
Abstract
BACKGROUND:
The efficacy of macrolide treatment on gastrointestinal motility and acquirement of feeding tolerance in extremely low birth weight (ELBW) infants are controversial. This study aimed to evaluate clinical effects of parenterally administered erythromycin (EM) and clarithromycin (CAM) on gastrointestinal motility in ELBW infants.
METHODS:
ELBW infants treated in Tokyo Medical University Hospital were retrospectively studied. Several outcomes of ELBW infants treated with EM or CAM were compared with those recognized before initiation of the medication, as well as with those of patients with no macrolide treatment. The primary outcomes included average gastric residual volume that was evaluated 3 hours after enteral feeding. Secondary outcomes were the number of patients who developed feeding intolerance, stool frequency, and other adverse events, such as respiratory comorbidities and pyloric stenosis.
RESULTS:
Among a total of 53 infants, 20 and 13 were treated with EM and CAM, respectively, whereas 20 infants were not administered macrolides. The gastric residual volume was significantly decreased after initiation of medication compared with before medication in the EM group, whereas that of the untreated group showed no change. When the EM and CAM groups were combined, the gastric residual volume was also significantly decreased after treatment compared with before treatment. An increase in stool frequency and pyloric stenosis were not observed in the groups.
CONCLUSION:
EM might be effective for acquiring feeding tolerance in ELBW infants. A future prospective study with a larger population is required to determine the efficacy of CAM.
Background
Macrolides, including erythromycin (EM) and clarithromycin (CAM), have several effects besides antibacterial activity, mainly on respiratory and gastrointestinal systems [1–5]. The effect of macrolides on the respiratory system includes decreasing fluid and mucin secretion, improvement of ciliary activity, and suppression of inflammatory cytokines. These processes then prevent mucosal remodeling of the airway tract, whereas the effect of macrolides on the gastrointestinal system is by activity as a motilin receptor agonist [3, 4]. Motilin is a hormone secreted from duodenal mucosa, and it exacerbates gastroduodenal motility via receptors in smooth muscles [6]. Therefore, macrolides are often used to treat paralytic ileus and for optimized upper gastrointestinal endoscopy in adult patients in expectation of motilin receptor stimulation [6].
In the neonatal intensive care field, macrolides are often used, especially for preterm infants, to prevent chronic lung disease (CLD). Physicians rely on the antibacterial activity of macrolides and its effects on the respiratory system, despite limited evidence of its efficacy [7, 8].
Feeding intolerance is a serious problem that develops in preterm infants because of immaturity of the gastrointestinal system, a risk factor of body growth failure, sepsis due to long-term intravenous nutrition, aspiration pneumonia, abdominal distention, and necrotizing enterocolitis (NEC). Although gastrointestinal effects of macrolides may be feasible to this problem, the efficacy of macrolides is still controversial because of variable study designs of previous reports [9]. Additionally, to the best of our knowledge, no studies have evaluated the efficacy of CAM.
In this study, we evaluated the clinical effect of enterally administered EM and CAM on gastrointestinal motility in extremely low birth (ELBW) infants using retrospectively collected indicators.
Materials and methods
Study design
The study was retrospectively conducted in Tokyo Medical University Hospital (TMUH), Tokyo, Japan. Data of each patient were collected using medical records. All guardians of the subject have given their written informed consent and the consent form has been approved by the ethical committee on human research of TMUH.
Study groups
ELBW infants (birth weight <1000 g) admitted to, treated in, and discharged from the neonatal intensive care unit of TMUH during January 2013 to December 2016 were included. Exclusion criteria were as follows: (1) patients who died before discharge; (2) patients with congenital anomalies, such as chromosomal abnormalities, congenital anomalies of the gastrointestinal system, and circulatory symptomatic congenital heart disease, such as tetralogy of Fallot; (3) patients who developed feeding intolerance before initiating macrolides; (4) patients who developed NEC before initiating macrolides, (5) insufficient data; and (6) no parental consent.
In our institute, enteral nutrition is started when the patient’s cardiopulmonary state stabilizes. This state is not well defined, but is usually considered when the patient’s blood pressure and heart rate are within the normal range of his/her age, no requirement for a high fraction of inspired oxygen (i.e., <50%), and the clinical impression is interpreted by the attending physician. Breast milk was the initial nutrition provided, with a dose of 1–2 mL/kg/dose×eight times/day. Volume was gained every 12 or 24 hours with an additional dose of 1–2 mL/kg. Synthetic milk and medication, such as aminophylline, caffeine, iron, and phosphorus preparation, were initiated after the milk dose reached 60–100 mL/kg/day. Enteral nutrition was provided via a gastric tube before the corrected gestational age of 34 weeks + 0 days. Immediately before tube feeding, the gastric residual volume (i.e., undigested and remaining milk in the stomach) was aspirated via a gastric tube and its volume was routinely recorded. When the ratio of gastric residual volume/planned milk volume exceeds 0.2, the gastric residual was given via gastric tube again, and the gastric residual volume was subtracted from the planned milk volume (i.e. the total given volume was same as the planned volume).
Macrolide administration
Indication of macrolide administration to each patient depended on the decision of the attending neonatologist. Each neonatologist made his/her decision concerning the patient’s respiratory state (i.e., presence of chronic lung disease, oxygen demand, and pressure support demand). Neonatologists then initiated enteral macrolide administration in expectation of a reduction in inflammatory response and colonization of inflammation-inducing pathogens, improvement of ciliary function in the lungs, and finally, prevention of CLD in an empiric manner. EM and CAM are used as macrolides in our institute. The delineated criteria for which medication should be used in each case were not firmly defined. Therefore, the choice of medication depended on the attending neonatologist’s decision. Doses of EM and CAM were 5–10 mg/kg/dose×two times/day, dissolved in 1 mL of milk, and administrated by a syringe directly into the stomach via a gastric tube.
The patients were divided into four groups as follows: (1) administration of EM (EM group), (2) administration of CAM (CAM group), (3) administration of EM or CAM (combination of the EM and CAM groups; treated group), and (4) no administration of EM or CAM (untreated group). Treated group was included in this study to evaluate the effect of macrolide group antibiotics as whole.
Data collection
We collected background characteristics of the patients, including sex, gestational age, birth weight, number of twins, Apgar score at 1 and 5 minutes, and the median day of macrolide initiation after birth. We also recorded the number of patients who were diagnosed with CLD, symptomatic patent ductus arteriosus, Surgical NEC, intraventricular hemorrhage, periventricular leukomalacia, retinopathy of prematurity requiring laser photocoagulation, requirement for home oxygen therapy, and the duration of respiratory support with artificial ventilation and hospitalization as complications and comorbidities.
Each complication and comorbidity were defined as follows. CLD was defined as the requirement for oxygen or respiratory support at the corrected age of 36 weeks. Symptomatic patent ductus arteriosus was defined as the requirement for treatment with indomethacin and/or surgical procedure. Because of clinical difficulty to diagnose medical NEC firmly, surgical NEC was selected as the studied outcome, which was defined as development of intestinal perforation. Intraventricular hemorrhage and periventricular leukomalacia were defined as lesions that were recognized by echogram and/or brain magnetic resonance imaging.
As the primary outcome, gastric residual volume (i.e., volume of the stomach content evaluated just before administration of each parenteral tube feeding) was collected. The ratio of gastric residual volume/volume of milk provided at that time was calculated. The observational period was from three days before to three days after initiating macrolide administration for the EM, CAM, and treated groups. The observational period for the untreated group was from the 9th to 15th days after birth because the median age of initiating macrolides in the treated group was day 12. Three, two, and one day before initiation of macrolides were defined as the pre-intervention period, and one, two, and three days after initiation were defined as the post-intervention period. The mean ratio of the gastric residual volume/milk volume provided was calculated in every patient for the pre- and post-intervention periods.
Secondary outcomes were the number of patients who developed feeding intolerance, the day on which the patient attained full feeding, the day on which the patient withdrew from intravenous nutrition, stool frequency during the observational period, and the number of patients who developed pyloric stenosis. Additionally, the mean ratio of gastric residual volume/milk volume provided was compared among the groups. Diagnosis of feeding intolerance was defined as the requirement for continuous parenteral feeding via a gastric or duodenal tube because of recurrent milk vomiting and reflux with the risks of milk aspiration and abdominal distention. The mean stool frequency per day was compared among the groups (from the day of macrolide initiation to three days after) and within each group (three days before vs three days after initiating macrolide). Pyrolic stenosis was evaluated when it was clinically suspected, therefore, recurrent vomiting and abdominal distention accompanied by abnormal enlargement of the stomach on X-ray were recognized. Pyrolic stenosis was defined as echographically determined stenosis of the duodenum with specific symptoms, such as recurrent vomiting and stomach enlargement.
Data analysis
Differences among groups were evaluated using the Mann–Whitney U test and chi-square test, and changes before and after initiating macrolides within each group were evaluated using the Wilcoxon signed rank test. Data were analyzed using IBMR SPSSR Statistics ver. 24 (IBM, New York, NY, USA). A p value < 0.05 was regarded as statistically significant.
Results
During the observational period, 73 patients were admitted to our institute. After recruitment according to the exclusion criteria mentioned above, 53 patients were eligible for the present study. Among these 53 patients, 20, 13, and 20 were categorized into the EM, CAM, and untreated groups, respectively (Fig. 1).
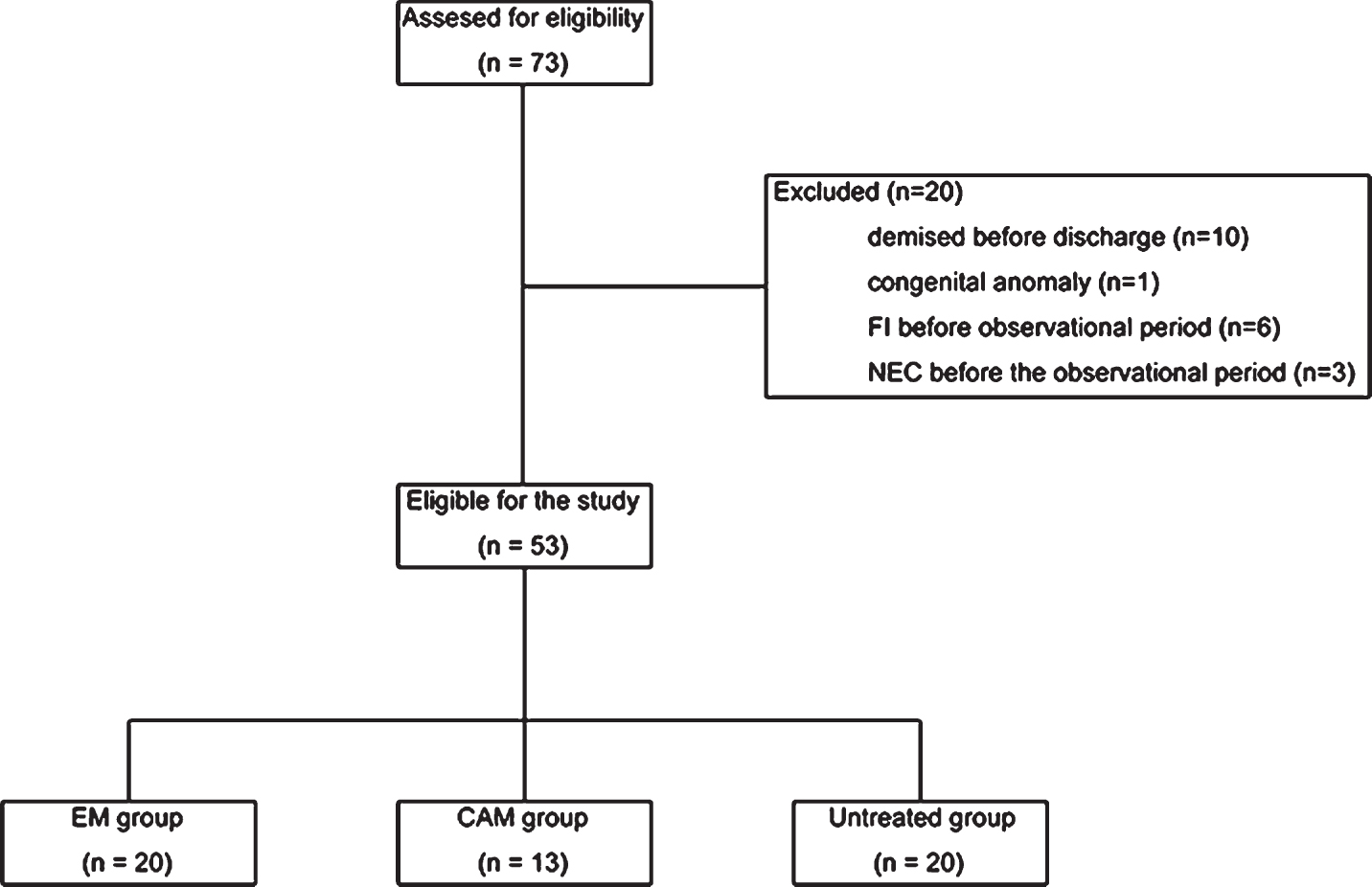
Diagram showing recruitment of subjects. FI, feeding intolerance; NEC, necrotizing enterocolitis; EM, erythromycin; CAM, clarithromycin.
The background characteristics of the patients are shown in Table 1. Gestational age and birth weight in the treated group were significantly lower than those in the untreated group (p = 0.045, p = 0.043, respectively), and the number of twins in the CAM group was significantly greater than that in the EM group (p < 0.01).
Background characteristics of the patients
Data are presented as the median (range) or n (%). ap < 0.01, compared with the untreated group; bp < 0.05, compared with the untreated group.
With regard to complications and comorbidities, the duration of artificial ventilation in the CAM group and the duration of hospitalization in the CAM and treated groups was longer than that in the untreated group (p = 0.032, p = 0.012, and p = 0.038, respectively, (Table 2). Additionally, the number of patients who developed retinopathy of prematurity and underwent laser photocoagulation in the treated group was greater than that in the untreated group (p = 0.035).
Complications and comorbidities of the patients
Data are presented as the median (range) or n (%). EM, erythromycin; CAM, clarithromycin; CLD, chronic lung disease; PDA, patent ductus arteriosus; NEC, necrotizing enterocolitis; IVH, intraventricular hemorrhage; PVL, periventricular leukomalacia; ROP, retinopathy of prematurity; HOT, home oxygen therapy. ap < 0.05, compared with the untreated group.
For the primary outcome, the mean gastric residual volume/milk volume provided ratio was significantly reduced after initiation of macrolides in the EM and treated groups, but the CAM and untreated groups showed no significant change (Table 3).
Primary outcome
Data are presented as the median value of each group. Pre, pre-intervention period; post, post-intervention period. The p values were obtained by the Wilcoxon signed rank test.
No significant differences in secondary outcomes were observed among the groups (Table 4). Stool frequency was not different between the pre- and post-intervention periods in all of the groups (data not shown). No patient was clinically suspected the development of pyloric stenosis.
Secondary outcomes
Data are presented as the median (range) or n (%). FI, feeding intolerance; IVN, intravenous nutrition.
There were three notable findings in the present study as follows. (1) Macrolides, especially EM, decreased the gastric residual volume when it was administered to premature infants. (2) No adverse events were observed in the treated group. (3) No significant differences in respiratory outcomes among the groups were observed.
In our study, gastric residual volume in the EM group was significantly decreased after initiating EM treatment compared with before treatment, but that in the untreated group did not change during the observational period. Additionally, although gastric residual volume in the CAM group did not show a significant decrease during the observational period, combining the CAM group with the EM group (treated group) showed statistical significance. In the clinical setting of neonatal intensive care, gastric residual volume is a commonly used indication of gastrointestinal motility [10, 11]. Sustained and/or recurrent recognition of a large residual volume is clinically considered to suggest feeding intolerance, development of NEC, and the risk of apparent or latent vomiting followed by aspiration pneumonitis [10, 11]. The significant decrease in this index found in the EM and treated groups suggests that macrolides enhance gastrointestinal motility. Prospective randomized control study is expected to elucidate this effect of EM on acquiring milk tolerance.
We found no apparent adverse effects, including NEC and pyloric stenosis, in our study. Stool frequency did not change in any of the groups during the observational period. This finding suggests that the effect of macrolides on gastrointestinal motility does not cause excessive excretion, or that this effect is mainly on upper gastrointestinal systems, such as the stomach. However, this finding should not be regarded as a direct adverse effect. The risk of pyloric stenosis is widely known, but still remains controversial as an adverse effect of neonatal use of macrolides [8, 13]. The present study suggested that macrolide administration might be safe during the acute phase in preterm infant intensive care. Further study with a larger population and long-term observation is essential for accurate evaluation of such risks.
We did not find any significant difference in the prevalence of CLD and requirement for home oxygen therapy in patients in the present study. A systematic review on the effect of EM on preventing CLD did not show favorable efficacy, whereas azithromycin and CAM were suggested to be effective in other studies [7, 15]. The present study was retrospectively designed and the duration of mechanical ventilation and hospitalization in the treated group was longer than that in the untreated group. This suggests that the treated group included more severe patients than the untreated group did, and there might be a selective bias. No significance in respiratory outcomes between the treated and untreated group may be the result of the substantial effect of macrolides.
The present study has several limitations. First, the number of subjects was relatively small. This small number could have resulted in the nonsignificant difference in efficacy to develop milk tolerance between the CAM and untreated groups. However, efficacy of developing milk tolerance between the EM and untreated groups showed superiority in EM use. We are unable to distinguish whether this non-significant finding was due to bias or a reflection of the specific characteristics of each medication. Second, the retrospective design of the study could have led to selective bias, as mentioned above. However, our retrospective study suggested that, with various confounding factors accompanied by the clinical setting, macrolide use may be effective in gastrointestinal motility and acquiring feeding tolerance. Third, there were no firm criteria indicating how to decide initiation of macrolides and which medication to be used. This limitation could have caused selective bias in that patients whose clinical impressions were relatively severe may have been assigned to the treated group by each attending physician. Regardless of these limitations, our finding that macrolides reduced gastric residual volume in premature infants is notable and indicates the potential for a further expanded study.
Conclusion
EM administration to ELBW infants is effective for developing milk tolerance without an increase in risk for adverse events. CAM might also have similar effects. Further prospectively designed studies with a larger population and long-term observational period, with the evaluation of an emergence rate of drug-resistant bacterium, are expected to determine more accurate significance regarding the effect of macrolides on care of premature infants.
Disclosures
The authors have no competing interests to disclose.
Statement of financial support
There are no funding sources for the present study.