
Abstract
BACKGROUND:
Delayed cord clamping (DCC) is the recommended strategy in neonates not requiring resuscitation, but umbilical cord milking (UCM) can also be used in term babies. DCC has been found to offer advantages more than just placental transfusion.
OBJECTIVE:
To compare the neonatal outcomes of DCC and UCM at birth in vigorous neonates ≥35 weeks born via cesarean section.
METHODS:
We included all vigorous neonates born ≥35 weeks of gestation through the cesarean section in this open-label randomized controlled trial. They were randomized into Group-A (DCC-cord was clamped 60 s after birth) or Group B(UCM). For neonates in Group B, the intact cord was milked at 25 cm from the stump 3 times towards the neonate and then clamped. The primary outcome was hematocrit at 72 h of life. Secondary outcomes were serum ferritin between 6 and 10 weeks of life, serum bilirubin at 72 h of life, need and duration of phototherapy, respiratory distress, hypoglycemia, hypotension, and sepsis.
RESULTS:
Baseline characteristics were similar in both the groups. The mean hematocrit at 72 h was more in the DCC group compared to the UCM group [(55.60±4.50) vs (53.89±4.44), MD (95% CI) = 1.71 (0.26, 3.16); p = 0.021]. There was no significant difference in median serum ferritin between the groups [102.88(84.67–173.24) vs 137.93(85.15–230.40); p = 0.173]. There was no significant difference in clinical outcomes.
CONCLUSION:
In neonates born via cesarean section, DCC resulted in improved hematocrit levels by 72 hours compared to UCM. DCC results in better placental transfusion.
Introduction
Retaining the umbilical cord intact for a while rather than clamping it immediately after birth increases the newborn’s total RBC mass and eases the transition from fetal circulation to neonatal circulation [1]. In term neonates, placental transfusion provides enough iron stores, retarding the onset of iron inadequacy till iron-fortified meals are adopted [2]. In preterm neonates, placental transfusion decreases mortality and also improves the long-term neurodevelopmental outcome [1]. Delayed cord clamping (DCC) and umbilical cord milking (UCM) are the two main placental transfusion methods adopted in the delivery room for vigorous babies. However, UCM is not recommended for neonates born less than 29 weeks of gestation due to a lack of research regarding safety [3].
Even though UCM is being used as an alternate placental transfusion method, DCC offers more advantages than placental transfusion alone [4]. Animal study has showed that DCC after the establishment of good respiratory efforts or ventilation termed as physiological-based cord clamping improves pulmonary blood flow thus stabilizing cardiovascular and cerebrovascular transition during the early neonatal transition [5]. However, UCM did not have any effect on pulmonary blood flow and caused disturbance in carotid artery pressure and blood flows [6]. This may lead to disruption in normal neonatal transition and thus, hemodynamic instability. There are paucity of studies comparing effects of DCC with UCM on placental transfusion and clinical outcomes in late preterm and tern neonates delivered by cesarean section [7–9]. Our study aimed at evaluating the effect of UCM when compared with DCC among vigorous neonates born by cesarean section.
Methods
Study design
This open label randomized controlled trial was conducted in the tertiary neonatal intensive care unit in Southern India. The study was done between October 2020 and April 2022. The study was approved by the institutional ethics committee (No.129/IHEC/August 2020) and a clinical trial registry was obtained (CTRI/2021/03/031782). All vigorous neonates ≥35 weeks of gestation delivered by lower segment Caesarean section were included. Neonates requiring resuscitation at birth, excessive postpartum hemorrhage and cord trauma/avulsion, preterm infants <35 weeks, isoimmunization, or hydrops were excluded.
Standard operating procedure
Informed consent was obtained before delivery from mothers admitted for cesarean section with gestational age ≥35 weeks. After birth, the eligible infants were randomized to Group-A (Delayed clamping group) or Group B (Umbilical cord milking group). Randomization was done through computer-generated random numbers placed in serially numbered opaque envelopes, which were opened by a member of the resuscitation team, immediately after the baby’s birth, after a rapid assessment of the need for resuscitation. Blinding was not attempted due to the nature of the intervention. All neonates after birth, underwent intervention according to their allocated group. In the delayed cord clamping group, the baby was received in a warm sterile towel and held between the mother’s thigh. The cord was clamped after 60 seconds from birth and cut. In the UCM group, the intact umbilical cord was milked at a distance of 25 cm from the stump 3 times towards the baby, with a 1-second time interval to allow refilling and then the cord clamped 2-3 cm from the stump [3]. The maternal and neonatal details were collected in structured proforma.
Hematocrit and serum bilirubin were done at 72 hours after birth and all enrolled neonates were monitored for respiratory distress, need for phototherapy, hypotension, and sepsis. Downes score was used to assess respiratory distress at birth. Newborns with Downes scores of 2 and above were admitted to the newborn nursery. The neonates were screened daily for visible jaundice until discharge. If clinical jaundice was found to be substantial, serum bilirubin was measured and phototherapy was started as indicated by AAP charts for phototherapy [10]. Venous blood sampling was done around 72 hours after birth for routine TSH screening and a sample for checking hematocrit was taken at the same time. According to our hospital’s protocol, babies had a follow-up and vaccination around 6 weeks of age. Serum ferritin levels were measured using infants’ venous blood during this follow-up.
Outcomes
The primary objective of the study was to compare the level of hematocrit at 72 hours of life in term infants and preterm infants ≥35 weeks’ gestation between delayed cord clamping and umbilical cord milking groups. The secondary outcomes were to compare the serum ferritin measured between 6–10 weeks, serum bilirubin at 72 hours after birth, need for and duration of phototherapy between the two groups. Clinical morbidities like respiratory distress, hypoglycemia, hypotension, and sepsis were also compared.
Sample size
From a previous trial [11], it was decided that to detect a 5% difference in hematocrit, at an alpha error of 0.05 and 80% power, for a two-sided test, a sample size of 75 was required in each group. To account for a dropout rate of 10%, the determined sample size was 80 in each group.
Statistical analysis
Data was analyzed using R software Version 4.3.1. R Core Team (2021) [12]. Categorical variables are presented as frequency and percentages. Continuous data are presented as mean and standard deviation. The risk ratios were estimated and tested using poisson regression for binary outcomes. Mean difference was estimated and tested using t test for continuous outcomes. P-value was considered significant at 5% level of significance for all comparisons. Intention to treat analysis was performed.
Results
Out of 160 eligible neonates, 80 were randomized to group A (DCC) and 80 were randomized to group B (UCM) (Fig. 1). Babies who required resuscitation at birth were excluded and thus, each intervention group had 75 neonates. The mean (±SD) birth weights in DCC and UCM groups were 2960±470 and 2980±420 grams respectively. Baseline characteristics were comparable between both groups (Table 1). Only 15 (20%) mothers in the delayed cord clamping group and 23(30.6%) in the umbilical cord milking group had been given oxytocin. The mean (±SD) hematocrit at 72 hours was more in the DCC group compared to the UCM group [(55.60±4.50) vs (53.89±4.44), MD (95% CI) = 1.71(0.26, 3.16); p = 0.021] (Table 2). There was no significant difference in mean serum bilirubin at 72 hours [DCC 10.99±3.37 vs UCM 10.37±2.37; p = 0.071]. The duration of phototherapy was also not statistically significant. There was no significant difference in serum ferritin in both groups [DCC 102.88(84.67–173.24) vs UCM 137.93(85.15–230.40); p = 0.173]. There was no significant difference in clinical outcomes (Table 3).
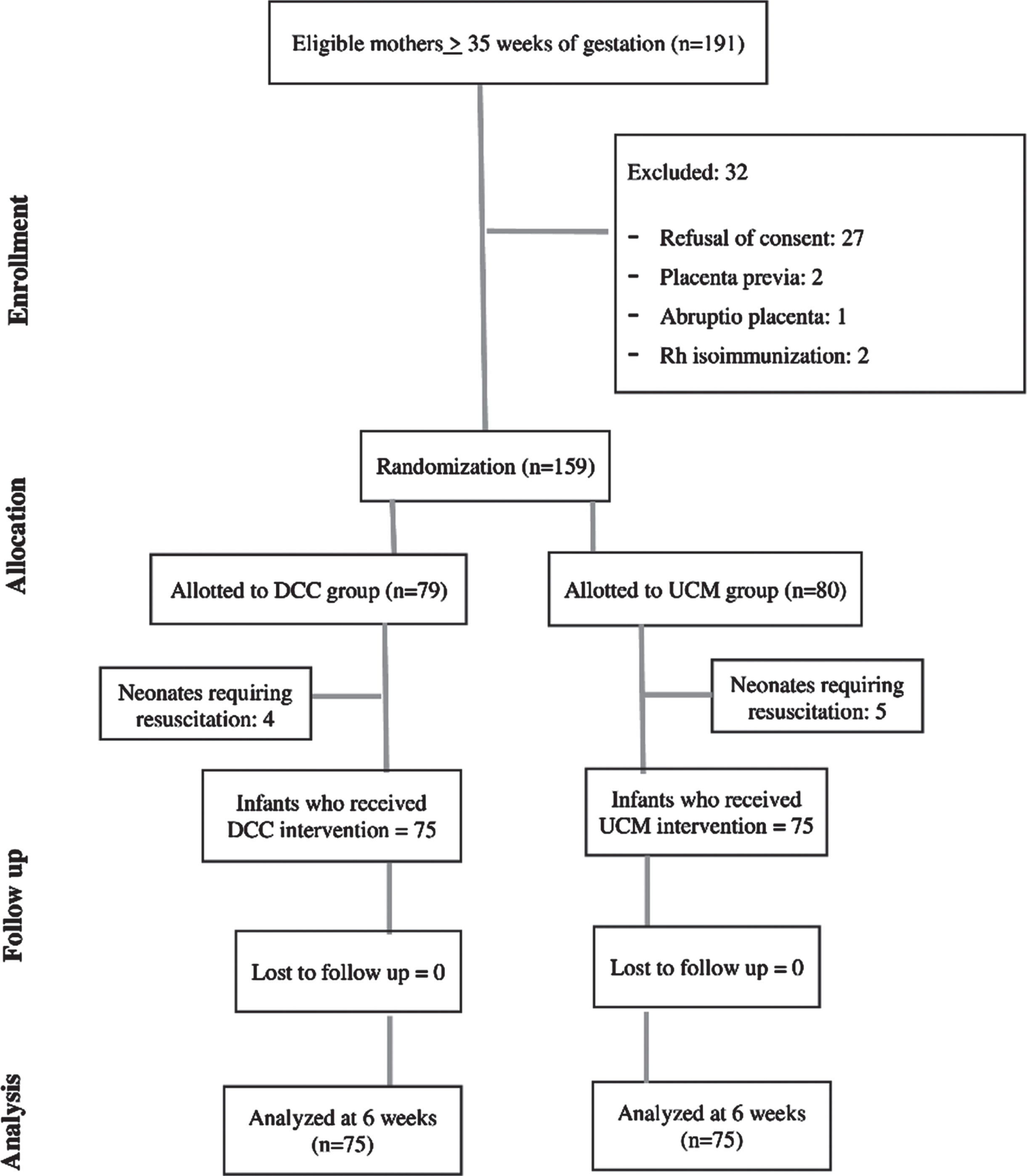
Flow of the study.
Baseline characteristics of the study subjects
¥Independent Sample T test. DCC –Delayed cord clamping; UCM –Umbilical cord milking.
Primary outcomes in the study subjects
¥Independent Sample T test. $Median(IQR)-Mann Whitney U test. DCM –Delayed cord clamping; UCM –Umbilical cord milking.
Clinical outcomes in the study subjects
RR – Relative Risk; RD – Risk difference; C.I - Confidence Interval; £Poisson Regression; ¥Mean Difference, Independent Sample T test.
Regarding placental transfusion during vaginal delivery, there was a false idea that the increased uterine tone due to contractions pushes the blood towards the neonate and hence in cesarean section, lesser transfer of blood and lesser hematocrit might occur due to ineffective uterine contractions [4, 14]. However, recent studies have clearly proven that blood tends to accumulate in the placenta during contractions and both umbilical arterial and venous flows cease during contractions. Even amplification of contractions by oxytocin has led only to decreased umbilical venous flow and net loss of blood from the lamb [15, 16]. This means that even in the absence of contractions as in elective cesarean section, DCC would aid in placental transfusion. Our study also showed that delayed cord clamping increased hematocrit levels when compared to umbilical cord milking in late preterm and term infants delivered by cesarean section.
In our study, the umbilical cord was milked towards the newborn who still had an intact cord. When compared to a newborn who receives the blood in the cut cord which has no connectivity with the placenta, intact cord milking results in larger placental transfusion [17–19]. In our study, the umbilical cord and placenta remained connected until the completion of milking. In our study where neonates delivered by cesarean section are included, the neonates are placed in between mothers’ thighs below the introitus in both groups. In vaginal delivery, it is recommended to receive vigorous babies over mothers’ abdomen [20]. Though it was initially believed that gravity and thus placing the fetus at a lower level than placenta aids in improved transfer of blood [4, 21], net placental transfusion volume into the baby is not affected by gravity according to recent studies [22, 23].
In our study, neonates allocated to the delayed cord clamping group had higher hematocrit values compared to the umbilical cord milking group. However, El Kotb et al. in a similar study on 300 term neonates born by elective cesarean section found no significant difference in hemoglobin levels between the two groups [9]. The mean Hb and hematocrit in the first 30 min and at 48h in Yadav’s randomized controlled trial, were also not different between the DCC group and the UCM group [8]. In the Cochrane review by Rabe et al., in 2019, the data was insufficient to conclude regarding the comparative effects of delayed cord clamping and umbilical cord milking [7].
Earlier study has shown that the volume of placental transfusion was dependent on the duration after which DCC was done, with higher hematocrit in neonates who had the cord clamped at 2 minutes or later, compared to those, who had their cord clamping done at 60 secs [24]. The variable duration of cord clamping beyond 60 seconds in our study, could have resulted in a higher placental transfusion, resulting in the higher hematocrit levels. In premature sheep models, UCM with placental refill (UCMwPR) where fetal end of umbilical cord was occluded after each milk so that refilling happens from the placental end only and then placental end was occluded before milking so that umbilical cord retains its volume resulted in increased net umbilical blood flow into the lamb when compared to UCM without PR and DCC [6]. We used release method or UCM without placental refill method. This might be the reason for lesser placental transfusion or hematocrit in the UCM group.
The potential problem expected with a higher hematocrit level is higher incidence of jaundice, which in turn might result in increased requirement for phototherapy. However, despite the higher hematocrit levels in the DCC group, the mean bilirubin levels at 72 hours were not higher. Also, the need for phototherapy was not significantly different between the groups. These findings were concordant with other studies, which showed that DCC compared UCM, did not result in increased requirement for phototherapy [25, 26].
Despite the increased hematocrit levels at 72 hours, noticed in the DCC group, there was no discernible difference in the ferritin readings at 6–10 weeks between the two groups. Iron stores in infancy are determined by many factors like the type of infant feeding, utilization of added iron supplements, and baseline iron stores at birth [27]. This could explain the lack of significant difference in the ferritin levels between the groups.
In conclusion, DCC results in improved hematocrit levels by 72 hours after birth compared to UCM in neonates born via cesarean section. Thus, DCC facilitates placental transfusion in cesarean as well.
Conflict of interest
None.
Funding
None.
Data availability statement
The data that support the findings of this study are available from the corresponding author, U.D, upon reasonable request.