
Abstract
BACKGROUND:
Recent in vitro testing of high frequency (HF) oscillation applied to bubble continuous positive airway pressure (BCPAP) using a novel flow interrupter device (HFI) demonstrated significantly improved CO2 washout while not altering delivered mean airway pressure (MAP) in a premature infant lung model. This study’s aim was to evaluate the safety and efficacy of the HFI paired with BCPAP in an animal model of prematurity prior to clinical testing.
DESIGN/METHODS:
Twelve fetal lambs, 131–135 days gestation, weight 3.51±0.42 kg, were delivered by Cesarean section. The lambs were supported by mechanical ventilation and weaned to spontaneous breathing with BCPAP at 6 cmH2O. A combined CO2/airflow sensor measured end-tidal (EtCO2) and tidal volume (VT). Blood gases, heart rate (HR), arterial pressure (Part), minute ventilation (MV), MAP, ventilatory efficiency index (VEI), thoracoabdominal phase angle and labored breathing index (LBI) were recorded over a 10-minute baseline period followed by four randomized 10-minute intervals with HFI set to either 8, 10, 12 or 15 Hz.
RESULTS:
EtCO2 decreased from baseline by 11.1±2.2SE%, 16.6±4.3SE%, 13.5±4.9SE%, and 19.5±4.5SE% at 8, 10, 12, and 15 Hz respectively (p < 0.001). Blood gases, SpO2, HR, Part, MAP, VT, MV, esophageal pressure, phase angle, and LBI underwent no significant change with HF. Respiratory rate decreased, and VEI increased, by 14.9±4.5SD% (p = 0.037) and 83±22SD% (p < 0.011) respectively, averaged over all frequencies.
CONCLUSIONS:
We demonstrated the safety and efficacy of a novel BCPAP flow interrupter device. HF applied to the respiratory system resulted in significantly improved CO2 clearance and ventilation efficiency with no deleterious physiological effects in a pre-term lamb model.
Introduction
We recently demonstrated the ability of superimposed high frequency (HF) oscillations to improve carbon dioxide clearance when paired with continuous positive airway pressure (CPAP) and heated and humidified high flow nasal cannula (HFNC) in an in-vitro model [1–3]. This was achieved using a simple, but novel, high frequency flow-interrupter device (HFI) placed in line with delivered gas flow [4, 5]. We also observed an additive effect in a bubble CPAP (BCPAP) system when the frequency of applied oscillations was in the frequency range of the random pressure oscillations caused by the bubbling. Using end-tidal carbon dioxide (EtCO2) level as an index of carbon dioxide clearance, EtCO2 decreased by 18% to 47% when the HFI was placed in the inspiratory limb of a BCPAP system connected to an in vitro lung model of a premature infant [2]. We have also shown in bench studies that while superimposed oscillations increased the amplitude of pressure swings in a BCPAP system, there was only a negligible effect on delivered mean airway pressure (MAP) [6].
The objective of the current investigation was to evaluate the safety and efficacy of our novel device in an animal model of prematurity prior to clinical testing. For this purpose, we measured clinically relevant, non-invasive and readily obtainable physiologic outcome markers of gas exchange and respiratory effort. Specifically, we measured EtCO2 levels, airway pressures and breathing effort while monitoring the hemodynamic response in premature lambs while receiving BCPAP with and without superimposed HF oscillations created with a flow-interrupter device.
Materials and methods
Animal Preparation and Protocol
All animals were managed according to the NIH regulations Guide for the Care and Use of Laboratory Animals. In addition, the Institutional Animal Care and Use Committee of Temple University approved all procedures. Following Cesarean section of the pregnant ewe (131–135 days gestation) and local anesthesia (subcutaneous 1 mL, 0.5% lidocaine HCL in ventral neck) of the fetal lambs (n = 12), the lambs were instrumented with an endotracheal tube by tracheotomy (approximately 5 cm from the cricoid cartilage; 3.0–3.5 mm ID Hi-Lo Jet Tube: Mallincrodkt, Saint Louis, MO, USA), and carotid and venous catheters were placed. After the umbilical cord was cut, the premature lamb was dried, weighed, and supported with volume targeted mechanical ventilation (Dräger Babylog 8000-plus, Dräger Inc., Lübeck, Germany) and gradually weaned within 4 hours to spontaneous breathing with CPAP support with warmed (37°C) and humidified gas to maintain SpO2 > 85%. Airway pressure was monitored at the ventilator wye connector. An air-filled esophageal balloon (Mallinckrodt, 8 French, St. Louis, MO, USA) catheter was positioned in the distal esophagus by advancing the balloon intragastrically as confirmed by positive pressure deflection during inspiration. The catheter was then withdrawn to clear the sphincter and was positioned in the distal esophagus as confirmed by negative pressure deflection during inspiration. Adjustments of balloon placement and inflation were performed to obtain pressure waves that were free of cardiac artifact and the catheter was secured at the mouth. Maintenance fluid was provided by a continuous venous infusion of 5% dextrose at a rate of 6 mL/kg/h. Electrocardiogram electrodes were placed and a rectal temperature probe inserted for monitoring. The animal’s rectal temperature was maintained within 37°C and 38°C through thermal support provided by an overhead radiant warmer (Babytherm 8004; Dräger Inc., Lübeck, Germany) and the lamb was covered with a plastic blanket to minimize insensible water loss.
After initial stabilization and transition to spontaneous breathing with CPAP support, the lambs were switched to BCPAP. BCPAP was applied using a Fisher & Paykel BC163 system (Fisher & Paykel Healthcare Ltd, Auckland, NZ) through an endotracheal wye adapter and maintained at 6 cmH2O throughout the entire protocol. Supply flow for the BCPAP was fixed at the manufacturer recommended 7 L/min for all measurements. After an initial 10-minute baseline period, the flow interrupter was activated to operate for four consecutive 10-minute intervals, each at an oscillation frequency of either 8, 10, 12 or 15 Hz in a random sequence. Blood gases were drawn during the final one minute of each 10-minute interval. At the end of the protocol, the animals were sedated and then euthanized.
Instrumentation for In-Line High Frequency Interrupter for use with Bubble CPAP
As previously described, we used our custom-designed HF flow interrupter that consists of a solenoid-operated pinch valve module and a remotely placed frequency controller/amplifier as illustrated in Fig. 1 [3]. The pinch valve was placed in-series at the midway point of the inspiratory limb of the Fisher & Paykel BCPAP setup. The pinch valve is normally-open in the unpowered state which allows airflow through silicon tubing having a 4.8 mm inside diameter. The frequency controller was set to generate a square wave with a 40% on-off duty cycle for all frequency settings. Carbon dioxide was measured at the tracheal connection using a Capnostat-5 mainstream infrared absorption spectroscopy CO2 sensor mounted on a neonatal sized 15mm endotracheal tube adaptor. The sensor head (< 1 cc dead space) is a combined detector which simultaneously measures CO2 concentration and airflow at the exact same tubing location (Respironics NM3 monitor, Phillips Corp., Wallingford, CT, USA). The continuous airflow signal was digitally integrated to provide the tidal volume recording. Arterial blood specimens were analyzed for pH, PaCO2 and PaO2 (Radiometer ABL330, Radiometer Copenhagen, Denmark). Blood pressures and esophageal catheter pressures were monitored continuously with Statham P23D pressure transducers. Airway pressure was measured at the tracheal connection using a Transpac IV transducer (ICU Medical, Inc. San Clemente, CA, USA). Blood SpO2 was continuously monitored caudally by a Nellcor pulse oximeter (model N100C, Medtronic Inc, Minneapolis, MN, USA). Rib cage and abdominal excursions were recorded with a Respitrace QDC monitor (Viasys Healthcare Inc., Yorba Linda, CA, USA). Rib cage and abdominal excursions were post-processed to compute minute-by-minute mean values of the rib cage-to-abdominal phase angle and labored breathing index (LBI). The Respitrace device was operated in DC mode to enable tracking of changes in expiratory lung volume and is reported as a dimensionless variable. The ventilatory efficiency index (VEI) was calculated as:
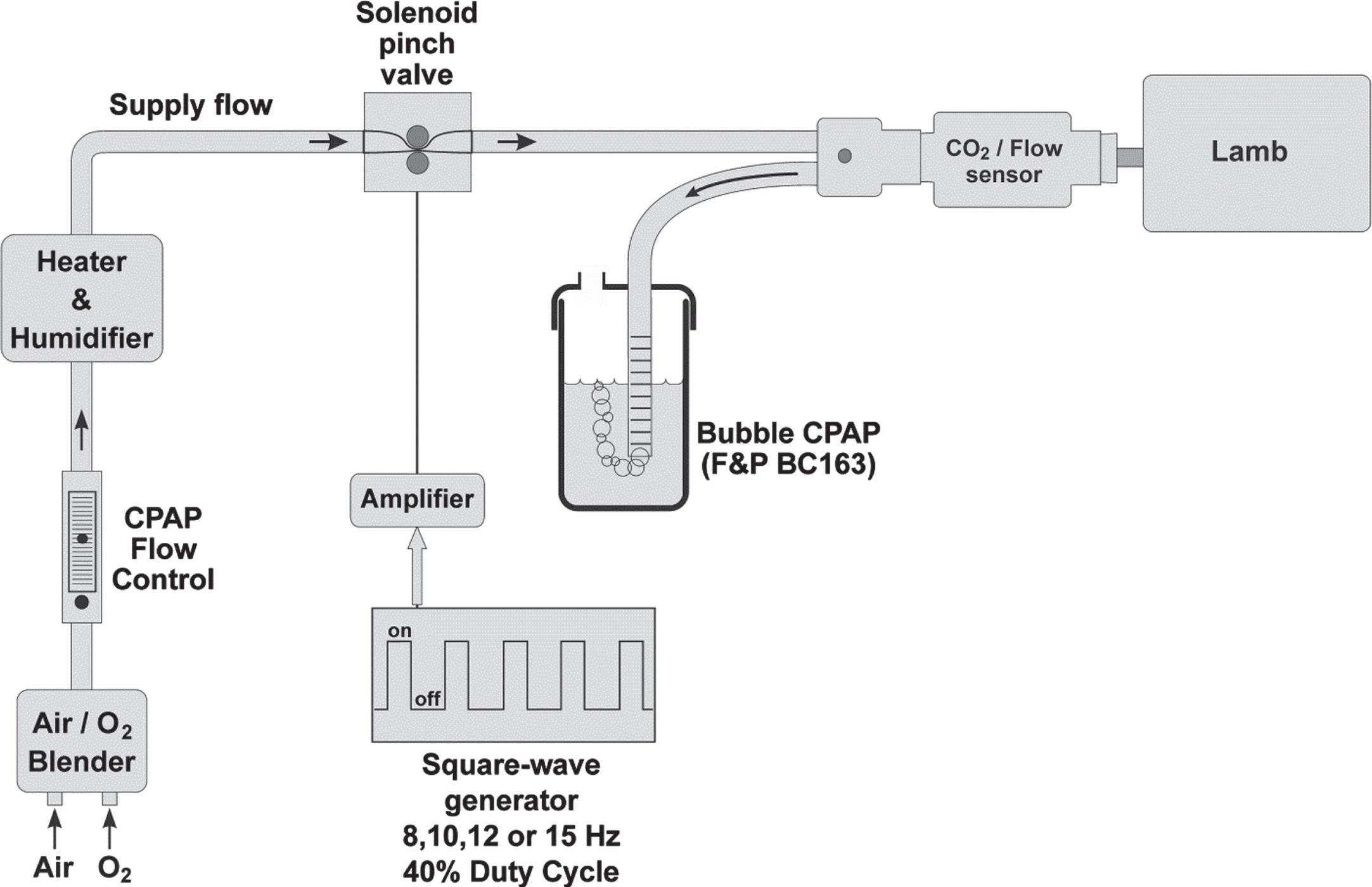
Schematic of the HFI and BCPAP system configuration.
where 3800 is a constant representing CO2 production; ΔP is the peak-to-peak difference in esophageal pressure and used as a surrogate for spontaneous breathing driving pressure in mmHg; F is the breathing frequency in breaths/min; and PEtCO2 is the end-tidal carbon dioxide partial pressure in mmHg [7, 8]. VEI has units of mL·mmHg–1 ·kg–1, however, it is conventionally accepted as a dimensionless index. End-tidal CO2 values were measured at the end-expiratory plateau portion of the capnometer CO2 signal (see Fig. 2) by an automated peak-detector algorithm and averaged over the last one minute of each 10-minute recording interval. Mixed expired CO2 was calculated as the area under the expiratory fractional CO2 concentration vs. volume curve computed for each breath analogous to what has been described for mixed expired nitrogen determinations [9]:
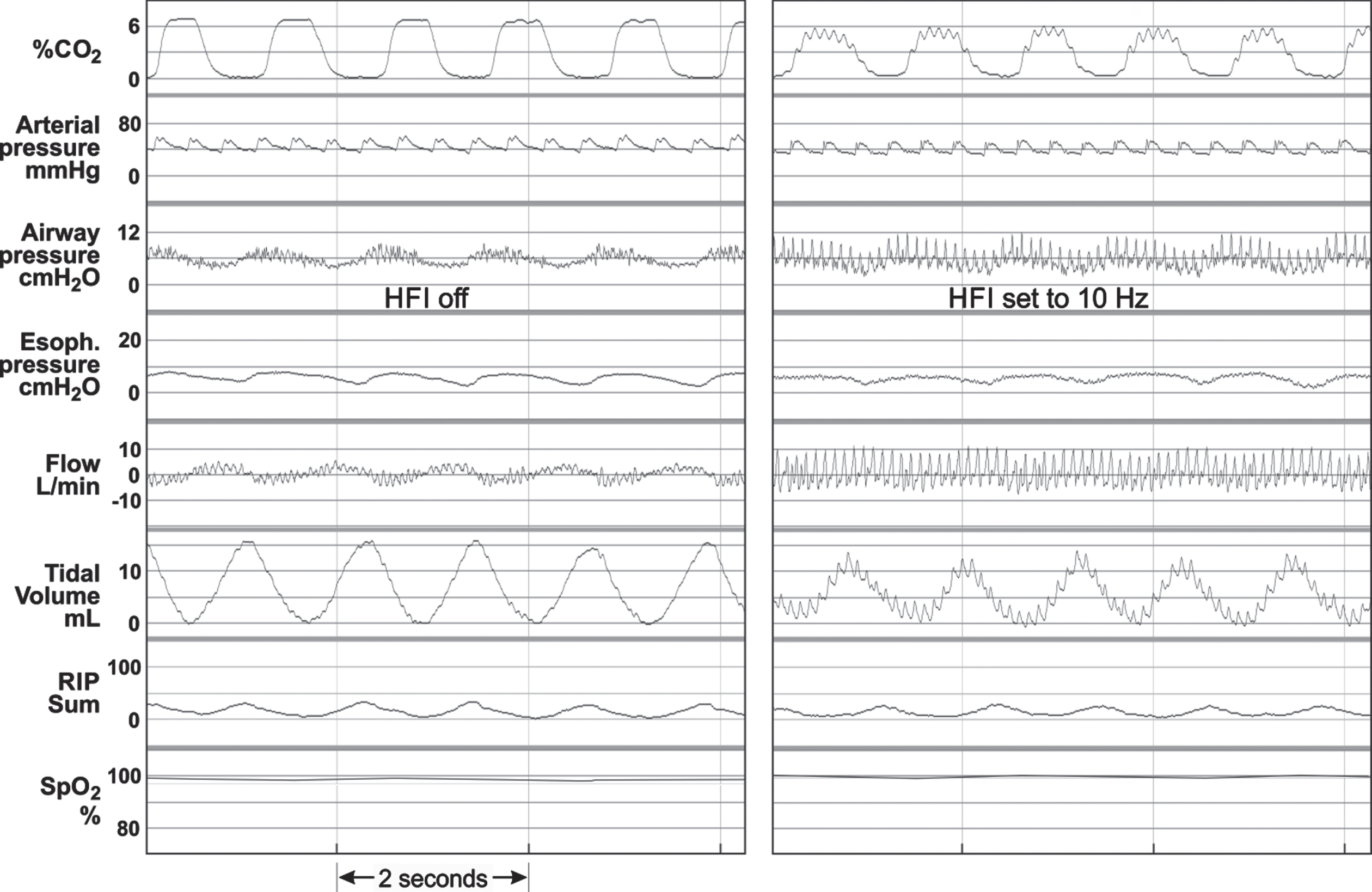
Real time tracings of physiologic parameters with HFI off (0 Hz) and when operating at 10 Hz. RIP Sum: Respiratory Impedance Plethysmograph sum of ribcage and abdominal excursions (arbitrary units).
where
Pressures were calibrated before each recording session using a digital manometer (range: ±259mmHg, ±0.05% NIST accuracy, Additel Corp., Brea, CA, USA). The flow sensor was calibrated using a precision rotameter (range ±9 L/min, ±1% accuracy, Aalborg Instruments, Orangeburg, NY, USA). The capnometer was calibrated with a gas mixture consisting of 5.0±0.1% CO2, 54.0% O2, balance N2O, GE Healthcare, Chicago, IL, USA).
All analog signals were interfaced to an Iworx IX-228 digital recording system using LabScribe v2.0 software and digitized at 200 Hz and 16 bit resolution (Iworx Systems Inc., Dover, NH, USA).
The Kolmogorov-Smirnov test was used to test for data distribution normality. For normally distributed data, the effect of HF on physiologic variables was assessed by repeated measures ANOVA across the different frequency levels. For non-normally distributed data, the Friedman test for multiple related samples was used. Post-hoc comparisons between baseline and each of the applied frequencies were done using Student’s paired-T tests for the normally distributed data and Wilcoxon signed-rank tests for nonparametric data. A p-value of < 0.05 was considered indicative of statistical significance. Statistical software used was SPSS version 19 (IBM SPSS Statistics, IBM Corp. Armonk, NY, USA).
Results
Table 1 lists characteristics of the study lambs after delivery. Figure 2 depicts a sample recording of selected physiologic variables during the baseline period (HFI off) and with the HFI activated and oscillating at 10 Hz. The effect of the HF oscillations can be observed on the carbon dioxide, airway pressure, flow, and tidal volume signals; there were negligible observable oscillations superimposed on the blood pressure and esophageal pressure signals. Table 2 lists the measured and calculated physiologic variables during the initial 10-minute non-oscillated baseline period and for each of the subsequent 10-minute periods during which the flow interrupter was operating at frequencies of 8, 10, 12 and 15 Hz. From a repeated measures analysis which included baseline (0 Hz) and each of the four applied frequencies, EtCO2 values demonstrated a significant decrease associated with HF (p < 0.001); also shown in the table are the average within-subject percent changes in EtCO2 on transition from baseline to each of the HFI frequency settings. Mixed-expired CO2 followed a decreasing trend similar to the decreased end-tidal values, with both parameters having the largest reduction at 15 Hz. In contrast to the EtCO2 values, blood gases demonstrated no significant change from baseline when high frequency was applied, except for a notable small improvement in PaCO2 at 15 Hz. Physiologic dead space, as calculated from mixed-expired and arterial CO2 levels, likewise did not change from baseline to HF. Median and interquartile ranges for SpO2 and heart rate experienced negligible change during HF and the mean systemic arterial pressure remained within 4 mmHg throughout the protocol. Respiratory rate during HF demonstrated a significant (p = 0.037) overall 14.9±4.5SD% decrease from baseline, the largest decrease occurring at 15 Hz. Tidal volume did not change appreciably during HF and remained within 0.3 mL/kg of the baseline 4.0 mL/kg; and likewise minute ventilation also remained unchanged during the entire protocol.
Lamb characteristics (n = 12)
Lamb characteristics (n = 12)
Summarized measured and calculated physiologic variables during the 10-minute non-oscillated baseline period and for each of the 10-minute periods at frequencies of 8, 10, 12 and 15 Hz
Data shown as Mean±standard deviation (SD) or Median (interquartile range). SE: standard error of the mean. *p-value by repeated measures ANOVA or †Friedman test, on 0, 8, 10, 12 and 15 Hz. **by paired–T test. ††Wilcoxon signed-rank test.
The mean airway pressure, as measured after low-pass filtering, remained within the range of 6.4 to 6.8 cmH2O during both the baseline period and all HF settings. The mean delivered peak-to-trough amplitude of the airway pressure, however, was 5.3 cmH2O during baseline, due to the BCPAP bubbling alone, and increased to a mean of 15.0±7.3SD cmH2O (p < 0.001) averaged over all the HF settings; and this pressure amplitude was significantly less (p < 0.001) at 15 Hz (11.7±5.5SD cmH2O) compared to 12 Hz (16.0±8.4SD cmH2O). Esophageal pressure excursions exhibited large variations among the lambs but the median peak-to-trough values during any of the HF settings was not significantly different than the baseline value and with negligible HF transmission onto the pressure waveform as exemplified in the tracing in Fig. 2.
Values of the ventilation efficiency index were higher (p = 0.011) at all levels of HF relative to the baseline median value of 0.28, as shown in Table 2. Also shown in the table are the average within-subject percent changes from baseline at each frequency and the respective post-hoc p-values for each set of paired values.
RIP measurements of thoracoabdominal asynchrony, as measured by the rib cage-to-abdominal phase angle, although trending higher relative to baseline, did not result in any statistically significant changes due to the large variability in this parameter during HF. Similarly, the labored breathing index (LBI) also exhibited negligible change in transition from baseline to HF. Interestingly, the RIP sum signal (rib cage + abdomen), as an indirect measure of changes in lung volume, remained relatively constant during the entire protocol.
Current lung protection strategies for preterm infants include utilization of non-invasive respiratory support to avoid more invasive methods requiring intubation and mechanical ventilation. Nasal CPAP, in particular, continues to be a first choice by clinicians to help reduce the risk of ventilator induced lung injury [10]. However, CPAP failure rates continue to be near 50%, particularly in extremely low birth weight infants [11]. Several investigations have attempted to improve basic CPAP technology to improve its success [12–14]. Toward this end, we developed our simple flow interrupter device (HFI) for superimposing high frequency oscillation onto the delivered pressure of a basic bubble CPAP delivery system.
In this pre-term lamb model we demonstrated that transition to HF oscillation was well tolerated by all of the study lambs. Whereas blood gases and acid-base parameters showed large biologic variability, there was no overall significant change from the non-oscillation baseline. There was no evidence of intrathoracic transmission of HF oscillations on central hemodynamics as reflected by stability of arterial blood pressure recordings, again demonstrating tolerance to methodology and importantly, safety, by protecting the delicate cerebral circulation from unwanted pressure swings. Other important physiologic parameters such as oxygen saturation, heart rate, tidal volume and minute ventilation also were shown to have been minimally affected by the HF oscillations. Airway pressure oscillations produced by the HFI device had amplitudes ranging from 12 to 16 cmH2O, extending both above and below the mean baseline level during HF resulting in a negligible net change from the baseline level and thus the delivered mean airway pressure remained remarkably constant and close to the baseline 6.4±1.6SD cmH2O with a variation of only one-half of one cmH2O. This is because the HFI is a passive device having no pressure generating component. The HFI pressure oscillations are due primarily to pressure accumulation and release in the compliant corrugated tubing in the BCPAP circuit as the interrupter valve closes and opens, as described by Rub et al in a recent in vitro study implementing this device [15]. In addition, from Table 2 the greatest reductions in EtCO2 occur between 10 and 15 Hz and correspond to the frequency range where the frequency power spectrum of the random bubble oscillations created by BCPAP has the highest dominant peak power [3].
The HFI-augmented CPAP resulted in changes in carbon dioxide, recapitulating results found in our in vitro model. Specifically, with applied high frequency oscillation, EtCO2 levels exhibited an overall decrease of 15% which is in the range of the 14% to 19% change measured in our in vitro model of abnormal and normal lung mechanics, respectively [3]. Interestingly, the higher EtCO2 relative to PaCO2 values at baseline and at 15 Hz was an unexpected result. This not uncommon phenomenon was described previously by Fletcher et al., and further elaborated on by Ickx et al., as being associated with, among other factors, a reduced respiratory rate [16, 17], which was also seen in the present study. We speculate that there are several experimental design limitations that could have contributed to this observation. Lambs were intubated, therefore partially reducing the HF carbon dioxide washout effect from the upper airways. In addition, the test interval duration might not have been long enough to detect maximum effect or potential long term improvement due to HF. It is also likely that the observed uncoupling between EtCO2 and PaCO2 reflects a salutatory effect of HF oscillations to improve overall ventilation: perfusion matching, specifically by increasing the ventilation of the dependent low V/Q alveoli.
The reduction in respiratory rate, EtCO2, and lower minute ventilation that contributed to a significant average increase of 83% (p = 0.011) in paired measurements of ventilation efficiency index (VEI), suggests improved efficiency of carbon dioxide elimination for reduced work of breathing. Further, the combination of reduced respiratory rate and work of breathing, supports reduced power of breathing, which could have additional beneficial effects, especially in the preterm infant.
In summary, in this first in vivo proof of concept study, we have demonstrated the safety and efficacy of a novel, but simple, BCPAP flow interrupter device. Application of high frequency oscillation to the respiratory system resulted in significantly improved carbon dioxide clearance and ventilation efficiency with no deleterious physiological effects in a pre-term lamb model. This novel approach holds promise as a tool to improve non-invasive respiratory support in the Newborn Intensive Care Unit.
Footnotes
Acknowledgments
The authors gratefully acknowledge Jacqueline Lynch, MLAS for assistance with animal preparation and monitoring.
Disclosures
The authors have no financial relationships or conflicts of interest to disclose concerning the contents of this article.