fischer’s exact test. Multivariate risk profiles for delay in literacy precursor skills were computed by means of logistic regression analysis using a stepwise forward selection procedure with in- and exclusion criteria as follows (PI < 0.05 and PE > 0.10).
Results
Table 1 summarizes maternal, pre-, peri- and neonatal data for the population of children born before 32 gestational weeks in the normal (n = 169) and the poor (n = 79) language performance group. Except for the prevalence of low maternal education (<12 years) (p < 0.001), low gestational age (p = 0.02), low birthweight (p = 0.04), male sex (p = 0.020), early-onset sepsis (p = 0.014), CLD (p = 0.03), severe ROP (p = 0.022) and late-onset sepsis (p = 0.022), no significant differences between these two groups were seen regarding all other maternal, pre-, peri- and postnatal variables.
Sociodemographic and neonatal characteristics of preterm infants with a gestational age of less than 32 weeks according to language skills at 5 years of age
Sociodemographic and neonatal characteristics of preterm infants with a gestational age of less than 32 weeks according to language skills at 5 years of age
CLD: chronic lung disease; ICH: intracerebral hemorrhage; PPROM: preterm premature rupture of membranes; PVL: periventricular leukomalacia; NEC: necrotizing enterocolitis; ROP: retinopathy of prematurity; P values are from Fischer’s exact test or T test, as appropriate. In all variables the proportion of missing data was < 5%.
Full assessment of cognitive abilities at five years of age was available in 248 of the 331 children. A total number of 219 (88.3%) achieved normal estimated full-scale IQ rates (between 85 and 115), 23 (9.3%) children were classified as having cognitive delay (estimated full-scale IQ between 85 and 70), and six (2.4%) children had significant cognitive delay (estimated full-scale IQ < 70). Cognitive or significant cognitive delay was much more frequent in those with poor (26 out of 79 children; 32.9%) than in those with inconspicuous BISC results (3 out of 169 children; 1.8%). There was a good correlation between BISC and verbal IQ results (Spearman correlation coefficient 0.268, p < 0.001).
In the multivariate analysis fitted with a stepwise selection procedure low maternal education (<12 years) (odds ratio 2.03 [95% confidence interval 1.09–3.79], p = 0.025), low gestational age (odds ratio 1.26 [95% confidence interval 1.08–1.48], p = 0.004), male sex (odds ratio 1.90 [95% confidence interval 1.01–3.59], p = 0.046), and severe ROP (odds ratio 2.25 [92% p = 0.095) remained significant risk predictors for delayed literacy precursor skills (Table 2).
Multivariable association between risk variables and delayed language skills at 5 years of age
CI: confidence interval; OR: odds ratio derived from logistic regression analysis of risk variables for delayed psychomotor development. The multivariate model was fitted with a forward stepwise selection procedure.
When separately focusing on children with a gestational age of≤30 weeks (n = 163) and > 30 weeks (n = 85), low maternal education showed similar associations with delayed linguistic skills in both age groups (2.29 1.18–4.47], p = 0.015, and 3.09 [0.82–11.58], p = 0.094), whereas gestational age and sex were relevant only in the younger ones (1.30 [1.09–1.56], p = 0.004, and 1.69 [0.86–3.32], p = 0.128).
Preterm-born children are at higher risk for language impairment than are their term-born peers[4, 6 , 19–23]. Reidy et al. reported low language scores in 20.3% to 30.1% of children born < 30 weeks of gestation at an age of 7 years. This very preterm group performed significantly more poorly than did controls regarding all language subdomains [24]. Similar findings were reported by other groups [25 –37]. In our cohort, 31.8% of the very preterm infants had poor results in the BISC test at the age of five years. Of the 79 children with impaired literacy precursor skills 26 had an IQ score < 85 in WPSSI-III and SON-R, whereas the other 53 children showed delayed language skills but a normal IQ, which clearly shows that learning difficulties are not necessarily related to global cognitive deficits.
Identifying children at risk for impaired language skills at an early age and offering support for those who show linguistic delay is of special importance. There is evidence that early training of phonological awareness at preschool age and intervention-oriented child development programs in this age-group positively influence linguistic skills and help improve school readiness [38, 39]. In 1988 Lundberg et al. were able to show beneficial short- and long-term effects on linguistic skills in Scandinavian children by offering a metalinguistic training program to pre-schoolers [40]. A German study replicated and extended these results [41]. A metanalysis including 19 German studies examined the effectiveness of training programs and showed significant benefits in those who were already trained in kindergarten [42].
In our cohort gestational age emerged as a significant risk predictor for delayed linguistic skills at five years of age suggesting that the most immature babies are at highest risk for impaired language development. This finding is in contrast to Reidy et al. [24], who revealed no difference in language scores in the gestational age groups < 26 weeks and 26 to 30 weeks, but is consistent with results from other studies that found the greatest risk for cognitive impairment including language performance in the most immature children [43, 44]. The relation between impaired linguistic skills and severe retinopathy in our cohort may also reflect the fact that the most immature and sick babies are at highest risk. Deficits in language abilities in former preterm babies may result from specific brain abnormality, especially reductions in cerebral tissue volume [45] and altered microstructure and connectivity [22]. Moreover, preterm children have significantly greater bilateral temporal lobe gyrification than do term controls [46]. Brain injury in the Broca and Wernicke areas of the dominant hemisphere is a strong predictor for subsequent language impairment [47 –49]. However, preterm-born children are at higher risk for linguistic impairment, even in the absence of brain damage [23].
In addition, low maternal education was associated with a two-fold risk for delayed linguistic skills at the age of 5 years in our preterm cohort, which is in accordance with the current literature [32 , 50–52]. Hoff et al. particularly focused on mechanisms by which socioeconomic status could influence the children’s productive vocabulary development and reported that mothers with lower educational status more frequently use shorter utterances and less complex vocabularies when talking to their children [53]. Voss et al. added quality of cognitive stimulation, parenting style, better health behaviour, higher quality of child care, superior utilization of follow-up care services and also genetic dispositions as further possible explanations for a better cognitive outcome including linguistic abilities in extremely low birthweight children [54].
The current study shows an increased risk for boys as compared to girls regarding delayed literacy precursor skills at a preschool age. In line with this, Yliherva et al. identified male sex as a predictor for poor linguistic skills at the age of eight in low birthweight children [55]. Interestingly, in the study by Jennische et al. the male preterm subgroup who had required neonatal intensive care (NIC) treatment after birth performed more poorly in language skills at the age of 6 than did the female NIC group, but performed similar to the (full-term born) control boys. Contrarily, the NIC girls did not reach the level of control girls [30]. These data support our finding that the male preterm-born children more frequently show language disabilities than do female ones. Furthermore, it indicates a possibly stronger influence of preterm birth on language development in girls than in boys. In a previous review of early linguistic development in healthy children a small but consistent female advantage was reported that seemed to disappear over the years and could not be seen among adults any more [56]. Therefore, it is difficult to define whether male sex per se is a risk factor for language disabilities or whether boys in general simply score lower in verbal testing during early development.
A strength of the current study is its size. With 248 preschool children included, to our knowledge it is among the largest studies investigating the relationship between prematurity and language performance at a preschool age [26 –38]. Moreover, a broad range of prospectively collected data on the pre-, peri-, and postnatal period as well as data on the sociodemographic background such as maternal education and data from the follow-up visit at the age of 5 were available in our cohort.
It should be mentioned, however, that participation was incomplete (participation rate 74.9%). Non-attendance in the follow-up assessment was significantly higher in mothers with lower educational levels. Hence, it is possible that the impact of maternal education on poor language outcome has even been underestimated.
In conclusion, the current study identified sociodemographic variables, male sex and low gestational age as risk predictors for delayed preschool literacy precursor skills. Identification of children at risk and early educational support for this group may help counteract school problems and improve academic and social performance in later life.
Ethics statement
I declare that the research is the original work of the authors. The study was approved by the Ethics Committee of the Medical University of Innsbruck.
Funding
There was no source of funding.