
Abstract
Emphysematous gastritis is a rare and life-threatening condition caused by gastric inflammation and intramural gas formation, most often diagnosed through radiological evidence of a radiolucent shadow in the stomach wall in the clinical scenario of severe sickness. We report a case of emphysematous gastritis secondary to early-onset neonatal sepsis in a newborn which, to the best of our knowledge, has not otherwise been reported. Is it very rare or do we just miss it?
Keywords
Introduction
Emphysematous gastritis (EG) has been described as a rare life-threatening condition caused by gastric inflammation and intramural gas formation, most often diagnosed through radiological evidence of a shadow in the stomach wall in cases of severe sickness [1]. Early diagnosis and aggressive management are key to securing survival and good outcomes in EG [2].
We report a case of emphysematous gastritis secondary to early onset neonatal sepsis (EONS) in a newborn.
Case report
An emergency lower uterine segment caesarian section was performed for a twin pregnancy in view of antepartum hemorrhage and premature rapture of membranes (PROM) for more than six days with breech presentation of the first twin at 31 weeks’ gestation. Both babies received routine neonatal care and cried immediately after birth with APGAR scores of 8, 9, and 9 (Twin A) and 7, 8, and 9 (Twin B) at 1, 5, and 10 minutes of life, respectively. The babies’ birth weights were 1.45 kg and 1.70 kg and both were moved to the NICU and started on IV antibiotics, in light of the PROM and their prematurity, once sepsis screening and blood cultures had been sent.
Expressed breast milk (EBM) feeding @ 10 ml/kg/d, two hourly was later started by orogastric (OG) tube. Monitoring by abdominal circumference charting (to quantify increase in AC > 2 cm) and pre-feed residue (25% or more of feeds) were introduced for the babies to assess tolerance of feeds. Twin A accepted and tolerated the feeds well, but Twin B vomited after feeding on the second day of life. The baby was otherwise hemodynamically stable. EBM feeding was continued for baby A, but the twin B was kept nil orally for 48 hours and on day four EBM feeds were reintroduced as hourly feeds, instead of every two hours because of previous feed intolerance. Sepsis screening was negative. On the third day, repeat sepsis screening became positive with CRP increasing to 12.77 mg/L.
On the fifth day of life, Twin B had blood stained gastric residue and three episodes of apnea. There was abdominal distension, and so feeding was suspended and anteroposterior and lateral X-rays were ordered. There was also skin mottling of skin and some features of shock, so inotropes were started with IV fluids, antibiotics were upgraded, and caffeine citrate injection was added. The X-ray showed gas in the wall of the stomach but not the intestinal wall (i.e., there was no pneumatosis intestinalis) (Fig. 1). An abdominal ultrasound showed minimal free fluid.
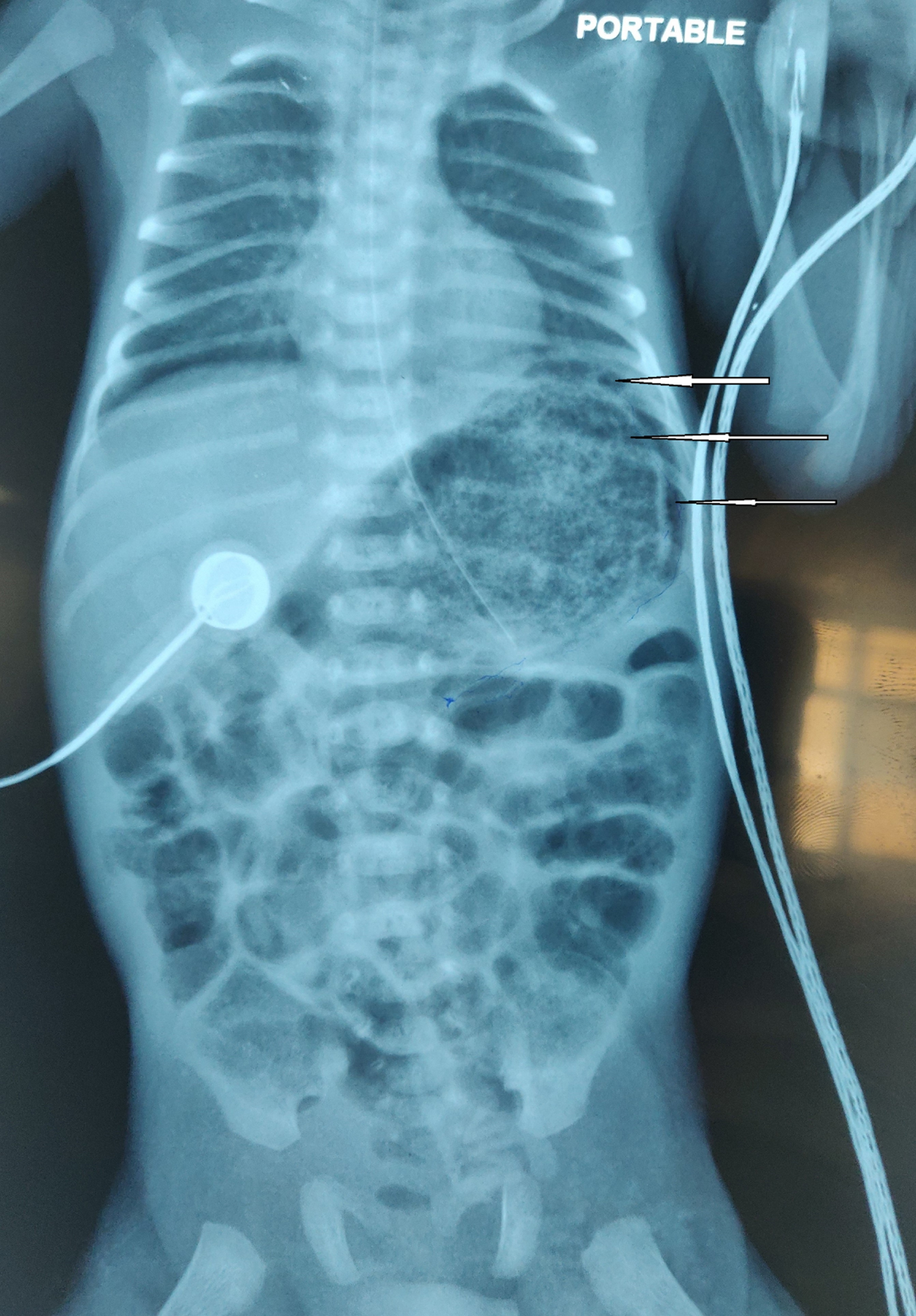
Showing intramural gas shadows, best seen around fundus and greater curvature.
Meanwhile, the initial blood culture had grown methicillin-resistant staphylococcus aureus which was sensitive to Vancomycin and Gentamycin, and so the antibiotics were modified accordingly. Improvement was noted after two days’ administration of these culture-sensitive antibiotics. The baby became hemodynamically stable, and so inotropic support was withdrawn and OG feeding restarted. Full feeds were gradually established and the antibiotics given for 14 days. Twin B’s blood culture had become sterile, and the baby was hemodynamically stable and on Katori spoon feeds at time of discharge on day 19 of life.
EG is a potentially fatal condition diagnosed on basis of radiological evidence. The clinical findings in newborns are non-specific. Abdominal distension, vomiting and increased residual volumes in stomach, the markers of feed intolerance are the only clinical features. The presence of gas specifically in the stomach wall is found in both emphysematous gastritis as well as gastric emphysema with these two conditions presenting similarly in radiological terms but differently in clinical presentation, management, and prognosis. Gastric emphysema is a benign, self-limiting condition while emphysematous gastritis has a high mortality rate of between 30 and 40% [3]. In the case report published in 1978 [4], three infants with pyloric stenosis had developed gastric emphysema, having linear gas collection limited to gastric wall. This type of gas collection has been reported with gastric or duodenal obstruction and is different from the bubbly clusters of gas seen in emphysematous gastritis. While gastric emphysema generally results from mucosal trauma, repetitive vomiting, nasogastric tubes, gastric volvulus, and superior mesenteric artery syndrome, emphysematous gastritis is an extremely rare condition arising from infection by gas-forming organisms. The most commonly associated organism species are Streptococcus, Enterobacter, Clostridium, Candida, and Mucor as well as Escherichia coli, Pseudomonas aeruginosa, and Staphylococcus aureus [5] and the key predisposing factor being immunocompromised. Preterm newborns are considered immunocompromised. As is observed with necrotizing enterocolitis (NEC), a more commonly encountered pediatric surgical condition, prematurity and severe sepsis in newborns are likely to be the risk factors for emphysematous gastritis too and it can happen even in absence of NEC.
Figure 1 illustrates a gas shadow along the greater curvature of the stomach wall near the fundus. This is in line with existing literature which describes the hallmark radiological changes of emphysematous gastritis as thickening of the gastric wall and the presence of irregular gas shadows in the stomach wall, particularly in the fundus and greater curvature [6]. As evident from the systemic review by Watson et al. more timely diagnosis and better medical management with appropriate antibiotics has reduced the mortality to 33% which was 60% earlier, before year 2000. Prompt management also reduced the need of exploratory laparotomies to 22% as compared to 62% during pre 2000 era and thus significantly improved the outcomes [7]. The treatment includes suspending feeding and keeping the babies nil orally, Intravenous fluids, appropriate antibiotics and proton pump inhibitors [8].
To our knowledge, emphysematous gastritis in a newborn has not been previously reported. Is it very rare or do we just miss it?