
Abstract
BACKGROUND:
The aim of this study is to assess the effect of age at adiposity rebound (AR) and changes in growth between birth and 6 months on growth status at 8–9 years in children born term and preterm. Age at AR is inversely correlated with risk for later obesity in children born full term, but has not been analyzed in children born preterm.
METHODS:
Birth anthropometrics, and weight and length/height data from age 6 months through 8–9 years were recorded for 175 children born in 2008 in the military health system. Calculated variables include body mass index (BMI, kg/m2), Z-scores, and age at AR.
Results:
Age at AR could be calculated for 150 children (32% preterm); average age was 5.4 years and 5.3 years for children born term and preterm, respectively (NS). For children born term and preterm, there was a significant correlation between younger age at AR and higher BMI Z-score at 8–9 years (r = – 0.685), and a direct relationship between weight Z-score change from birth to 6 months and weight Z-scores at 8–9 years (p = 0.034).
CONCLUSIONS:
Younger age at AR correlates with higher BMI Z-score at 8–9 years in children born both term and preterm. Weight gain from birth to 6 months correlates with weight Z-score at 8–9 years. These results emphasize the importance of younger age at AR in addition to greater early weight gain as an indicator of later obesity.
Abbreviations
Adiposity rebound
Body mass index
Introduction
Childhood obesity continues to be a wide-spread epidemic, with prevalence increasing significantly over the last two decades [1, 2]. Obesity is associated with cardiometabolic consequences including metabolic syndrome, hypertension, insulin resistance, type-2 diabetes and cardiovascular disease. Infants born preterm are at greater risk for cardiometabolic sequelae than infants born full term [3–9]. The early development of increased fat mass in children born preterm may be a significant contributor to this increased risk for later obesity and cardiometabolic sequelae. In children born both preterm and full term, rapid weight gain from birth to early infancy and elevated BMI in the first year of life have been associated with increased risk of being overweight in early childhood [5, 11].
Body mass index (BMI) progressively decreases after mid-infancy and reaches a nadir at an average age of 4–6 years [10–15]. BMI then progressively increases thereafter. The age at which this increase begins is defined as the adiposity rebound (AR) and the younger the age at AR, the greater the risk for later obesity [12, 13]. The impact of early AR on later adverse cardiometabolic consequences appears to be mainly related to its association with increased adiposity, but also perhaps to dysfunctional adipose tissue [12]. Early AR is also strongly associated with increased BMI and increased fat mass index in adolescence [14]. The published data related to AR have only addressed children and adolescents born full term, with no reported data on AR in children born preterm.
The purpose of this study is to track the longitudinal growth of children born full term and preterm in the military health system in order to determine predictors of growth status at 8–9 years of age. Our specific objectives in both full term and preterm births are to study (1) the predictive importance of age at AR in relation to growth status at 8–9 years of age, and (2) the relationship of growth between birth and 6 months to growth outcomes at 8–9 years of age. We hypothesized that younger age at AR and greater growth between birth and age 6 months would both directly correlate with greater growth at 8–9 years.
Methods
This is an extended retrospective longitudinal follow-up of a large and well-characterized database of 501 preterm and 1423 full term infants born at 3 military health system hospitals in 2008. The birth anthropometrics and growth to NICU discharge in 1093 children (19% born preterm) have previously been published [16, 17]. The inclusion criteria included full term infants born at a gestational age of 37–42 weeks, and infants born preterm at < 37weeks gestation. Exclusions included infants with a suspected or confirmed disorder affecting growth, multiple births, or infants with missing maternal charts. Feeding regimen at hospital discharge was categorized as breast, bottle, or mixed. Small-for-gestational-age was defined as < 10th percentile and large-for-gestational-age as > 90th percentile for birth weight.
A subsequent analysis of growth to 4 years of age was previously conducted (Stokes T et al, Pediatric Academic Societies Annual Meeting, Baltimore, MD, May, 2013). Between birth and 4 years of age, weight and length/height were consistently less in preterm compared to term births (overall difference across all 4 years, p < 0.0001). Among 661 children with growth data at 4 years of age (35% born preterm), however, there was no difference between children born preterm and full term for weight, height, or BMI, both for all 661 children and among the 26% of these children (n = 175) with follow-up data to 8–9 years.
To extend this retrospective cohort study, we now report longitudinal growth status at 8–9 years of age. Weight (kg), length (cm) at birth and at 6 months of age, and weight (kg) and height (cm) at 8–9 years were obtained by review of outpatient electronic health records The health records were also searched for presence of any medical diagnosis potentially affecting growth, including asthma, attention deficit hyperactivity disorder, diabetes, malabsorption, and malignancy. Calculated variables included AR, BMI (kg/m2), and Z-scores for weight, length/height and BMI. Z-scores were calculated using means and SDs published for sex and estimated gestational age, based on the CDC growth charts from 2000 for ages 0 to < 20 years (https://www.cdc.gov/growthcharts/clinical_charts.htm). Growth status at 8–9 years of age was correlated with AR and with change in growth from birth to age 6 months.
Age at AR was calculated for each child as the nadir of a 2nd-degree polynomial regression of BMI on age [14]. Age at AR was calculated for all children in whom≥4 data points for BMI were available between 1 and 9 years of age. This study was approved by the Institutional Review Board, and parental consent was waived for this extended retrospective review of electronic medical records.
Data analyses
The relationship between change in weight from 0–6 months and final weight Z-score at 8–9 years was modeled using linear regression, adjusting for full term status at birth. Resulting corrected model and individual covariate F-tests determined significance. Average growth for BMI and weight Z-score from birth to 6 months were compared across the three feeding methods (breast, bottle, mixed) using one-way ANOVA followed by Tukey’s post-hoc tests. There was 80% power to detect a change in growth based on discharge feeding method and effect of preterm vs. full term birth, corresponding to a medium effect size of 0.6 SD, approximating a 0.7 point difference in weight Z-score and 1.2 point difference in BMI.
Comparison for each anthropometric measure between the full term and preterm infants was assessed using t-tests for independent samples. Age at AR was compared between children born full term and preterm using Student’s t test, and correlated with birth measurements (gestational age, weight, length, BMI, weight Z score) using Pearson correlation coefficients. All analyses were conducted in SAS version 9.4 and SPSS version 24 software, with Type I error controlled at 0.05. Figures were generated using both SPSS and R Statistical Software.
Results
Anthropometric data to 8–9 years of age were available for 175 children remaining in the military database, including 116 full term and 59 preterm births (Table 1A). Maternal characteristics included age, pre-pregnancy weight and BMI, gestational weight gain, race, and education. Mothers of preterm births were older than for full term births, and mothers of preterm births were less educated. There were no significant differences between mothers of preterm births and full term births infants in the incidence of preeclampsia, gestational diabetes mellitus, or 1-hour glucose. Among infant characteristics, 53% of preterm births and 44% of full term births were female. Among the preterm births, 22% were < 32 weeks gestation and < 1500 grams. The percent of small- and large-for-gestational age infants was similar among infants born preterm and full term.
Birth characteristics and longitudinal growth
Birth characteristics and longitudinal growth
All results shown as mean (SD) or as a percent. The number of children at 6 months and 8–9 years of age. (Table 1B) varies slightly for individual anthropometric measures due to missing data for that age. All significant differences in bold. BMI body mass index (kg/m2); SGA small for gestational age; LGA large for gestational age.
Among the complete cohort of 175 children, 165 records (94%) included information on feeding method at discharge from the birth hospital: 50% breast fed, 12% bottle fed, and 38% mixed breast and bottle. Also for all 175 children, 25% and 17% born preterm and full term, respectively, had been diagnosed with asthma, 9% and 6% with attention deficit hyperactivity disorder, 3% and 0% with diabetes mellitus, and 0% and 0% for malabsorption or malignancy.
Anthropometric data for preterm and full term births are summarized in Table 1B. Weight and weight Z-score are listed for birth, 6 months and 8–9 years of age. Length and length Z-score are listed for birth and age 6 months, and height and height Z-score are listed for 8–9 years of age. BMI data are included for birth and age 6 months; at 8–9 years of age, both BMI and BMI Z-score are included. As expected, weight, length and BMI are significantly less at birth for infants born preterm than for full term births. At 6 months of age, weight and length were both still significantly less for preterm than for full term births, but Z-scores for both weight and length were significantly greater for infants born preterm compared to full term. BMI at 6 months was similar among the preterm and full term births. At 8–9 years of age, children born both at term and preterm did not differ for any anthropometricparameter.
Age at AR could be calculated for the 150 children with both (a) at least four BMI measurements between the ages of 1 year and 8–9 years, and (b) an identifiable minimum BMI. A representative example in one child of serial BMI values and calculated AR is shown in Fig. 1. Average age at AR was 65 months for 102 full term and 64 months for 48 preterm children (p = 0.727). There was no correlation between age of AR and feeding regimen at discharge (p = 0.258) in either children born preterm (p = 0.154) or full term (p = 0.696)
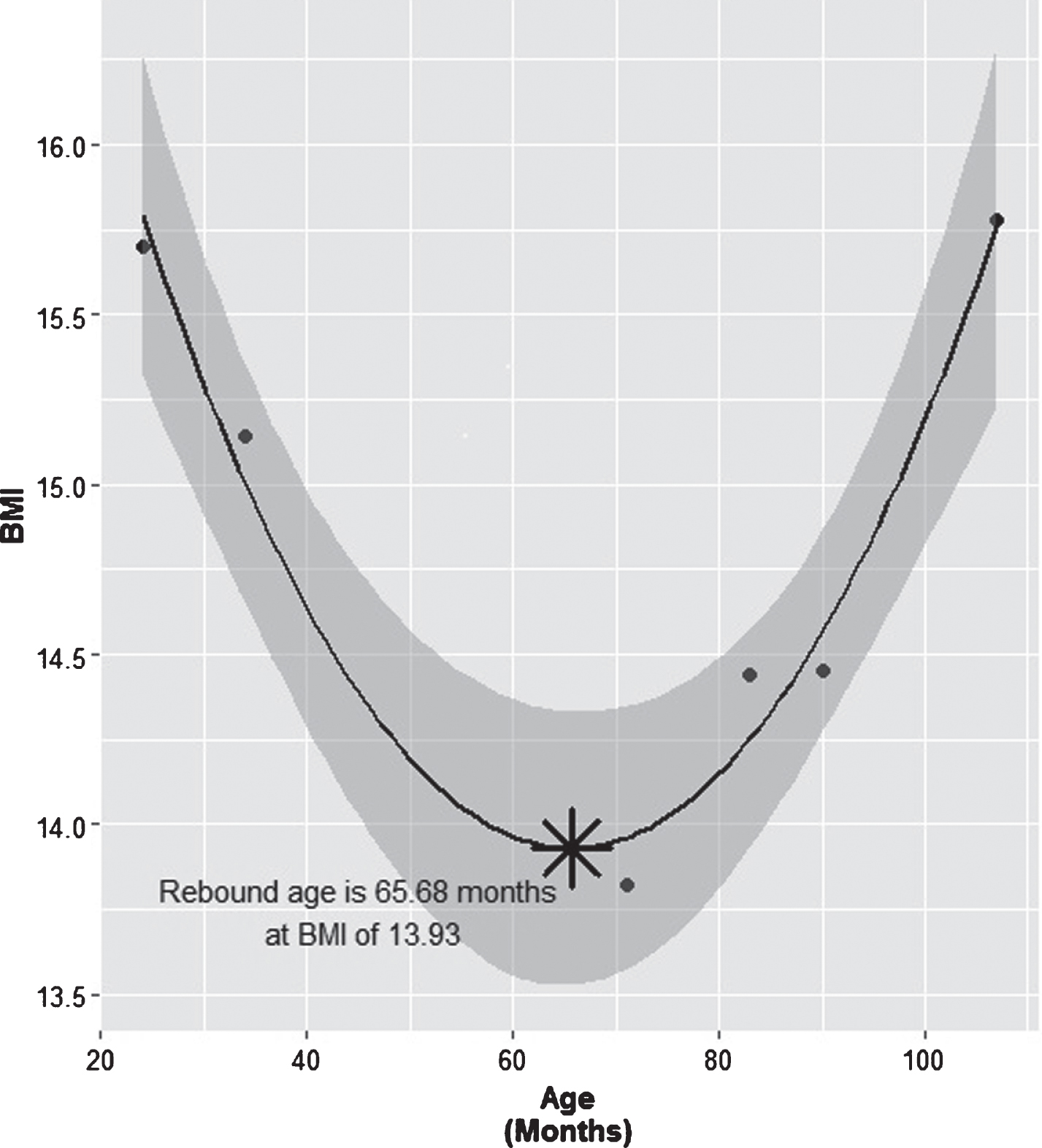
An example of longitudinal changes in body mass index (BMI) for calculating adiposity rebound (AR) in a 9-year-old child born at 37 weeks gestation. AR for this child occurred at 5.7 years of age. The shaded area represents the confidence intervals calculated from the quadratic model using the 6 measures of BMI available in this child beginning at 2 years of age.
Among the 121 children with both a calculated AR and anthropometric data at 8–9 years of age, there was a significant negative correlation between age of AR and BMI Z-score at 8–9 years of age (Fig. 2, r = – 0.685). These associations were similar in children born preterm (r = – 0.634) and full term (r = – 0.710). There was also a significant negative correlation between age at AR and weight, weight Z-score and BMI at 8–9 years in both the preterm and full term cohorts. The results were less consistent for height in that there was no association between age at AR and height or height Z-score at 8–9 years in children born full term but there was a significant negative correlation between age at AR and height at 8–9 years of age in children born preterm (Pearson r = 0.378, p = 0.019). Overall, there was no association between gestational age at birth and ageat AR.

Significant negative correlation between age at adiposity rebound (AR) and BMI Z-score at 8–9 years of age in 150 children, 102 born full term and 48 born preterm. The negative correlation is similar in children born full term compared to preterm births.
There was a significant correlation between change in weight from birth to 6 months and final weight Z-score at 8–9 years of age for all children (Fig. 3, p < 0.001). The slope of the relationship between weight Z-score at 8–9 years and change in weight from birth to age 6 months did not differ in children born preterm compared to full term, but weight Z-scores for change in weight were consistently higher in children born full term than preterm (p = 0.025). There was no correlation between change in BMI from birth to 6 months and BMI Z-score at 8–9 years (p = 0.407). Change in weight Z-score from birth to 6 months did not vary by feeding method (p = 0.838) but the change in BMI did vary by feeding method (p < 0.001). Specifically, BMI increased more at 6 months in the mixed feeding cohort than in the breastfed cohort (mean increase in BMI 5.23 vs. 4.36 m2, respectively, p < 0.001). There was no difference for preterm births in growth from birth to 6 months based on discharge feeding method, but for full term births there was a significantly greater increase in BMI with mixed than breast milk feeding (mean change 4.59 vs. 3.93, respectively, p = 0.022). At 8–9 years, children born preterm vs. full term differed significantly with respect to weight Z-score difference (p = 0.035) and BMI difference (p = 0.000). However, the effect of discharge feeding method did not differ between children born preterm and full term for either weight Z-score difference (p = 0.308) or BMI difference (p = 0.439).

Correlation between change in weight from birth to 6 months and weight Z-score at 8–9 years of age. For this analysis, data were available at 8–9 years for 153 children, 100 born full term and 53 born preterm.
This longitudinal study of growth from birth to 8–9 years of age includes several important observations, in particular the correlation of AR with longitudinal growth in children born preterm as well as born full term. Our results demonstrate that age at AR is directly correlated with growth at 8–9 years and that younger age at AR correlates with significantly higher BMI at 8–9 years of age. There was no difference in age of AR between children born preterm compared to full term. We also observed that greater weight gain from birth to age 6 months correlated with greater weight Z-score at 8–9 years both for children born preterm and full term. For all other anthropometric measures, there was no relationship between growth from birth to 6 months and growth status at 8–9 years, including change in BMI from birth to 6 months versus BMI Z-score at 8–9 years. At 8–9 years there was no significant difference for any anthropometric measure in children born at term versus preterm (Table 1B).
Our AR results are consistent with previous data in children born full term that early AR was associated with higher weight status, waist circumference, blood glucose and triglyceride levels, and with insulin resistance [12]. In children born full term, age at AR was a strong risk factor for adiposity and markers of cardiometabolic risk as assessed in early adolescence [15]. In young adults born full term, age at AR and BMI at AR were positively associated with adult BMI and waist circumference, and with cardiometabolic derangements including elevated HDL, triglycerides, fasting glucose, diabetes and hypertension [18]. Our results confirms this positive relationship between early AR and later BMI, and demonstrate that this relationship is already evident in middle childhood.
Our results are consistent with previous studies reporting a positive correlation between rapid early growth and later growth status. In children born full term, for example, studies have observed that rapid weight gain in the first few months of life correlated with a higher weight status in early childhood [10, 11]. In a large cohort study, infants who experienced rapid weight gain were four times more likely to be overweight at 3 years of age than infants who had not experienced rapid weight gain, and rapid early weight gain was the strongest predictor of overweight and obesity at age 3 years [19]. In children born preterm at < 36 weeks gestation, rapid weight gain in the first 3 months of life was positively associated with elevated body fat percentage, waist circumference, total cholesterol and low-density lipoprotein cholesterol levels in early adulthood [20].
Although our results for later growth status are generally consistent with previous results for effect of preterm birth compared to birth at term, the study methods and hence the results have varied significantly. One study of growth to 3–4 years of age compared the weights of infants born full term versus preterm and reported that despite differences in weight at birth, those differences were resolved by 3–4 months and remained similar to the final measurement at 3–4 years [21]. In a study of growth to 12 years in children born full term and preterm (≤34 weeks gestation and≤1800 grams), children born at term had greater height to age 8 years of age, by which time children born preterm had caught up with the children born at term [22]. As in our results (data not included), however, BMI was similar in preterm and full term births by age 4 years. In a study of growth to 18 years of age in a large cohort of extremely preterm infants born at < 28 weeks gestational age, children born preterm were lighter and shorter than children born full term through childhood to late adolescence [23]. Although the differences in weight Z scores gradually lessened over time, the differences in height persisted, with no evidence of catch-up between 2–18 years of age. BMI Z-scores were lower in the children born preterm at 2, 5, and 8 years of age, but were similar at 18 years. In a study of children born full term and preterm at≤34 weeks gestation, preterm infants had statistically significant lower weights, heights and BMI scores at 5 to 7 years in comparison to infants born full term [24]. However, these children born preterm did not have increased fat mass or visceral adiposity.
The primary strength of our study is a well-characterized birth cohort of full term and preterm infants followed longitudinally, of whom 175 children still remained in the military database at 8–9 years of age and for whom AR could be calculated in 150 children. There are, however, several limitations. There was significant attrition between hospital discharge (n = 1 093), 4 years (n = 661, 60%) and 8–9 years (n = 175, 16%). However, attrition from the military database was due primarily to discharge from active duty and not differentially related to any circumstances potentially affecting any growth outcome. Indeed, growth at 4 years of age among children no longer in the database at 8–9 years was similar to growth at 4 years for the 175 children still in the database at 8–9 years. Our study is also limited by a small number of very low-gestation preterm births, with only 13 children born at < 32 weeks gestation (Table 1A), thus yielding an insufficient very low gestation sample size for comparison with children born late preterm or full term. We were not able to assess the potential effect of comorbidities on growth due to the small number with a chronic illness; this was presumably due to low frequency in our cohort, although coding errors cannot be excluded. The measurements of weight and length/height were not standardized, but all were obtained by health care providers at a military care facility. For unknown reasons, the percent of preterm births in the available sample at 8–9 years was greater than at 4 years. Finally, these results in a military population may not be generalizable to a civilian population.
In summary, in children followed longitudinally to 8–9 years, younger age at AR correlates with higher BMI Z-score at 8–9 years in children born both term and preterm. Weight gain from birth to 6 months correlates with weight Z-score at 8–9 years, also in both term and preterm births. These results emphasize the importance of younger age at AR and more rapid early weight gain as indicators of later obesity. Future studies should focus on preterm infants born at younger gestational ages, for example < 32 and especially < 28 weeks gestation, for whom the risk for later obesity and cardiometabolic sequelae are greatest compared to children born late preterm or full term. Larger longitudinal studies extended from birth to adulthood are also needed. Although AR is not calculated in routine clinical practice, studies are needed to assess the potential clinical effectiveness of calculating AR in children as a valid marker for later morbidities and as a target for intervention.
Disclaimer
The views expressed in this manuscript are those of the authors and do not reflect the official policy of the Department of the Army/Navy/Air Force, Department of Defense, or U.S. Government.
Financial assistance
None.
Previously presented in part at Pediatric Academic Societies Annual Meeting, Toronto, CA, May 7, 2018.
Footnotes
Acknowledgments
The authors thank Chinenye Adimora, MD, Young Choi, MD, Jerri Curtis, MD, Leah Enright, MD, Jason Higginson, MD, and Alexander Holston, MD, for their participation in development of the original database of birth and discharge data (See references 16, 17).