
Abstract
BACKGROUND:
Diabetes insipidus (DI) is a disease resulting from defects in the arginine vasopressin system responsible for regulating body water homeostasis. It is characterized by polyuria with increased serum osmolality and sodium and can result from congenital or acquired disorders.
CLINICAL PRESENTATION:
A baby was admitted to NICU for extreme prematurity (25 weeks gestation), extreme low birth weight (900 grams) and respiratory distress. He received one dose of Surfactant and was ventilated using high frequency jet ventilation for development of pulmonary interstitial emphysema. After nine days, he still required high settings with development of early chronic lung changes in the form of atelectasis. Therefore, he was started on a course of dexamethasone following the DART study protocol (Dexamethasone: A Randomized Trial). However, after six days (cumulative dose of 0.75 mg/kg/day) he developed polyuria (7.4 ml/kg/h) with increased serum sodium (150 mmol/L) and osmolality (348 mmol/L). He lost 85 grams of his weight in 24 hours, which represented a 9.8 %weight loss. The findings were suggestive of DI and given there were no apparent causes other than dexamethasone, it was discontinued. Over the following 48 hours, polyuria and hypernatremia gradually resolved, reaching 3.5 ml/kg/h, and 140 mmol/L respectively.
CONCLUSION:
The use of dexamethasone is not an uncommon practice in tertiary care neonatal units. To our knowledge, our case is the first report of neonatal DI secondary to the use of dexamethasone. We recommend closely monitoring urine output and serum electrolytes in preterm infants receiving dexamethasone.
Introduction
Diabetes insipidus (DI) is a disease resulting from defects in the arginine vasopressin (AVP) system responsible for regulating body water homeostasis. It is characterized by hypotonic polyuria with secondary dehydration and increased serum osmolality and sodium. Synthesized in the hypothalamus and stored in the posterior pituitary gland, AVP is released in response to increased serum osmolality or hypotension. It acts on the renal collecting ducts to enhance reabsorption of water, concentrates the urine, decreases the urine output, and restores serum osmolality and blood pressure. A defect in secretion of AVP is classified as central DI and an inappropriate kidney response to AVP is classified as nephrogenic DI. Both can result from congenital or acquired disorders [1].
We present a neonate who developed DI secondary to the use of dexamethasone to facilitate weaning off mechanical ventilation.
Clinical report
A baby boy was born at 25 weeks gestation to a 39 years old G1P0 mother. Parents were non-con-sanguineous and family history was unremarkable. Pregnancy was uneventful. The baby was delivered via vaginal delivery after spontaneous onset of preterm labor and rupture of membranes for less than an hour. The mother was not given any steroids, and one dose of Penicillin G was given less than 4 hours before delivery.
Baby was born cephalic and required intubation in the delivery room for poor respiratory effort. He was admitted to NICU for extreme prematurity, extreme low birth weight (900 grams), respiratory distress and potential risk for sepsis. He had no dysmorphic features and was appropriate for gestational age.
He was hypotensive on admission requiring dop-amine infusion for about 24 hours. Given the high risk of sepsis, he received a 5 days course of ampicillin and gentamycin. He also suffered from a short period of oliguria which responded to one dose of aminophylline. An abdominal ultrasound ruled out renal anomalies. His head ultrasound showed a left sided grade I intraventricular hemorrhage (IVH) which was resolving on serial scans with no structural brain anomalies. Newborn metabolic screen was reported normal, which screens for congenital adrenal insufficiency.
The baby received one dose of Surfactant, but high oxygen and ventilatory requirements persisted with development of pulmonary interstitial emphysema (PIE) which required use of high frequency jet ventilation (HFJV). After nine days, he still required high settings and his chest X-ray showed signs of early chronic lung changes in the form of atelectasis and worsening PIE. Given the worsening chest X-ray, PIE and respiratory status, he was started on a course of dexamethasone following the DART study protocol (Dexamethasone: A Randomized Trial) starting at a dose of 0.15 mg/kg/day and titrating over a course of 10 days [2].
However, after six days of dexamethasone (cumulative dose of 0.75 mg/kg/day) the baby developed polyuria with increased serum sodium and osmolality. Urine output increased from 4 ml/kg/h to 7.4 ml/kg/h, serum osmolality increased to from 282 mmol/L to 348 mmol/L and serum sodium increased from 141 mmol/L to 150 mmol/L. Serum creatinine was only slightly elevated (71μmol/L) and serum potassium and glucose were both normal. He lost 85 grams of his weight in 24 hours, decreasing from 870 g to 785 g which represented a 9.8 %weight loss. The findings were suggestive of DI and given there were no obvious or apparent causes for DI, dexamethasone was thought to contribute to the development of the findings and was therefore discontinued.
Over the following 48 hours, polyuria and hypernatremia gradually resolved. Urine output decreased to 4 ml/kg/h then 3.5 ml/kg/h, and serum sodium decreased to 147 mmol/L then 140 mmol/L.
Discussion
Diabetes insipidus can either be primary, or secondary to multiple underlying causes, including drugs [1]. In our case, DI was likely secondary to use of dexamethasone, where symptoms rapidly resolved after cessation of the drug.
Our baby had a normal newborn metabolic screen, ruling out congenital adrenal insufficiency. His abdominal ultrasound excluded any renal anomalies that could have contributed to his symptoms. IVH was only grade I and was resolving on subsequent head scans. There was no hydrocephalus, nor were there any midline defects detected that could lead to DI. He had neither dysmorphic features nor a positive family history to suggest congenital genetic or metabolic diseases. As urine output and serum osmolality normalized within a short period after stopping dexamethasone, it was impractical and unnecessary to pursue a desmopressin challenge test.
The effect of glucocorticoids (GC) on water regulation has been studied in both animal models [3–8] and humans [9, 10]. These studies suggested that the mechanism of DI secondary to GC could be both central as well as peripheral. Centrally, GC act via negative feedback inhibition to decrease the release of corticotropin releasing hormone (CRH) which is an AVP secretagogue. Also, GC directly attenuate the secretion of AVP in response to changes in osmolality and blood pressure. Peripherally, GC cause a state of AVP resistance in the kidneys by interfering with the AVP V2 receptor signaling, causing a downregulation in expression of aquaporins (AQPs), which are responsible for water reabsorption in the renal collecting duct [11] (Fig. 1).
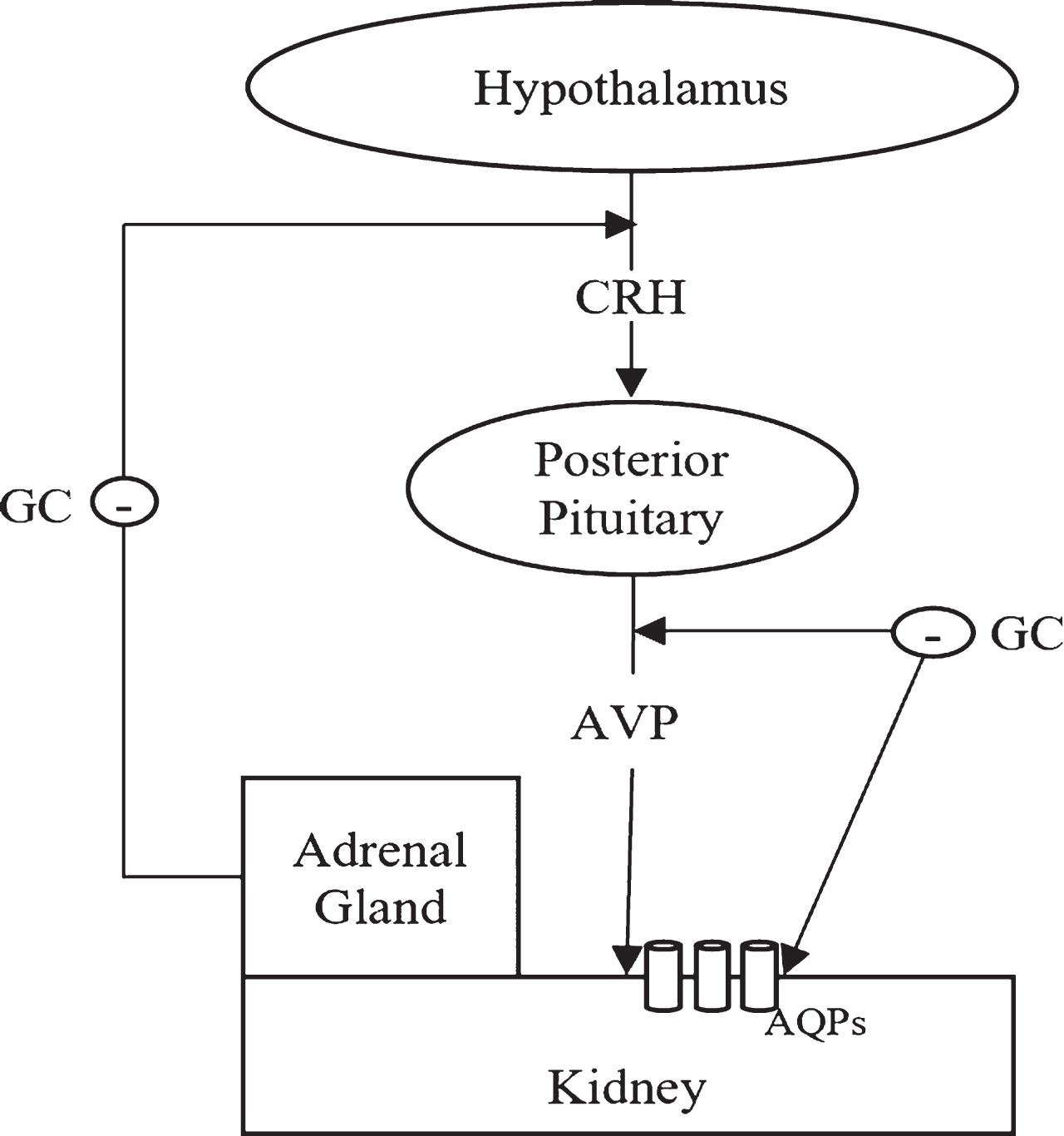
Effects of glucocorticoids on water regulation.
Although several animal studies have reported DI secondary to GC [12–14], there have been relatively few case reports of DI secondary to GC in humans and none in neonates. In 1991, Ohta et al. reported a 37 years old man treated with dexamethasone for malignant lymphoma [15]. In 1997, Chin et al. reported DI in a 71 years old woman suffering from bronchogenic carcinoma, who received hydrocortisone for bronchospasm, and dexamethasone for perilesional edema [11]. Another 40 years old female was reported in 2012 by Patel et al. who was given dexamethasone for hypotension secondary to adrenal insufficiency [16]. There are two case reports of DI secondary to GC in the pediatric population. One was a 15 years old girl with brain tumor reported by Knudsen et al. in 1995 who got dexamethasone during endotracheal intubation for general anesthesia, suggesting that DI can arise even after a short exposure to dexamethasone [17]. The other is the youngest reported case of DI, by Puri et al. in 2011, a two months old infant who suffered from septo-optic dysplasia (SOD) and developed DI after receiving a stress dose of hydrocortisone [18].
The use of dexamethasone is not an uncommon practice in tertiary care neonatal units. To our knowledge, our case is the first report of neonatal DI secondary to the use of dexamethasone. We recommend closely monitoring urine output and serum electrolytes in preterm infants receiving dexame-thasone.
Disclosure statement
The authors declare no conflict of interest, financial or otherwise.