
Abstract
BACKGROUND:
There is little published data on how to prepare probiotic supplements for enteral delivery in the NICU. The objective of this study was to determine how a three-strain probiotic blend (Bb-02, TH-4® and BB-12®) would behave when mixed and held for 4 hours with saline water, sterile water, dextrose 5% in water (D5W), 24 kcal preterm formula, and human milk.
METHODS:
A packet of a three-strain probiotic supplement was mixed with 3 mL of saline water, sterile water, D5W, 24 kcal preterm formula, and human milk (tested at 3 mL and 2 mL). Samples were stored at room temperature for 60 minutes then refrigerated for 180 minutes. Probiotic survival, using quantitative enumeration, and pH were monitored over 4 hours. Samples were passed through a 5 French (Fr) feeding tube at the end of the study to evaluate viscosity.
RESULTS:
The largest variation in total cell count from 0-time was sterile water with a + 0.26 log(CFU)/mL change at 90 minutes and typical variation is considered±0.50 log units indicating no significant change between samples in 4 hours. Saline water had the lowest final pH at 4.88. All samples easily passed through a 5 Fr feeding tube.
CONCLUSION:
The study showed minimal change in cell counts across solutions for 4 hours of storage, indicating health care facilities may be able to prepare probiotic supplements with a variety of solutions in pharmacies or milk rooms. This allows greater flexibility for probiotic delivery to preterm infants.
Abbreviations
Neonatal intensive care unit
Dextrose 5% in water
Human milk
Deionized
Colony forming units
Introduction
Probiotics are live microorganisms that confer benefit to the host and have been studied in over 11,000 preterm infants over the past 20 years in multiple clinical studies yet routine prophylactic probiotic use in United States (USA) Neonatal Intensive Care Units (NICUs) is still low [1–3]. The low use in the USA may be in part due to uncertainty as to which probiotic strain or combination of strains to use for which desired outcome, and in part due to lack of understanding of how to evaluate product stability and safety [2–4].
To date, there is very little published data as to how best to prepare specific probiotic supplements for enteral delivery to preterm infants. Probiotic preparation varies from hospital to hospital, and media selection may be based on the location of preparation (pharmacy or NICU). Since certain probiotic supplements should be mixed into 2-3 mL of media and administered enterally to the infant separately from feedings, practical clinical questions have been raised about what media can be used to reconstitute probiotics. Specifically, what is the viability of probiotics, the impact of probiotics on the solution pH, and the stability of the probiotic strains when mixed with different media and held for a period prior to administration to the infant? This study investigates the viability, the solution pH, and stability of the three-strain probiotic blend Bifidobacterium infantis (Bb-02), Streptococcus thermophilus (TH-4), and Bifidobacterium lactis (BB-12) when mixed with saline water, sterile water, dextrose 5% in water (D5W), 24 kcal preterm infant formula, and human milk (HM) for up to 4 hours storage.
Methods
A probiotic supplement (Abbott Nutrition, Columbus, Ohio) containing Bifidobacterium infantis (Bb-02), Streptococcus thermophilus (TH-4®), and Bifidobacterium lactis (BB-12®) was mixed with sterile water (Abbott Nutrition), dextrose 5% in water (D5W) (Abbott Nutrition), 24 kcal preterm infant formula (Similac Special Care 24) (Abbott Nutrition), 0.9% saline water (sterile water + NaCl), and human milk (HM) (Lee Biosolutions, Maryland Heights, MO). All solutions were brought to room temperature and mixed at a ratio of 1 probiotic sachet (0.5 g) to 3 mL of solution. HM was mixed at an additional ratio of 1 sachet to 2 mL of solution. The probiotic mixtures were held at room temperature for 0 to 60 minutes and then refrigerated from 60 to 240 minutes. Samples were collected for pH testing (SevenEasy pH, Mettler-Toledo GmbH, Schwerzenbach, Switzerland) at 0-time, 30 minutes, 60 minutes, 90 minutes, 120 minutes, and 240 minutes. Prior to the start of the experiment the pH meter was calibrated with a pH 4.0, 7.0, and 10.0 buffer and pH readings were taken in duplicate for each sample at each time point. At 240 minutes the samples were passed through a 5 French (Fr), 1.7 mm×51 cm, feeding tube (Kangaroo Polyurethan Feeding Tube, Covidien, Mansfield, MA, USA) using a 10 mL syringe (Luer Slip Disposable Syringe, CareTouch, Brooklyn, NY, USA) to ensure flowability.
One probiotic sachet was mixed with 3 mL of dei-onized (DI) water and 5 mL of DI water and tested for osmolality. An average osmolality of 291 mOsm/kg was assumed for preterm HM [5]. The resulting osmolality of the probiotic in DI water was added to the average osmolality of preterm HM to predict the osmolality of preterm HM supplemented with 1 probiotic sachet.
Samples from all mixing solutions were enumerated at 0-time, 30 minutes, 60 minutes, 90 minutes, 120 minutes, and 240 minutes. To obtain the total cell count 2 probiotic sachets were combined with 6 mL of solution (sterile water, D5W, formula, saline water, HM) and mixed for 2 minutes. An additional variable was performed for HM combining 3 probiotic sachets with 6 mL of HM. At each time point, a 1 mL aliquot was pulled for serial dilution in Maximum Recovery Diluent (for example Oxoid CM0733), transferred to sterile petri dishes and mixed with de Mann, Rogosa and Sharpe (MRS) agar fortified to contain cysteine hydrochloride (0.19%) and sodium carbonate (0.14%) [6, 7]. The dishes were placed in anaerobe jars containing AnaeroGenTM sachets (Thermo Scientific, Waltham, MA), or equivalent, and incubated for 5 days at 37°C. The recovery at each time point was then calculated and results were transformed to log (Colony Forming Units (CFU) per mL of sample).
The experiments were carried out in duplicate and each enumeration was plated twice. An ANOVA was run on the log (CFU)/mL data comparing the rehydration solution across time points and comparing the time intervals with the different rehydration solutions using Minitab 19 (Minitab, State College, PA, USA). The p-value was set at p < 0.05 and a Tukey Pairwise comparison, at a 95% confidence interval, was performed when a difference existed in the ANOVAs.
Results
There were no significant differences (p < 0.05) in total cell counts observed when the probiotics were dispersed and stored in D5W, sterile water, formula, HM (1 packet: 3 mL HM and 1 packet: 2 mL HM), and saline water in any solution across time. Figure 1 is comparing the difference in the total cell count at each time point to the initial total cell count (Fig. 1). The greatest variation from 0-time was in sterile water at 90 minutes with an increase of 0.26 log (CFU)/mL. Typical quantitative enumeration methods have a reliability of±0.5 log units indicating the variability in total cell count may have been contributed to method variability [6, 8–10]. The total cell counts of each solution were compared to one another at each time point (Fig. 1). There was no significant difference (p < 0.05) in the total cell count data [log(CFU)/mL] among solutions at 0-time, 30 minutes, 60 minutes, 120 minutes, and 240 minutes. At 90 minutes sterile water had a significantly larger increase from 0-time than all other solutions. However, at the following time point sterile water was not significantly different from 0-time.
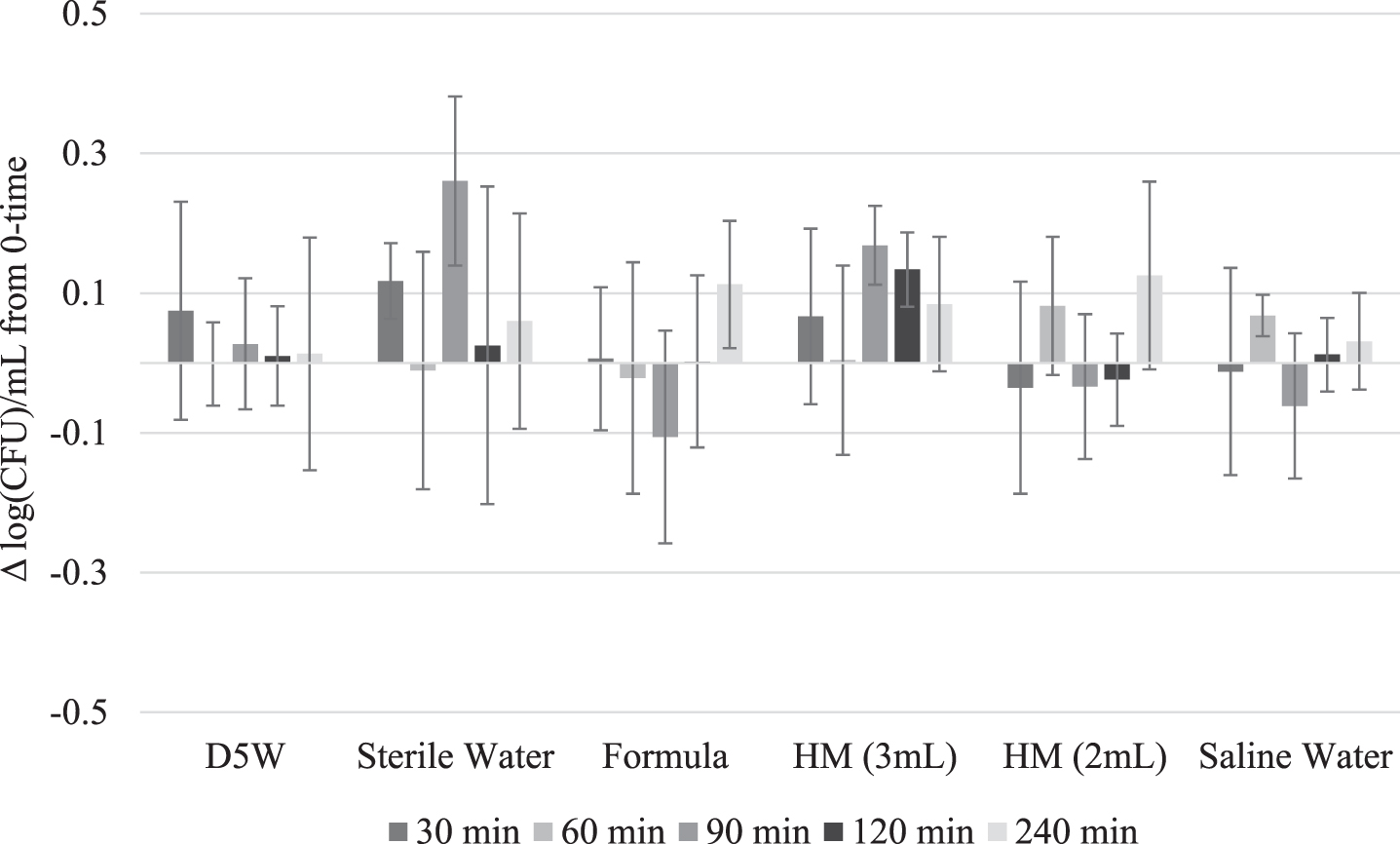
Probiotics total cell count change in the log (CFU)/mL between 0-time and 30, 60, 90, 120, and 240 minutes when the probiotics were stored in D5W, sterile water, preterm formula, HM (1 sachet: 3 mL HM and 1 sachet: 2 mL HM), and saline water and the associated standard deviations. No significant difference existed in the total cell count between time points of any solution (p < 0.05).
Table 1 shows the results of the average pH values of each probiotic solution at each time point (Table 1). Preterm formula had the largest decrease in pH from 6.33 at 0-time to 5.47 at 240 minutes indicating a significant (p < 0.05) change of 0.86 pH units. Saline water had the lowest pH reading (pH 4.88) at 240 minutes. HM (1 packet: 3 mL HM and 1 packet: 2 mL HM) exhibited the smallest change in pH value.
Average pH values of sterile water, D5W, HM, saline water, and preterm formula mixed with the probiotics over 4 hours of storage (60 minutes room temperature and 180 minutes at refrigeration)
1 HM diluted at a ratio of 1 sachet probiotics: 3 mL HM. 2 HM diluted at a ratio of 1 sachet probiotics: 2 mL HM. 3 (0 minute pH) –(240 minute pH) = Total change. 4 pH value with the highest standard deviation of 0.092. 5 HM (2 mL) is not significantly different between 0-time and 240 minutes (p < 0.05).
To impact preterm infants the probiotics must remain viable from point of manufacture to feeding [11, 12]. The low water activity and moisture content of the probiotic used kept the probiotics in dormant state during storage, until rehydration at time of their usage. Once rehydrated, the three-strain probiotic maintained a constant cell count, over 4-hours of storage, in sterile water, D5W, saline water, formula, and HM (Fig. 1). In Fig. 1, all total cell counts have a change less than 0.5 log units, which is the standard accepted variability range for quantitative enumeration methods, indicating consistency in total cell counts across 4-hours of storage [6, 8–10]. In the clinical setting, probiotics are often mixed and delivered quickly. However, for routine hospital use, the probiotics may be mixed in pharmacies or milk rooms and held for several hours prior to feeding. When mixed in pharmacies, sterile water, saline or D5W may be the preferred media for probiotics preparation. Since the probiotic supplementation is to be fed separately from routine feedings, fortified HM was not studied as a media for mixing. The study showed the three-strain probiotics remained viable at stable concentrations over 4-hours of storage potentially providing greater flexibility for use in hospitals. This data aligned with a study that looked at the storage of single strain probiotics in human milk [13].
An additional study was performed to observe the effect of pumping of the probiotic mixture through a 5 Fr feeding tube, similar to how the probiotic would be delivered in the NICU. The probiotics were mixed with HM, and the probiotics total cell counts were monitored throughout pumping. It was found that the variation pre and post pumping was within the standard testing error for total cell count [6, 8–10], demonstrating the majority of the probiotics will be delivered to the infants. The delivery of viable probiotics to infants allows the probiotics to have a desired impact on the preterm infant [2, 12].
The variability of rehydration solutions would allow health care professionals to customize probiotic delivery. The results showed if the probiotic is delivered via HM, the potential acidic byproduct of the probiotics had minimal effect on the pH of HM (Table 1). The delivery of probiotics in HM may provide additional benefits compared to formula or other solutions [14], but the probiotics must not acidify or alter the milk’s cellular and nutritional components [15]. The results showed the buffering capacity of HM could neutralize potential acidic fermentation products the probiotics may have created [15, 16]. Although HM at a dilution of 1 sachet to 3 mL of HM had a significantly different pH from 0-time and 4-hours the pH increased indicating the nutritional components of the HM were likely not affected.
Formula had the largest change in pH even though it has a high buffering capacity. Formula’s pH change may have been associated with the available carbohydrates such as lactose and corn syrup solids in the formula. An increase in available nutrients of the rehydration solution could have led to growth of the microorganisms producing acidic byproducts [17]. The formula experienced a large pH drop, but the pH after 4 hours of storage was 5.47, which is still above the typical gastric pH of preterm infants [15, 18]. D5W and sterile water have no buffering capacity and experienced changes in pH. However, both D5W and sterile water had pH values above 5.0 through 4-hours of storage. If D5W and sterile water are being used to rehydrate and deliver the probiotics, these beneficial microorganisms are likely being delivered before or after a feeding so the reduced pH should not impact HM [19]. Saline water dropped below pH 5.0 approaching the acidified range, so caution should be taken when using saline water as a rehydration solution.
Preterm infants are often intolerant of high-volume enteral feeds [19, 20], making the volume of probiotic rehydration solution critical. In order to address that, one experimental dilution was carried out using 2 mL of HM with 1 probiotic sachet, 1 mL below the recommend 3 mL volume. The smaller dilution volume did not have an impact on cell viability. The cell count remained constant over the 4-hour hold period. There was no significant difference between the 0-time and 4-hour pH of the 2 mL HM sample. These probiotics were also dissolved easily in 2 mL of HM, and the cell count and pH remained constant over 4 hours of storage indicating that small volumes of rehydration solution may be used to deliver three-strain probiotics. However, the osmolality of the solution should be considered.
As the volume of the feeding decreases the osmo-lality of the feeding increases. The American Aca-demy of Pediatrics recommends infant feedings do not exceed 450 mOsm/kg [21] and a recent study has challenged the 450 mOsm/kg maximum [5]. The probiotic contains maltodextrin which will increase the osmolality of the rehydration solution. When the probiotic was mixed with 3 mL of DI water the osmolality was 137 mOsm/kg H2O and when mixed with 5 mL of DI water the osmolality was 73 mOsm/kg H2O. The average osmolality of preterm HM is around 291 mOsm/kg [5], so the addition of 1 probiotic package to 3 mL of HM would yield an estimated osmolality of about 428 mOsm/kg and 1 probiotic packet to 5 mL HM would project an osmolality of about 364 mOSM/kg. The increase in osmolality with the addition of three-strain probiotics should be taken into consideration, when preparing and feeding these microorganisms to preterm infants.
All probiotics dissolved easily in the rehydration solutions and provided similar total cell count [log (CFU/mL)] data indicating the probiotics were homogenously distributed in these media. After 4 hours of storage, all samples flowed easily through a 5 Fr feeding tube, ensuring the delivery of the probiotics will not clog the preterm infants enteral feeding tube.
Conclusion
In conclusion, the total cell counts revealed that the three-strain probiotic was stable in sterile water, D5W, saline water, formula, and HM over 4 hours of storage. The pH of HM remained relatively constant over 4-hours of storage, while formula, sterile water, and D5W had decreases in pH but remained above pH 5.0. Saline water had the lowest final pH of 4.88. The results showed that HM, formula, D5W and sterile water may be good rehydration solutions for the delivery of probiotics to preterm infants. To our knowledge, this is the first study investigating the stability and viability of Bifidobacterium infantis (Bb-02), Streptococcus thermophilus (TH-4) and Bifidobacterium lactis (BB-12) in sterile water, D5W, saline water, formula, and HM. Probiotics must be viable to deliver potential health benefits to preterm infants and this study confirms the viability of the probiotics over 4 hours of storage with various media. The variety of rehydration solutions used in this study may provide greater flexibility for the use of probiotics in hospitals. More experiments should be conducted to add on to this study and therefore potentially expanding the practical knowledge of probiotic usage in different solutions, determining the ideal storage conditions of rehydrated probiotics, and the effect of the probiotics on the rehydration solution.
Funding
The study was funded by Abbott Nutrition.
Financial disclosure
All authors received research funding from the study sponsor, Abbott Nutrition, to conduct the study.
Conflict of interest
All authors are employees of Abbott Nutrition.
Footnotes
Acknowledgments
We thank Sara Mager, of Abbott Nutrition, for assistance with the plating and incubation of the probiotics that was required to obtain the total cell count data at each time point.