
Abstract
BACKGROUND:
Stridor is one of the rare side effects of neonatal hypothermia treatment for hypoxic-ischemic encephalopathy. We aimed to describe the clinical characteristics of the infants who underwent whole-body hypothermia and developed stridor.
METHODS:
We reviewed the medical records of 171 infants with moderate or severe hypoxic-ischemic encephalopathy who underwent hypothermia therapy. Demographics, as well as clinical characteristics, were documented.
RESULTS:
A total of 18 infants developed transient stridor out of 171 infants who underwent whole-body hypothermia (10.5%). The stridor was transient and resolved in all infants. All infants with stridor received treatment with one or more of the following: racemic epinephrine, dexamethasone, positive pressure ventilation and/or heliox. Two infants required otorhinolaryngologist (ENT) evaluation due to persistent and severe symptoms, of whom one was found to have left vocal cord paresis that improved with time.
CONCLUSION:
Stridor is a transient complication associated with hypoxic-ischemic encephalopathy and whole-body hypothermia in neonates. The exact mechanism is unclear and most likely multifactorial. ENT evaluation is recommended in the presence of prolonged symptoms or significant respiratory distress.
Introduction
Therapeutic hypothermia (TH) in moderate or severe hypoxic-ischemic encephalopathy (HIE) decreases mortality as well as adverse neurodevelopmental outcomes in term and near-term infants. The committee of fetus and newborn has recommended well-defined criteria for initiation of cooling in these infants [1]. Complications from the cooling intervention have been described, including cardiac arrhythmia, subcutaneous fat necrosis, electrolyte imbalance, and stridor; however, the benefits of hypothermia treatment outweigh risks in these infants [2].
Methods
We performed a retrospective chart review of electronic medical records of all infants admitted to a level-four regional neonatal intensive care unit, with the diagnosis of moderate or severe HIE and who underwent whole-body hypothermia (WBH) from January 2012 to October 2018. The University at Buffalo institutional board review board approved the study protocol (Approval number: 3091).
Infants underwent WBH if they met the eligibility criteria for cooling well established by the Committee of Fetus and Newborn [1]. Cooling was initiated by 6 hours of age, and a target temperature of 33.5°C maintained for 72 hours in all infants. All infants had core temperature monitored by an esophageal probe. Infants were rewarmed gradually by 0.5°C per hour until core body temperature reached 36.5°C.
Infants who did not receive WBH treatment or those that died during WBH were excluded from the study. The majority of infants received a spectrum of respiratory support, including nasal cannula support, non-invasive positive pressure ventilation, or mechanical ventilation based on the respiratory status during hospitalization. Gas flow provided in these devices was both humidified and rewarmed to 37 °C.
Using the electronic medical record system, we reviewed all infants with the ICD-10 code diagnosis of acquired stridor (R06.1). The determination of stridor was made by physical examination performed by the advanced pediatric provider, then confirmed by the neonatologist -attending or neonatal fellow. Stridor was treated with one or combination of the following: racemic epinephrine (0.5 ml) per dose, dexamethasone (0.25 mg/kg/dose), non-invasive positive pressure ventilation and/or heliox gas. Attempts of intubation were analyzed as part of data collection. The stylet was routinely used during the intubation procedure. Otorhinolaryngologist (ENT) evaluation was performed if infants had prolonged stridor or significant signs of respiratory distress (severe subcostal and intercostal retractions, failed medical and non-invasive management, symptoms, and signs of impending respiratory failure).
Results
Eighteen infants (18/171, 10.5%) who underwent cooling for moderate or severe hypoxic-ischemic encephalopathy developed stridor during hospitalization. Perinatal, clinical, and relevant laboratory characteristics of all infants with stridor are shown in Table 1. Table 2 shows the stridor clinical course characteristics and the type, frequency and duration of interventions provided to each infant. The severity of stridor in all infants increased with agitation. The onset of stridor generally occurred during the cooling/rewarming phase in non-intubated infants and immediately following extubation in intubated infants. In all infants, stridor was transient (median duration: 2 days; IQR:±1 day) and resolved over time. Sixteen infants (16/18, 88%) received racemic epinephrine, and 11 infants (11/18, 61%) received dexamethasone therapy for stridor. Fourteen infants (77%) required positive pressure ventilation either by non-invasive positive pressure ventilation or high flow nasal cannula at a flow rate of≥4 L/min. The majority of infants who developed stridor had moderate HIE (17/18, 95%), and only one infant had severe HIE. Seven infants (7/18, 38%) had abnormal magnetic resonance imaging (MRI) of the brain. Two infants (2/18,11%) with stridor had multiple attempts of intubation. Significant hypokalemia (≤3 mEq/L) developed in nine infants (9/18, 50%); and hypocalcemia (<8.5 mg/dl) in five infants (5/18, 28%). Potassium and calcium supplementation were adjusted in parenteral nutrition to correct electrolyte abnormalities.
Perinatal, clinical, and laboratory characteristics of infants who developed stridor following hypoxic-ischemic encephalopathy and whole-body hypothermia
Perinatal, clinical, and laboratory characteristics of infants who developed stridor following hypoxic-ischemic encephalopathy and whole-body hypothermia
GA: gestational age, VAVD: vacuum-assisted vaginal delivery, CS: cesarean section, SVD: spontaneous vaginal delivery, HIE: hypoxic-ischemic encephalopathy, K: potassium, Ca: calcium.
Stridor characteristics, clinical course, and management
NIPPV: non-invasive positive pressure ventilation, ENT: Otolaryngologist.
Four infants developed stridor (4/18,22%) were never intubated. Two infants (ID #7 and 18) required ENT evaluation due to prolong and significant stridor; Infant #7 had severe HIE based on the clinical examination and magnetic resonance findings suggestive of ischemia affecting the frontal lobe. ENT airway evaluation suggested intact vocal cords. Stridor resolved at the outpatient follow-up at one month of age. Infant #18 had moderate HIE and unremarkable brain MRI. He never required intubation, and the delivery was uncomplicated. ENT examination revealed unilateral vocal cord paresis, which resolved over time. The course of stridor was transient in all infants.
There is a lack of data about the occurrence of stridor in HIE infants who underwent WBH. The general adoption of neonatal hypothermia as the standard of care in moderate and severe HIE revealed few side effects that have not been reported in the initial randomized trials. The literature evidence about stridor occurrence in HIE and therapeutic hypothermia is limited and mainly based on case series and safety reports; Orme, et al. [3]. reported an incidence of 9.6% (5/51) in their practice, in reply to Orme observation L. Smit reported a lower incidence of 5% (6/120) in their unit, out of the 11 infants in both observations; only one infant underwent ENT evaluation. All 11 infants had an uncomplicated course of recovery regarding their stridor course. A similar incidence of 9.3% (7/75) was reported in another case series done by Redondo, et al. [4]. In the multicenter randomized safety outcomes study to compare the incidence of adverse outcomes that could be related to TH intervention, stridor developed in 9 infants out of 31 (29%) in the TH group vs. one infant out of 31 in the non-intervention group (3%) (p-value<0.01). The authors suggested the use of humidified gas at a lower temperature of 34° in the intervention arm as a possible reason for this higher incidence. The stridor course was uneventful in the nine reported infants, and none required invasive interventions [5].
In our relatively large size cohort, we reviewed all cases of HIE who underwent WHB and developed stridor. Stridor course was uncomplicated and resolved in all infants with no significant consequences. The preference for either using racemic epinephrine or dexamethasone or both was based on the evaluation performed by clinicians. The precise mechanism for stridor in infants with HIE who underwent WBH is unclear and most likely multifactorial. The fact that four infants developed stridor in spite of never being intubated suggests that mechanisms other than a traumatic intubation procedure might be involved.
Derived from other relatively small studies and case reports; suggested mechanisms may include, brain injury resulting in neuronal dysfunction of the respiratory control center or the nucleus of the vagus nerve has been postulated, especially in the presence of lesions or increased ICP that can result in neuronal compression mainly in the brainstem or frontal cortex [6 –8]. Electrolyte imbalances such as hypocalcemia or hypokalemia that occurs during cooling, due to electrolytes shift from the extracellular to the intracellular space, can potentially result in laryngospasm and muscle weakness, respectively [9 –11]. In addition to the above factors, hypothermia and temperature fluctuations can result in glottic closure reflex and edema of the vocal cords and the surrounding tissue leading to significant airway narrowing [12, 13]. The possible suggested pathophysiology of stridor in infants with HIE is illustrated in Fig. 1 [6 –13]. Based on our observation and the clinical outcome we observed in this report, we suggest an evaluation approach, as shown in Fig. 2.
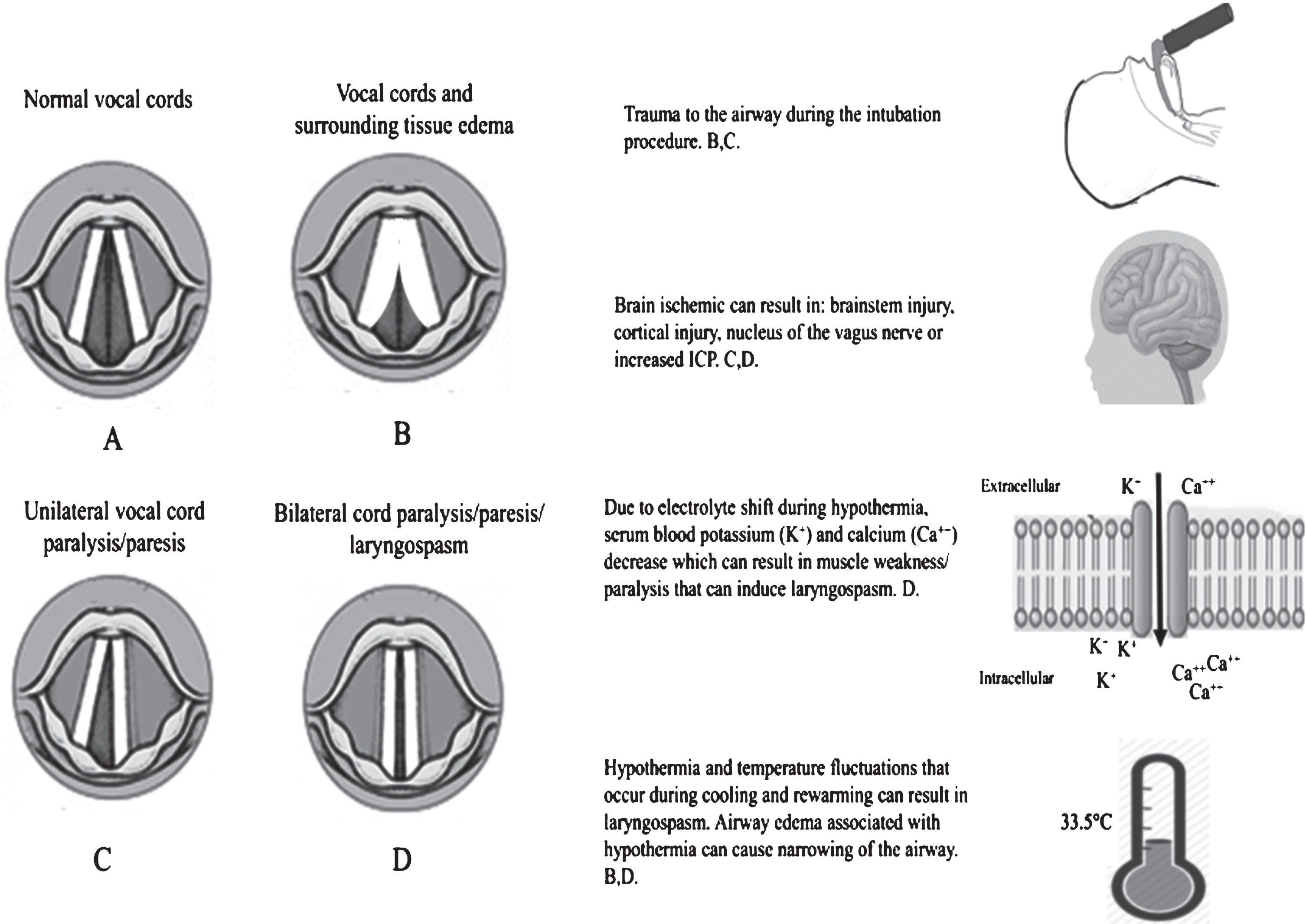
Suggested mechanisms of stridor in infants with moderate or severe hypoxic-ischemic Encephalopathy who underwent cooling. ICP: Intracranial pressure.
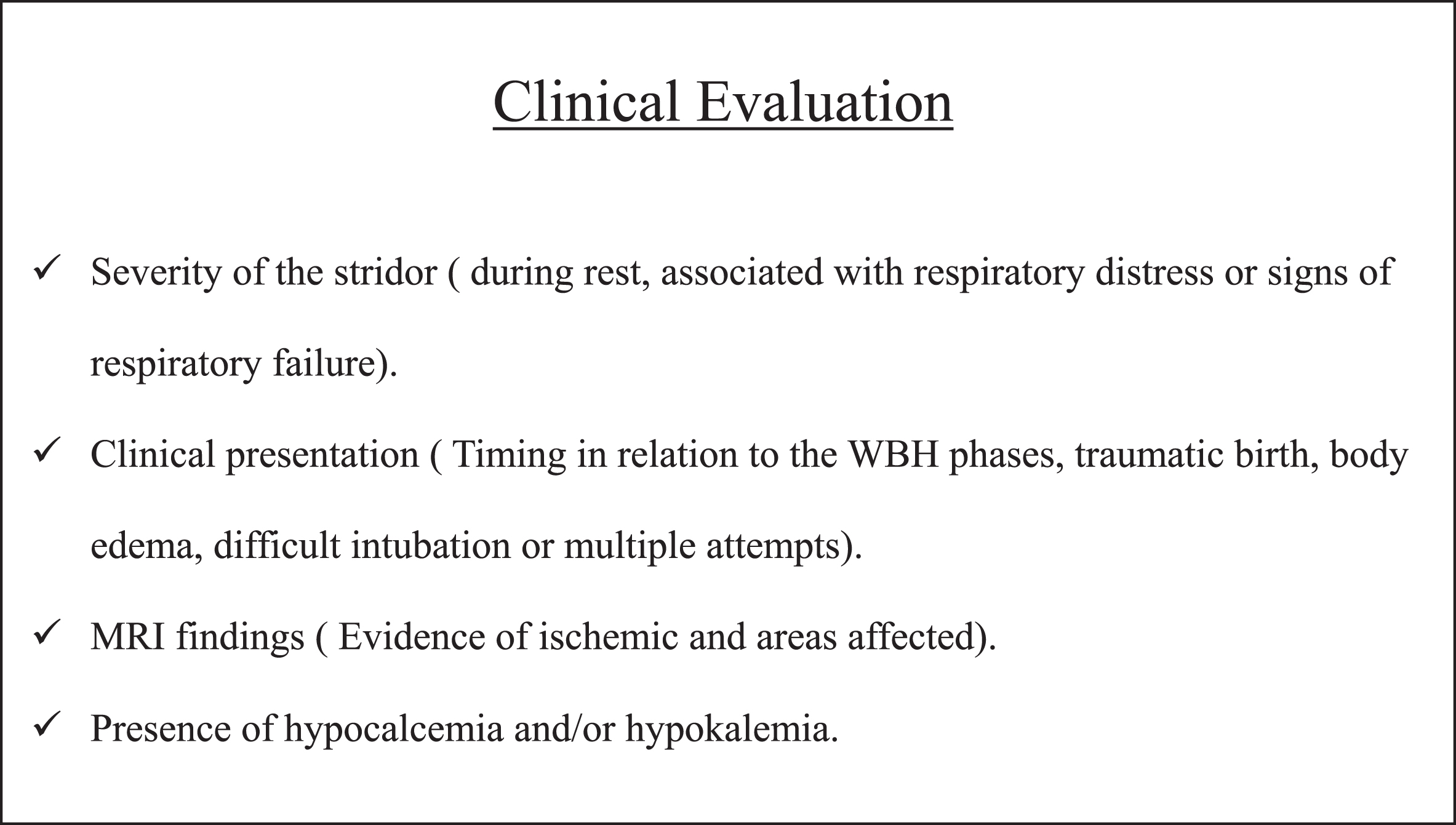
Suggested Clinical evaluation of infants with stridor following hypoxic-ischemic encephalopathy and whole-body hypothermia. WBH: whole-body hypothermia. MRI: Magnetic resonance imaging. ENT: Otolaryngologist.
This study is limited by the retrospective nature and the absence of a standardized evaluation and management protocol for the assessment of stridor in our cohort. ENT evaluation was not performed on all infants to assess either vocal cords edema or abnormal cord movement.
In this largest cohort of infants with stridor associated with hypothermia for hypoxic-ischemic encephalopathy, we put forward that stridor in infants with hypoxic-ischemic encephalopathy who underwent whole-body hypothermia is mostly a transient associated side effect. The exact mechanism is unclear and most likely multifactorial. Several hypotheses exist to explain the possible pathophysiology. ENT evaluation is recommended in the presence of prolonged symptoms or significant distress.
Declaration of conflicting interests
The authors declare no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Footnotes
Acknowledgments
None.