
Abstract
Central diabetes insipidus (CDI) may occur in the setting of intracranial abnormalities that affect the hypothalamus-pituitary system. It occurs rarely in neonates, especially in the premature population, and represents a challenging disease process to treat pharmacologically. Little is known regarding the treatment options in premature infants, including dose and route of administration of intravenous desmopressin (DDAVP). We present a case of a late premature male infant with gastroschisis and septo-optic dysplasia who developed transient CDI. He was treated with intravenous DDAVP but required frequent laboratory monitoring and a multidisciplinary approach, and ultimately his CDI resolved. Although there are minimal guidelines regarding the appropriate formulation and dosage of DDAVP for management of CDI in infants, we initiated the lowest dose available and titrated the medication based on close monitoring of urine output and serum sodium levels in order to successfully treat his transient CDI.
Introduction
Central diabetes insipidus (CDI) is a rare disease process, secondary to impaired production or release of vasopressin [1]. It has been described in infants with septo-optic dysplasia (SOD), a disorder of two or more features including midline neuro-radiologic abnormalities such as absent septum pellucidum, agenesis of the corpus callosum, optic nerve hypoplasia, and pituitary hypoplasia [1–3]. Interestingly, SOD has been linked with gastroschisis [3]. Gastroschisis was presumed to occur as an isolated defect; however, recent studies suggest that it may be associated with malformations in up to one-third of cases, and central nervous system anomalies in 8% of infants [3]. Reported cases of infants with gastroschisis and SOD postulate both to be the result of an early vascular interruption sequence [4]. These infants are at risk for CDI, which can be challenging to manage. Multiple agents have been used with limited evidence including vasopressin, thiazide diuretics and synthetic desmopressin (DDAVP)— the latter of which comes in various preparations with different levels of potency and half-lives. Furthermore, there are no recommended dosing guidelines or established safety profiles for neonates [1]. We present a case of a late-premature infant with gastroschisis and SOD who developed transient CDI ultimately managed with intravenous desmopressin.
Case report
A male infant was born via Cesarean section at 34 weeks gestation to a 20-year-old primigravid Hispanic white woman. The pregnancy was notable for fetal gastroschisis, absent cavum septum pellucidum, and intrauterine growth restriction. The mother declined amniocentesis for cytogenetics or microarray. Birth weight was 2660 grams (77th percentile), head circumference 31.5 centimeters (51st percentile). At birth, a replogle was placed and bowel contents were placed into a silo by the surgical team. His exam was remarkable for partially reduced right-sided intestinal contents, facial dysmorphism included inverted triangular-shaped face, low-set ears, and a depressed nasal bridge. He was diffusely hypertonic with multiple beats of clonus in his lower extremities. He had normal preterm male genitalia.
His initial hospital course was notable for profound hypoglycemia requiring an initial glucose infusion rate nearing 12 mg/kg/min during the first 12 hours of life. He was hyponatremic (sodium nadir of 119 mmol/L) by 36 hours of life and responded to fluid restriction and sodium correction with hypertonic saline. A brain MRI showed absence of the cavum pellucidum, a thin corpus callosum, small optic nerves, and a normal pituitary gland (Fig. 1A– B). An ophthalmology exam confirmed bilateral optic nerve hypoplasia. His echocardiogram was normal. He developed multiple intestinal perforations requiring resection of 25 centimeters of bowel including his ileocecal valve. The family repeatedly declined genetic testing.
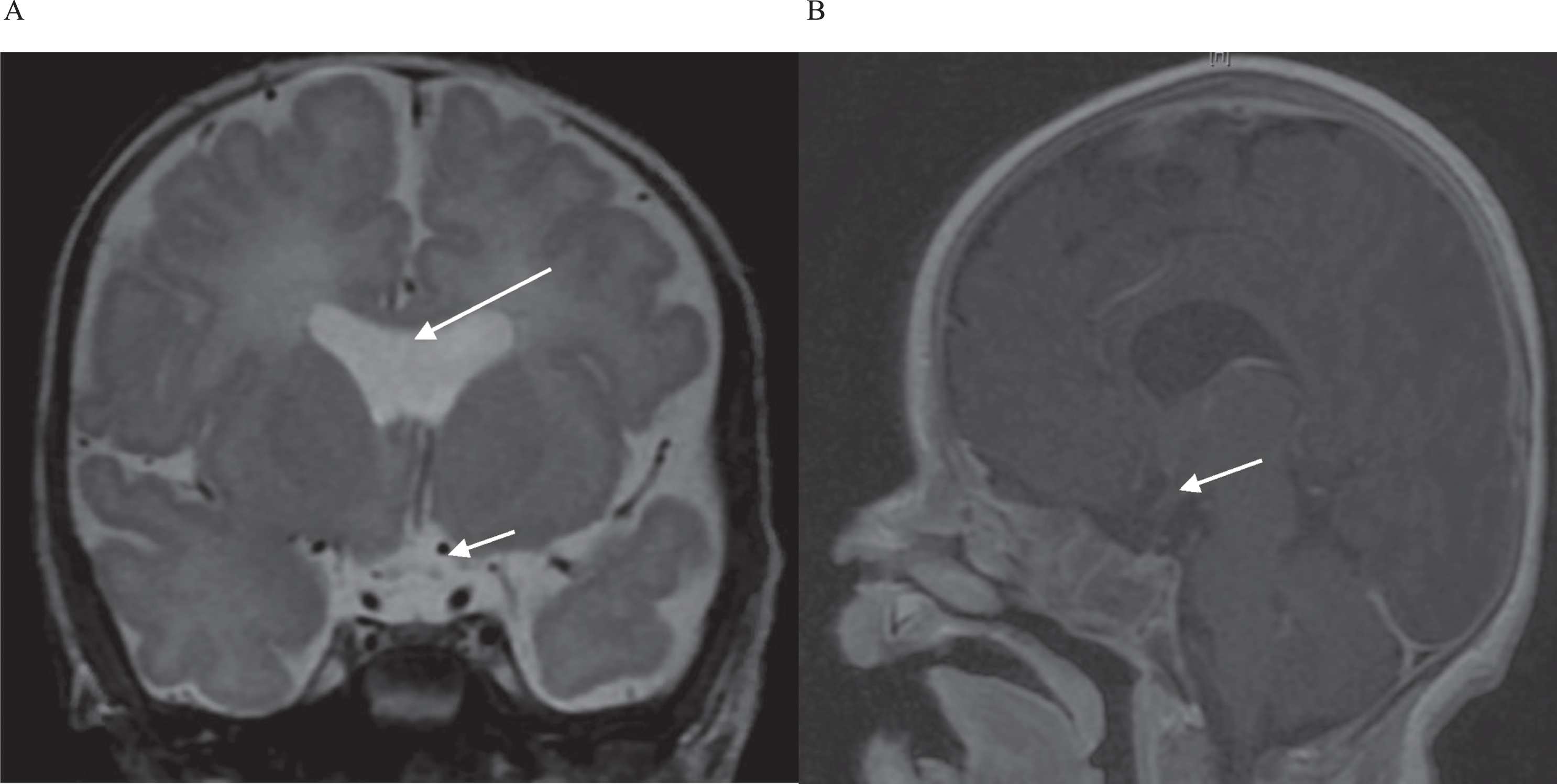
A– B. Selected images from brain magnetic resonance imaging (MRI) without contrast in our patient. A. Coronal T2 image with absence of the cavum pellucidum (long white arrow) and hypoplastic-appearing optic nerves (short white arrow). B. Sagittal T1 flair image demonstrating normal pituitary gland and pituitary stalk (white arrow).
Given the hyponatremia and hypoglycemia, an abnormal hypothalamic-pituitary-adrenal axis and cerebral salt wasting were initially suspected; however, his electrolytes and urine studies did not support either clinical picture. He underwent an ACTH stimulation test, which was normal. His thyroid, growth hormone, luteinizing hormone and follicle-stimulating hormone levels were unremarkable.
On day of life 8, he developed polyuria with urine output increasing to >10 ml/kg/hour and hypernatremia with a 16-point rise in his sodium. Laboratory analysis supported the diagnosis of CDI with an elevated serum sodium 158 mmol/L, urine specific gravity <1.005, serum osmolality 304 mOsm/kg, urine osmolality 187 mOsm/kg and urine sodium 20 mmol/L. He remained euglycemic with normal potassium and creatinine levels. His neurologic exam remained at his baseline. He was maintained on total parenteral nutrition with a fluid requirement of 150 ml/kg/day. His urine output was replaced 1:1 if it exceeded >4 ml/kg/hour with dextrose 5% + 1/4 normal saline. Vasopressin infusion was not initiated given risk of compromised intestinal perfusion. For one week, he required total fluid requirement of almost 300 ml/kg/day to maintain a serum sodium between 140– 150 mmol/L. On day of life 24 in the setting of episodic hypernatremia despite fluid repletion, he was started on intravenous desmopressin at an initial dose of 0.05μg/daily. Over the next three days, his sodium levels and urine output were followed closely and ultimately normalized. He was titrated to a dose of intravenous desmopressin 0.03μg every 12 hours with stable sodium levels and urine output, and total fluid requirements were decreased to 130 ml/kg/day. On day of life 50, he was incidentally hyponatremic down to 125 mmol/L, and desmopressin was held. This acute hyponatremia was attributed to potential excess salt loss from the replogle output with inadequate replacement compounded by desmopressin. Serum sodium levels and urine output remained normal, so DDAVP was never restarted. He underwent bowel reanastomosis and gastrostomy tube placement on day of life 83 and was eventually transferred to a rehabilitation center.
SOD is a heterogenous clinical triad present in only 1 per 10,000 births with a higher incidence in babies of young mothers aged 20 to 24 years [4]. The majority of cases are often classified as an isolated cerebral anomaly with no identifiable genetic cause [5]. Gastroschisis has an estimated prevalence of 2 to 5 per 10,000 live birth births with an increasing incidence in younger mothers aged less than 20 years, which has been confirmed in multiple surveillance studies [3, 6]. Although the largest increase in incidence has been observed in non-Hispanic black mothers over the past three decades, the incidence in Hispanic white mothers remains the highest [6, 7]. Although there are no identified genetic causes for this defect as well, several cases have reported the association among gastroschisis, SOD and panhypopituitarism. Although this infant’s various pituitary-related hormone levels were normal, the diagnosis of CDI was evidenced by his hypernatremia, polyuria and low urine osmolality. Garvin et al. presented a case of an infant with gastroschisis with SOD with adrenal insufficiency manifesting as shock, hypothyroidism and growth hormone deficiency, but without mention of CDI [8]. Another report of an infant with gastroschisis and SOD with hypothyroidism and CDI, noted a sodium peak of only 148 mmol/L and treatment included levothyroxine [9]. The same authors presented a literature review of three other cases of infants with gastroschisis, SOD and CDI. One required intramuscular vasopressin followed by management with intra-nasal DDAVP, while another infant had schizencephaly and panhypopituitarism without mention of management of CDI [9].
Another treatment option includes enteral thiazide diuretics, which are used in nephrogenic DI, combined with a low renal solute load formula. A few series have reported effective treatment of CDI in infants with minimal adverse effects. Ultimately these infants required eventual transition to DDAVP around six months of age when they were no longer drinking only breastmilk or formula [10, 11]. However, because our patient could not feed for a prolonged period of time following his intestinal perforation, this was not a pharmacologic option for him.
Minimal data exist regarding the appropriate dose and route of administration of DDAVP in infants who consume their calories exclusively in the form of breastmilk or formula and normally produce dilute and high amounts of urine. Coupled with immature renal function, premature infants are prone to water intoxication and hyponatremia if fixed antidiuresis is achieved using DDAVP, which has a half-life of 12– 24 hours [11]. Vasopressin can reduce intestinal blood flow and induce hypertension, both of which would have been detrimental in this patient. Van der Kaay et al. reported a case of a preterm infant with post-hemorrhagic hydrocephalus with CDI, treated with intranasal DDAVP 0.2μg, resulting in oliguria and anuria and a 25-point drop in sodium levels within 15 hours [12]. Atasay et al. reported a similar infant successfully treated with oral DDAVP 2.5μg/kg twice a day [13]. Therapeutic options available to our team included free water replacement, which required reliable intravenous access or intravenous DDAVP (intranasal formulation was unavailable) [2]. We ultimately initiated a low dose of intravenous DDAVP and followed urine output and sodium levels closely to determine an ideal dose and interval using the guidelines outlined in Table 1. In our patient at an effective dose of 0.024μg/kg/daily divided every 12 hours, the urine output decreased about two hours after administration with the duration of action lasting between 8 to 12 hours until break-through increased urine output occurred. His sodium levels were maintained between 140 and 150 mmol/L. The drug was subsequently stopped in the setting of incidental hyponatremia one month later, and he did not require it again suggesting a transient form of CDI. Transient CDI typically occurs in patients who have undergone a neurosurgical intervention (e.g. surgery by transsphenoidal approach) that causes a temporary dysfunction of antidiuretic hormone-producing neurons and often resolves after a few days [14]. On rare occasions, CDI has gone into remission spontaneously despite a persistent deficiency of vasopressin with no clear physiologic explanation such as in our patient [15]. Despite these reported cases, it is still possible that this disorder reoccurs in the future leading to potentially harmful complications, thus highlighting the need for appropriate and vigilant follow-up with a pediatric endocrinologist moving forward.
Initiation of intravenous DDAVP dosage and titration guidelines used in our patient
Initiation of intravenous DDAVP dosage and titration guidelines used in our patient
The multiple presenting anomalies in our patient made us vigilant about the potential risk for panhypopituitarism, thus when he developed polyuria with hypernatremia, the diagnosis of CDI was quickly made. To our knowledge, this is the first report in which intravenous DDAVP was used to manage CDI in a premature infant with gastroschisis. This latter anomaly posed multiple challenges as he remained unable to feed enterally, limiting our options for drug delivery and compounded by adverse effect of hyponatremia as he was losing sodium from his gastrointestinal tract. However, with close lab monitoring and careful urine output measurement and a multidisciplinary approach that included Endocrine, Neonatology and Surgery, we were able to control his transient CDI with DDAVP. This case represents the importance of anticipating and assessing for pituitary abnormalities in this population of infants presenting with multiple anomalies that could lead to earlier diagnosis and treatment as well as the reassessments during the management of CDI, which may be a transient presentation in infants.
Conflicts of interest
Dr. Kim and Dr. Towers have no conflicts of interest or financial ties to disclose.
Footnotes
Acknowledgments
We are grateful to the many families we have the privilege of caring for in the neonatal intensive care unit at our institution who have taught us greatly.