
Abstract
BACKGROUND:
A novel home monitoring program, in which premature infants are cared for at home with a nasogastric tube in place prior to achievement of full oral feeding, was evaluated. The program combines a digital, fully EMR-integrated, virtual daily rounding platform with direct provider video and telephone contact.
METHODS:
A case-control study was performed evaluating infants < 34 weeks’ gestation who were followed in our program. A historical control group, was created by matching 2 : 1 based on gestational age±6 days, retroactively.
RESULT:
15 patients discharged in the program were compared with 30 controls. The home cohort gained an average of 30 g/day compared with the in-hospital group at 27g/day (p = 0.325). The home group required a mean of 5.9±2.9 days to full oral feeding once discharged, not different from the control group at 5.4±3.7 days (p = 0.606). The percentage of oral feeds for the home cohort, however, increased at a rate of 12.2%before discharge compared to rising 57%at home (p < 0.001). The control group spent an additional 8.1±3.9 days in the hospital after reaching criteria. There were no reported adverse events or readmissions.
CONCLUSION:
Premature infants can safely advance oral feeds using a home monitoring program. While at home, infants gained weight similarly to their inpatient controls, yet gained full oral skills at a significantly faster rate compared to when they were in the hospital.
Abbreviations
Electronic Medical Record Home Monitoring Program Neonatal Intensive Care Unit Nasogastric Tube Postmenstrual Age
Introduction
In 2018, there were approximately 3.8 million live births in the United States, with about 380,000 infants born premature (9.93%). Of these, 93%are born moderately preterm or late preterm [1]. Preterm infants account for half of all infant hospitalization costs in the United States [2, 3]. For these infants, 20%–40%will remain hospitalized beyond 36 weeks post-menstrual age due to inadequate oral feeding [4, 5]. These infants had already met other commonly accepted criteria for discharge, including normothermia in an open crib, no respiratory support or home oxygen settings, and completion of an apnea countdown.
Additionally, prolonged hospitalization of a neonate is associated with significant parental distress including disturbance in parental bonding and higher rates of marital turmoil [6]. Earlier discharge from the neonatal intensive care unit (NICU) to the home environment can improve parental stress and promote parental bonding [7–9].
Previous studies have shown that discharging premature infants who meet criteria for NICU discharge, though still dependent on nasogastric (NG) tube feedings for hydration status, can be safe and cost-effective [10–12]. Commonly, neonatologists hesitate to discharge infants with home NG tubes given concern for complications related to the NG tube and the inability to monitor and support the infant’s progress across a variety of socioeconomic, cultural, and geographic situations.
We initiated a novel home monitoring program (HMP) for infants that met all criteria for discharge except for being able to maintain their hydration status orally, thus still requiring an NG tube. The HMP combined a digital, fully electronic medical record (EMR) integrated, virtual daily rounding platform with direct provider video and telephone contact. We aimed to study the safety and efficacy of the program by comparing the preterm infants discharged into the HMP program with a historical cohort of infants that would have been eligible for the program but were discharged before its initiation.
Methods
The structure of the HMP consisted of the provision of education for families to obtain weights, document their child’s feeding progress, and proper management and placement of NG tubes. Furthermore, they were provided with a scale and a secured, iPad® directly connected to our institution’s EMR. Families were able to input daily data including weight, volume per feed (stratified by NG tube vs. oral), and output (emesis and diaper counts) that were viewable by the clinicians through the EMR. Infants at home were rounded upon by the care team as part of routine daily rounds within the NICU. The care team reviewed data and documented progress and potential changes within the EMR daily. Families were contacted as clinically appropriate to necessitate interventions, provide assessments, answer questions, or address concerns at least three times per week. If speech therapy or nutrition services were required, a direct video link to the families at home was made using the platform. Families were discharged from HMP when the infant was either taking all oral feeds for 5–7 days and showing appropriate weight gain or had received a gastrostomy tube. The primary pediatrician for the patients continued to see the patients in the home monitoring program as they would any infant discharged from the NICU. The care team in the NICU communicated with the pediatrician prior to the infant’s discharge to coordinate our roles in the patients care after discharge. The NICU continued to make changes only in relation to feeding while the parents were instructed to contact their pediatrician with any other concerns.
We performed a retrospective case-control study of all infants less than 34 weeks’ gestation at birth who were followed in our HMP between February 2018 and February 2019. Infants were eligible for our HMP, and thus met inclusion criteria for this study, once their post-menstrual age was greater than 35 weeks, weight greater than 2 kg, had completed their apnea countdown (apnea free for 7 days) [13], maintained thermoregulation for at least 2 days in an open crib, and were taking approximately 35–50%oral feedings. The percentage of oral feed inclusion criteria existed to prevent need for emergent visits for NG replacement to maintain hydration. Additionally, parents needed to agree to home NG and have completed all NG education prior to discharge. Infants with abnormalities on genetic testing, significant congenital anomalies, or obvious phenotypic syndromes were included in the HMP but were excluded from this study secondary to concern in finding appropriate matches.
A historical, pre-HMP, control group was created using infants that met the same inclusion and exclusion criteria as the HMP group. Infants were gathered by identifying all infants less than 34 weeks’ gestation starting in December 2017 using our institutional database and working backward until a 2:1 match was created for each HMP case. Match criteria was by gestational age±6 days. The same exclusion criteria as the HMP group were utilized. These control infants were deemed ready for discharge at the time they met the HMP criteria and would have been discharged into it, had it existed at the time. No patient before June 2016 was matched to ensure similar eras of enrollment.
Complete demographic and background data were collected to compare the two groups. Feeding outcomes, including the time to full oral feeds, length of time with NG tube, and weight parameters were gathered to assess for differences in patients who were kept in the hospital (historical cohort) and patients who were sent home with NG tubes (HMP cohort). All patients were analyzed in the group in which they met criteria. Short-term readmissions were defined as readmission to our institution within 30 days of discharge from the initial hospitalization. All infants were discharged into our institution’s catchment area, reducing the likelihood of unknown readmissions to other centers.
Continuous, normally distributed data are reported as mean±standard deviation while non-normal data are presented as medians with interquartile ranges, where appropriate. Categorical variables are reported as frequencies (%). Comparisons were made using appropriate parametric and non-parametric hypothesis testing for both continuous and categorical variables. A p-value of less than 0.05 was considered significant. Daily feeding data for the HMP group was displayed using a run chart, though control limits were not added due to total numbers.
Parental consent was obtained before discharge home into the HMP. This study was approved by the Institutional Review Board of the University of Virginia.
Results
There were 26 patients followed in the home monitoring program between February 2018 and February 2019. After applying exclusion criteria, we had 15 patients that were matched with 30 historical control infants discharged between June 2016 and December 2017 before the start of the HMP. Two patients were excluded because they were monitored only for weight gain and taking all PO at discharge; six were excluded for gestational age > 34 weeks; two were excluded due to genetic syndromes; and one was excluded for significant congenital anomaly. Results comparing the initial baseline demographics of the two groups are displayed in Table 1. There was no difference in gestational age, size, sex, or proportion of twin pregnancies. There was also no significant difference with regard to post-menstrual age at completing their apnea countdown and ability to maintain thermoregulation in an open crib.
Patient demographics
Patient demographics
PMA, post-menstrual age.
Table 2 displays the age and weight of the infants at the time of discharge. With regard to post-menstrual age at the time of discharge and weight at discharge, there were no significant differences between the two cohorts. There was a statistically significant difference between the post-menstrual ages at meeting home monitoring criteria with the children discharged into the home monitoring program having an older post-menstrual age. Also, the infants that were discharged into the home monitoring program were bigger at the time they met home monitoring criteria compared with the infants that received standard in-hospital care. At the time the infants met home monitoring program criteria, there was no significant difference in the percent PO the infants were taking and in total length of stay.
Patient data at time of discharge
PMA, postmenstrual age; LOS, length of stay; EBM, expressed breastmilk.
Infants that remained hospitalized working on PO skills spent an additional 8.13±3.9 days in the hospital prior to discharge. The time for the standard in-hospital care infants to transition to full oral feedings once they met home monitoring program criteria was 5.4±3.7 days. The time to full feeds was not different from infants who advanced their home feedings in the home monitoring program, which was 5.9±2.9 days. Infants spent an additional 2–3 days in the hospital after mastery of full oral feedings to ensure ongoing oral skills in addition to appropriate weight gain. Importantly, there was no significant difference in average daily weight gain between the standard in-hospital care cohort compared with the home monitoring patients while they transitioned to full oral feedings. (27.2±10.6 vs 30.4±9.7 g/day).
Line charts depicting percent oral feeding over the course of the last 20 days of their care for the home monitoring cohort and the standard in-hospital care cohort are displayed in Fig. 1 and Fig. 2, respectively. Both groups were subjectively slow to advance oral feeding at the time they met HMP criteria. After they met criteria, or were discharged into the HMP for the case group, there was a similar rapid rise in their percent oral feeding. Furthermore, the HMP demonstrated a higher day-over-day increase in their PO abilities after discharge than they had achieved prior to discharge. This equated to an average increase of 12.2%in oral feeding during the 10 days prior to discharge compared to an increase on average of 57%once at home (p < 0.001).

Home monitoring patients %oral feeding by day. Line chart depicting %oral feeds over the course of the 10 days prior to discharge and the first 10 days in the home monitoring program.
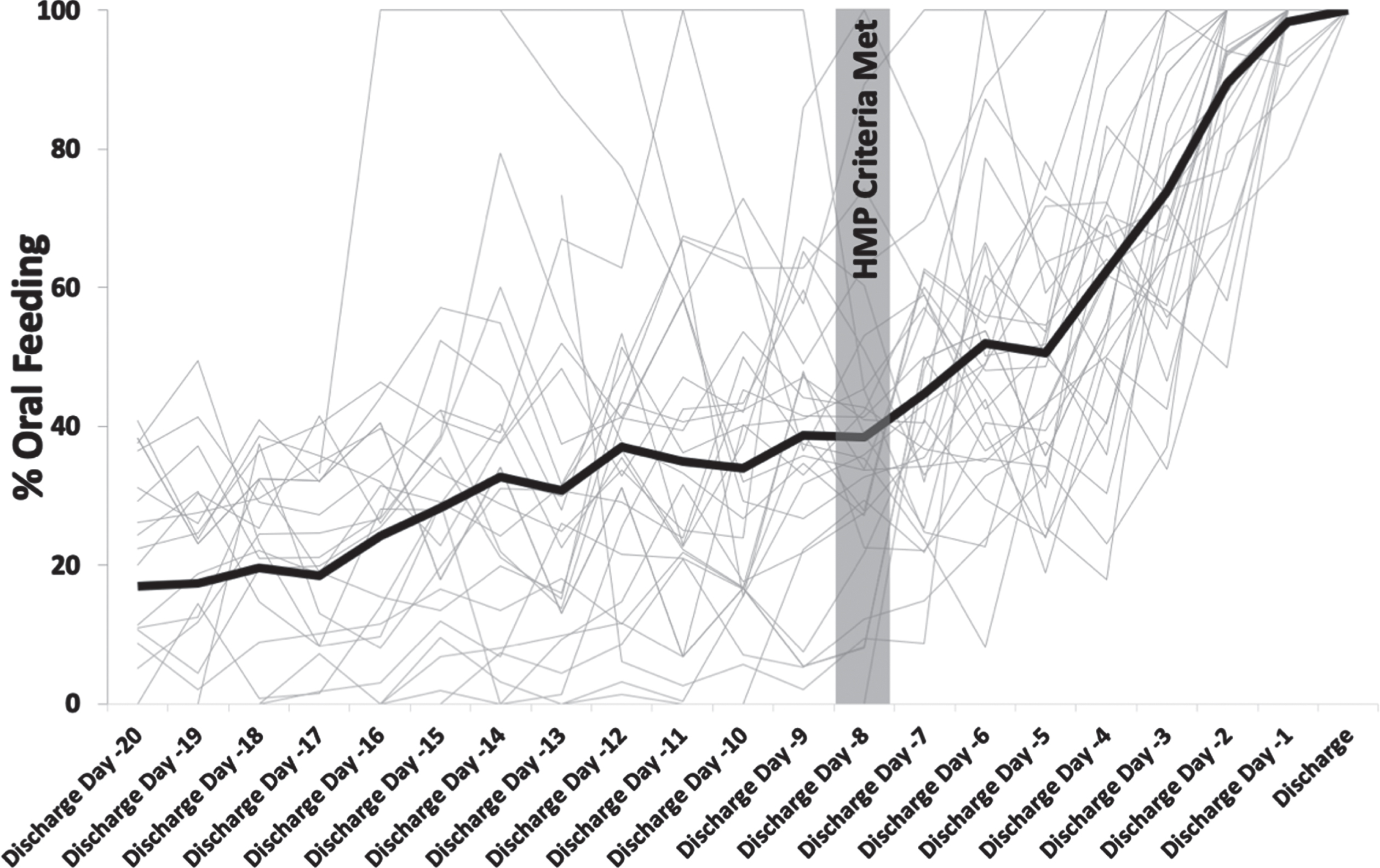
Standard in-hospital patients %oral feeding by day. Line chart depicting the %PO of the standard in-hospital care patients for the last 20 days of their hospitalization. The average amount of time they spent in the hospital after meeting HMP criteria was 8 days. This is marked on the line chart.
Adverse events determined a priori included; malposition NG, aspiration events, pediatrician discomfort, ED visits, and hospital readmission. There were no reported adverse events based on rounding phone calls and chart review, including 30-day readmissions for either cohort of patients.
The objective of this study was to assess the safety and outcomes of a novel home monitoring program for infants that were continuing to work on developing their oral feeding skills. The results of the study show that premature infants who were discharged into our home monitoring program to develop their oral skills in the home environment were able to advance to full oral feeds safely and effectively. The time to transition to full oral feedings and removal of the NG tube (5–6 days) were similar between the patients that were managed in the hospital versus those that were managed via a virtual rounding model. This demonstrates that the home monitoring program for infants working on continued oral skills is not inferior to in-hospital care. The most important aspect was that the infants discharged into the home monitoring program gained weight similarly to those that remained hospitalized.
The data would suggest that the infants did better in the home environment compared to the hospital. One explanation for this is that the patients at this time were bigger and older, than they were the week before. While this remains a very distinct possibility, it seemed predictable that they significantly increased their oral feeds once at home compared to the hospital. At a minimum, these patients orally fed with a similar pattern to the control group suggesting non-inferiority of the HMP to standard in-hospital care.
One significant difference between the two groups was that the children discharged into the home monitoring program were significantly older and larger at the time of meeting home monitoring criteria. When the program began, enrolled patients were considered significant outliers with regard to obtaining their oral skills. Many of the initial patients in the program met the home monitoring program criteria, as described in the study, earlier than their discharge date into the home monitoring program. For this study, we used their discharge date as the date they met HMP criteria and thus likely contributing to the significant difference between the weight and age of the infants that were discharged into the HMP program. While the retrospective design of the study limits our ability to comment on the causality of these differences the similar rate of feed increase limits the impact of this difference. Further research is needed to evaluate the growth trajectories of infants receiving NG feeds using the home monitoring program versus the neonatal intensive care unit.
Multiple NICUs have published their results discharging infants into a home NG program. Previously published programs rely on nurse visits or outpatient clinic visits to monitor the patient’s progress in the program and determine the timing of removal of the NG tube in addition to demonstrating safety in this initiative [10, 14].
Our program is novel in that it uses a remote patient monitoring platform in which the parents enter the same types of data monitored while the neonate was still admitted to the NICU. This includes daily weights, oral versus tube feeding volumes, breastfeeding, and emesis. If the parents were to enter a concerning value (such as excessive weight loss), it would alert the parent to call the neonatologist on call. The NICU team perform daily virtual rounds to determine the timing of NG tube removal and other potential interventions for the patient. Using real-time data and daily rounds, instead of relying on nurse phone calls or clinic visits, allows for more timely intervention with regard to advancing feeds and removal of the NG tube. Phone or secure video connection remained a significant component of our program, occurring approximately 3 times per week to connect with parent. The digital transfer of information in this HMP limited the need for family travel and in-person nursing or office visits.
The primary limitation of this study is the retrospective nature. The nature of the study makes it difficult to determine when the children in the control cohort would have been discharged into the program had the program existed. This is single-center study and therefore the practices and discharge criteria may differ from other institutions. We were not able to assess the social situations surrounding parental decisions to be discharged into the home monitoring program. Additionally, we did not factor in social considerations of the control cohort.
Conclusion
Use of a novel home NG feeding with remote patient monitoring for premature infants that remain hospitalized solely working on obtaining oral feeding skills was associated with comparable feeding outcomes without adverse events. Remote patient monitoring and discharge with home NG feeds has the potential to significantly decrease the length of stay for a cohort of NICU patients who remain hospitalized exclusively for acquisition of oral feeding skills.
Footnotes
Acknowledgments
The authors would like to acknowledge our families that participate in the home monitoring program. We would also like to acknowledge the entire NICU team for their participation in the program.
Potential conflicts of interest
The authors have no conflicts of interest, financial or otherwise, relevant to this article to disclose.
Human research statement
The authors affirm that this research was conducted in accordance with the ethical standards of all national and institutional committees. The research was reviewed and approved by the University of Virginia IRB.