
Abstract
OBJECTIVE:
To validate the vasoactive inotropic score as a predictor of the severity of compromised systemic circulation and mortality in preterm infants.
METHODS:
A retrospective study was conducted on preterm infants with Compromised systemic circulation [hypotension±lactic acidosis±oliguria] who received a cardiovascular support, we calculated the vasoactive inotropic score (VIS) and cumulative exposure to cardiovascular medications over time (VISct). Receiver operator curve was constructed to predict the primary outcome which was death & refractory hypotension.
RESULTS:
VIS had an area under the curve of 0.73 (95% CI 0.85–0.98, p < 0.001). A VIS cut off of 25 has sensitivity and specificity of 66% and 92%, and positive and negative predictive values of 78.5% and 83%, respectively.
CONCLUSION:
High VIS predicts the severity of Compromised systemic circulation and mortality rate in preterm infants.
Keywords
Abbreviations
Compromised systemic circulation
Intraventricular hemorrhage
Mean arterial blood pressure
Necrotizing enterocolitis
Vasoactive inotropic score
Vasoactive inotropic score with cumulative time of exposure to cardiovascular medication
Introduction
Management of hypotension is an unresolved challenge to neonatal intensive care practitioners [1]. The concern about hypotension in preterm infants and the main rationale of neonatologists to treat the detrimental effect on end-organ perfusion [2]. Hypotension has been associated with several adverse effects that reflect the cardiovascular instability and end-organ injury; the most common detrimental short term clinical consequences are intraventricular hemorrhage (IVH) and periventricular leukomalacia, necrotizing enterocolitis (NEC), and finally death [3]. It has been reported that 16–98 % of preterm infants receive cardiovascular medications during admission [4].
Compromised systemic circulation [CSC] was considered present if the infant had hypotension±one or more of the following: oliguria < 1 ml/kg/hour for at least 12 hours beyond the first postnatal 12 hours, or lactic acid > 2.8 mmol/dl will probably have a high mortality. We hypothesized that a preterm infant with Compromised systemic circulation unresponsive to a certain dose of a cardiovascular drug as represented by the vasoactive inotropic score (VIS) can represent a marker at which the treating team should reassess the management strategy rather than continuing to escalate the cardiovascular medication dosage or adding more medications in the absence of clinical improvement. Blood pressure has never been proven to be a sensitive marker reflective of end organ blood flow, especially when relying solely on mean blood pressure (MABP) and ignoring the physiologic values of systolic and diastolic blood pressures [5, 6]. VIS may be useful as an independent predictor of poor short-term outcome after cardiothoracic surgery in neonatal population [7, 8] and predicts eventual morbidity and mortality in post-operative congenital heart surgery with cardiopulmonary bypass [9]. The aim of this study was to validate the value of VIS for prediction of the severity of Compromised systemic circulation and mortality in preterm infants < 33 weeks. We hypothesized that a higher VIS score would be associated with high mortality in preterm infants < 33 weeks gestation.
Methods
All infants who were admitted to the 2 tertiary NICUs in Winnipeg, Canada between 2011–2015 who received cardiovascular medications were identified using pharmacy’s electronic records. Preterm infants < 33 weeks were identified and a retrospective chart review was undertaken. Elligibility criteria was premature babies < 33 weeks who had clinical evidence of compromised systemic circulation with at least one of the following: low mean arterial blood pressure (MABP) as defined by less than the lower 95% confidence interval (CI) for the corrected gestational age with considering invasive BP measurement as the standard monitoring, oliguria less than 1 mL/kg/h for at least 12 hours, or lactic acidosis greater than 2.8 mmol/l, and received cardiovascular medication [1, 10]. Infants with congenital or chromosomal anomalies were excluded. In this study we calculated the (VIS) as follows [Dopamine (mcg/kg/min) + Dobutamine (mcg/kg/min) + Epinephrine (mcg/kg/min)×100 + Norepinephrine (mcg/kg/min)×100 + Vasopressin (IU/kg/min)×10000 +Milrinone (mcg/kg/min)×10] [7, 9]. We considered the highest dose for each drug if continued for > 6 hours. We calculated the cumulative vasoactive inotropic (VISct) exposure to the cardiovascular medications by multiplying the (VIS) of each drug with the exposure time in hours. Demographic and clinical data were abstracted from the chart review. Those data included antenatal steroids, gestational age (GA), birth weight, sex, Apgar scores at 5 and 10 minutes, confirmed sepsis, and IVH. The cumulative time of compromised systemic circulation (CSC) during NICU admission was considered as marker of disease severity. CSC was considered present if the infant had hypotension as described above±one or more of the following: oliguria < 1 ml/kg/hour for at least 12 hours beyond the first postnatal 12 hours, or lactic acid > 2.8 mmol/dl [5, 6]. The study period was before the targeted neonatal echocardiography was introduced in our units as a standared of care for assessment of infants with refractory hypotension; the cardiovasculr medications were prescribed empirically starting with dopamine with the addition of dobutamine, epinephrine, norepinephrine, vasopressin and milrinone as second or third line (Table 3), plus the administration of multiple empirical normal saline boluses. Our primary outcome was death due to intractable CSC.
Table3
Table3
Dop;dopamine, Dob;dobutamone, Epi;epinephrin, Norepi;norepinephrine, vaso;vasopressin
Ethics approval was obtained from University of Manitoba Research Ethics Board.
SPSS v 24 (SPSS Inc, Chicago, Illinois) was used to perform the statistical analysis. Data are presented as median with interquartile range or frequencies. Comparisons between groups were analyzed by Mann-Whitney U test; Frequencies were analyzed using Chi-square; p < 0.05 was considered significant. The primary outcome for infants with hypotensive shock was evaluated using Cox proportional hazards regression model. A receiver operating characteristic (ROC) curve was constructed, and predictive values were calculated. Pearson correlation was used to correlate VIS ≥25 associated with death with other variables, with relevant graphs created by GraphPad program.
Results
One hundred and seventeen preterm infants < 33 weeks GA who had significant hypotension were enrolled in the study; 38 (32.5%) died and 79 (67.5%) survived. Table 1 showed comparison of the descriptive data between both groups. The groups had similar birth weights and gestational ages. Nine infants presented initially with lactic acidosis, 4 with oliguria and 8 with both, and 96 infants presented initially with hypotension. Infants who died have developed CSC at an earlier postnatal age day 2 (1–8) vs. day 4 (1–14) (p < 0.05), and had a significantly higher VIS (median, IQR): 28 (12, 37) vs. 10 (7, 18) (p < 0.0001) compared to those who recovered. Infant who died also had a higher fraction of inspired oxygen (FIO2) at the time of the highest recorded VIS 0.45 (0.36–0.65) vs. 0.4(0.3–0.5) (p < 0.05) and lower serum cortisol level 294 (196–739) vs. 1640 (383–1750) (p < 0.05), 39 babies received steroids 7 [18% ] of them died, 79 babies didn’t receive 31[39%] of them died.
Descriptive data of the studied groups presented as median (IQR) and percentages, p-value is bold when significant
Descriptive data of the studied groups presented as median (IQR) and percentages, p-value is bold when significant
GA; gestational age, VIS; vasoactive inotropic score, VISct; Cumulative exposure to CVS medications, IVH; Intraventricular hemorrhage
VIS value had an area under the curve of 0.73 (95% CI 0.85–0.98, p < 0.001). A VIS value cut off of ≥25 has sensitivity and specificity of 66% and 92%, and positive and negative predictive values of 78.5% and 83%, respectively, Fig. 1 shows the receiver operator curve.
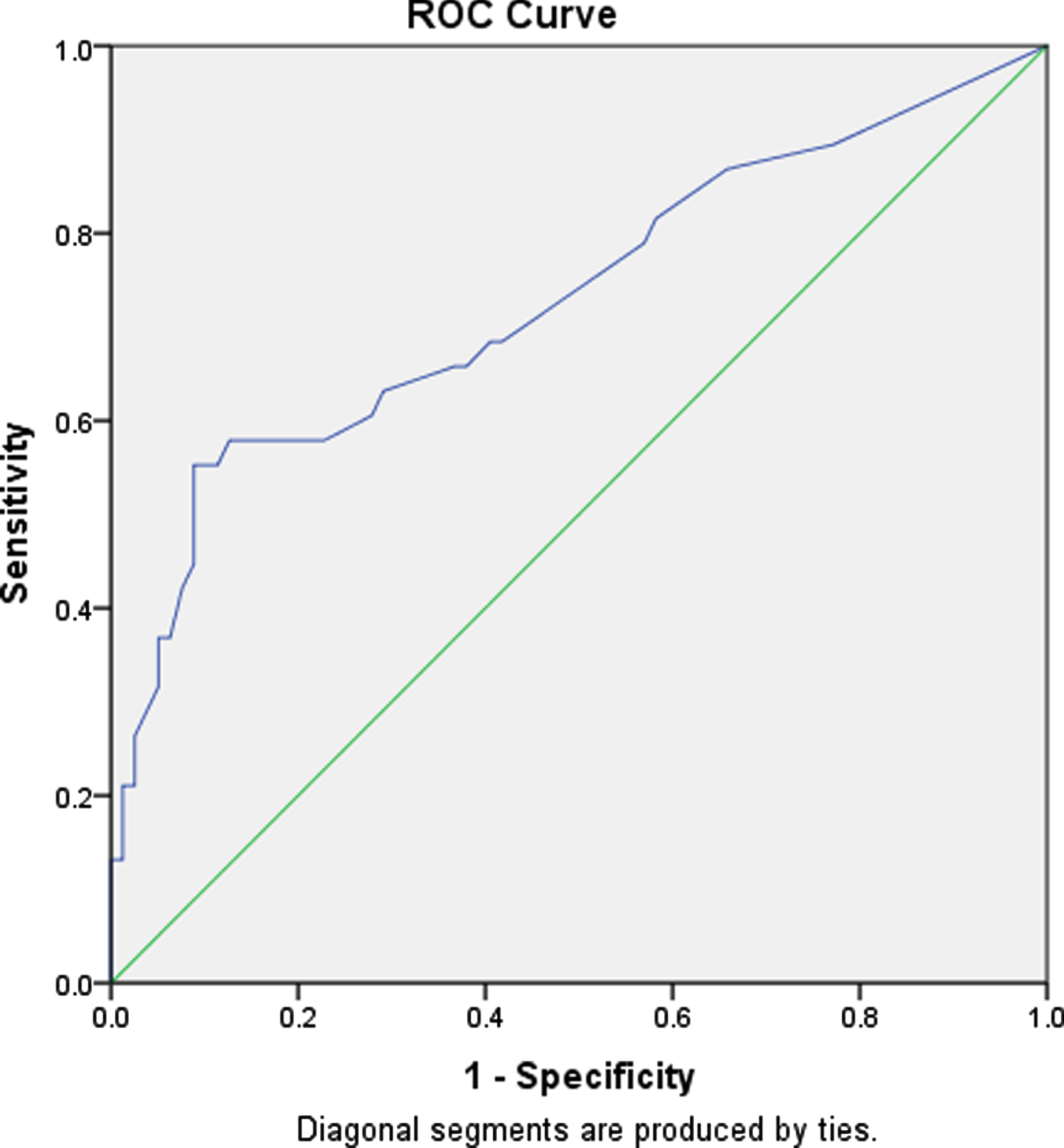
ROC curve of VIS.
Figure 2 shows Cox proportional of death of infants with VIS ≥25 compared to infants with VIS < 25 and in relation to exposure time to cardiovasculr drugs. Table 2 and Fig. 3 show the assoctation beween infants with VIS who either dead or survived with the following variables: Lactic acid, urine output, systolic blood pressure, diastolic blood pressure, mean blood pressures, serum cortisol levels, gestational age, and Apgar scores; there was signifcant correlation with lactic acid, urine output, systolic blood pressure, gestaional age, and serum cortisol level. Higher percent of cases underwent delayed cord claming was assocaited with VIS < 25, which was not the case with the percent of cases with confirmed infection Fig. 4.
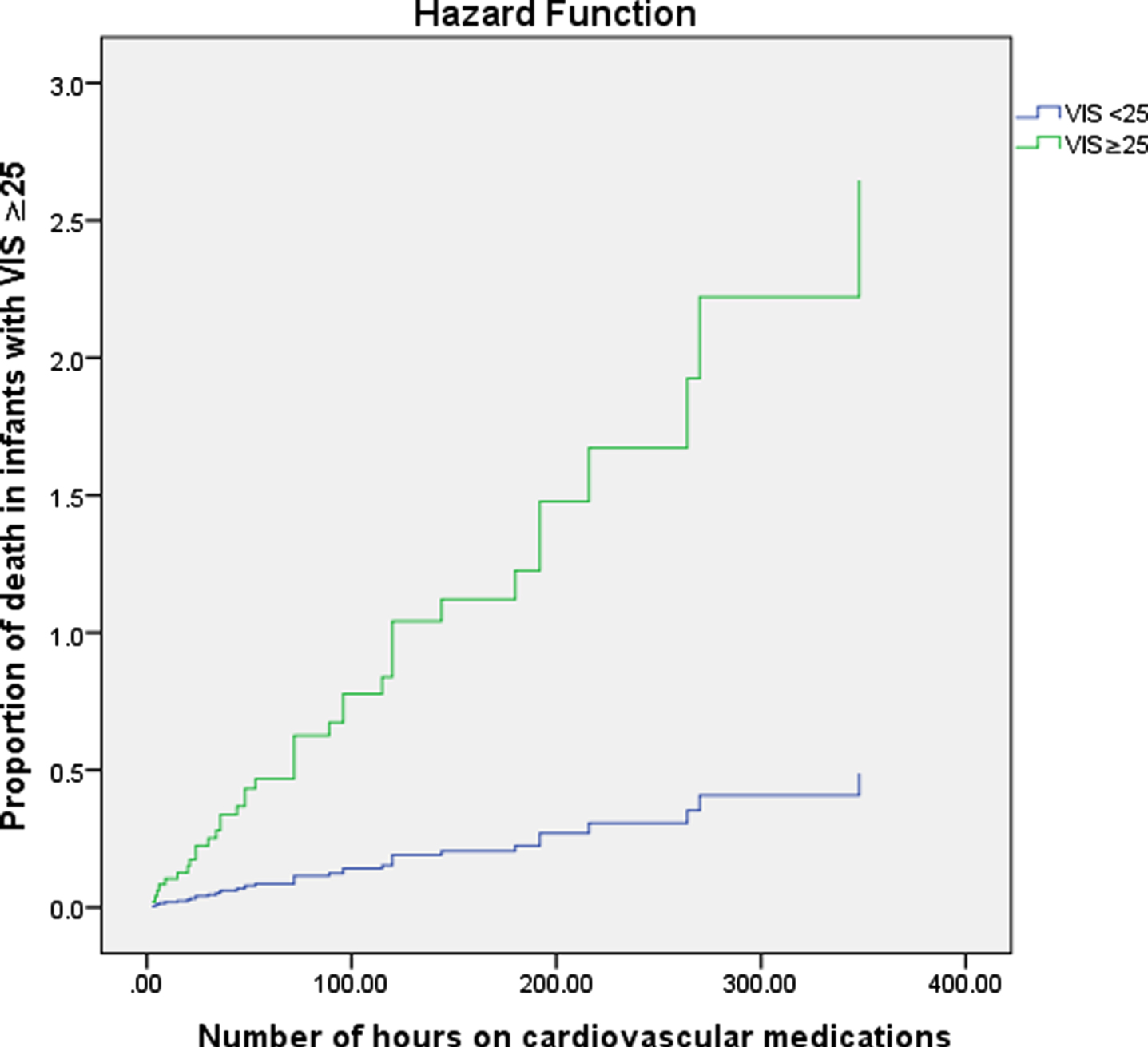
Cox proportional of death of infants with VIS ≥ 25 compared to infants with VIS < 25 and in relation to exposure time to cardiovascular drugs.
Correlation between duration of VIS ≥25 in infants who dead, and physiologic parameters
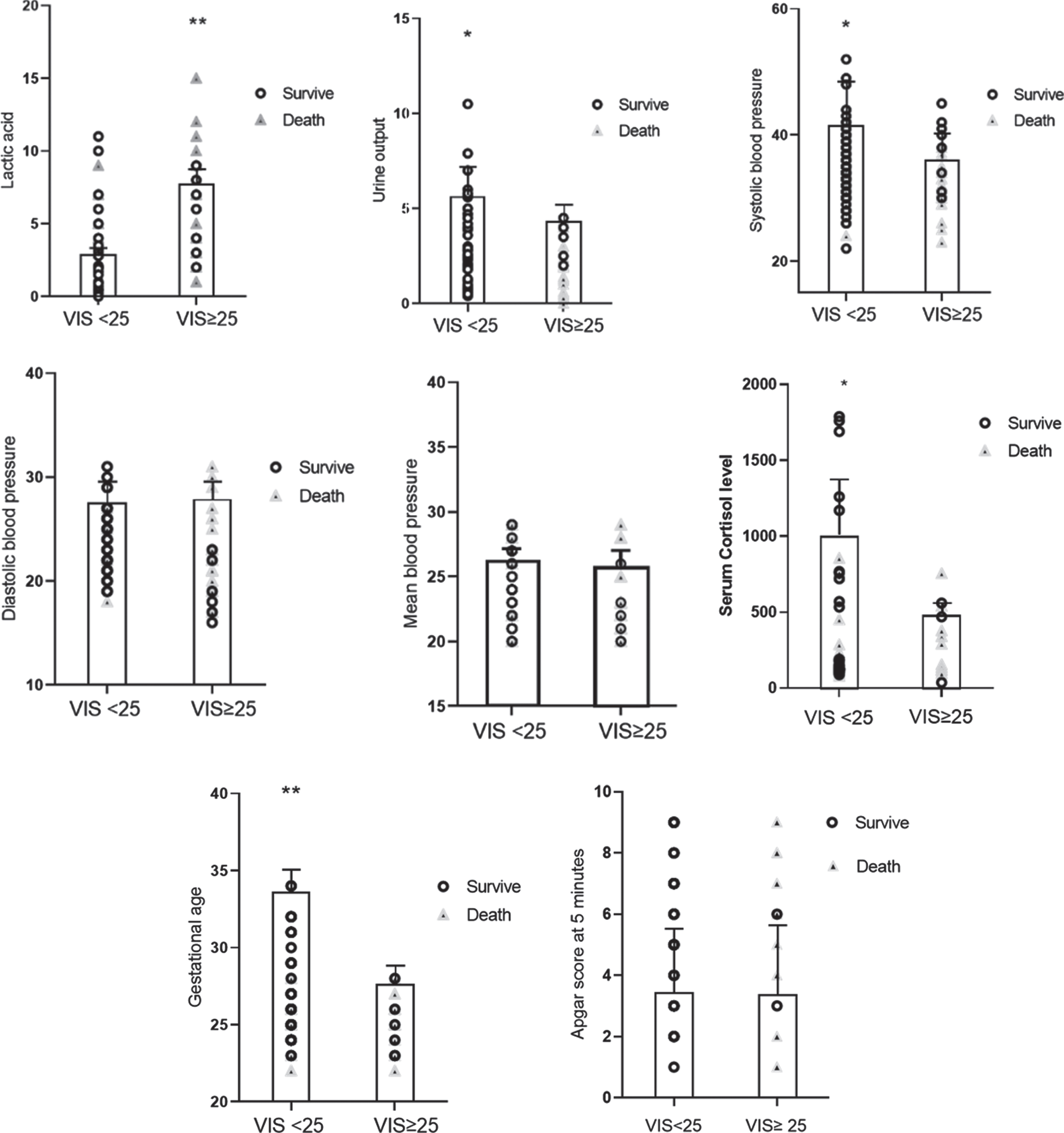
The association between infants with VIS who either dead or survived with the following variables: lactic acid, urine output, systolic blood pressure, diastolic blood pressure, mean blood pressures, serum cortisol levels, gestational age, and Apgar scores, *= p value < 0.05, **= p value < 0.01.
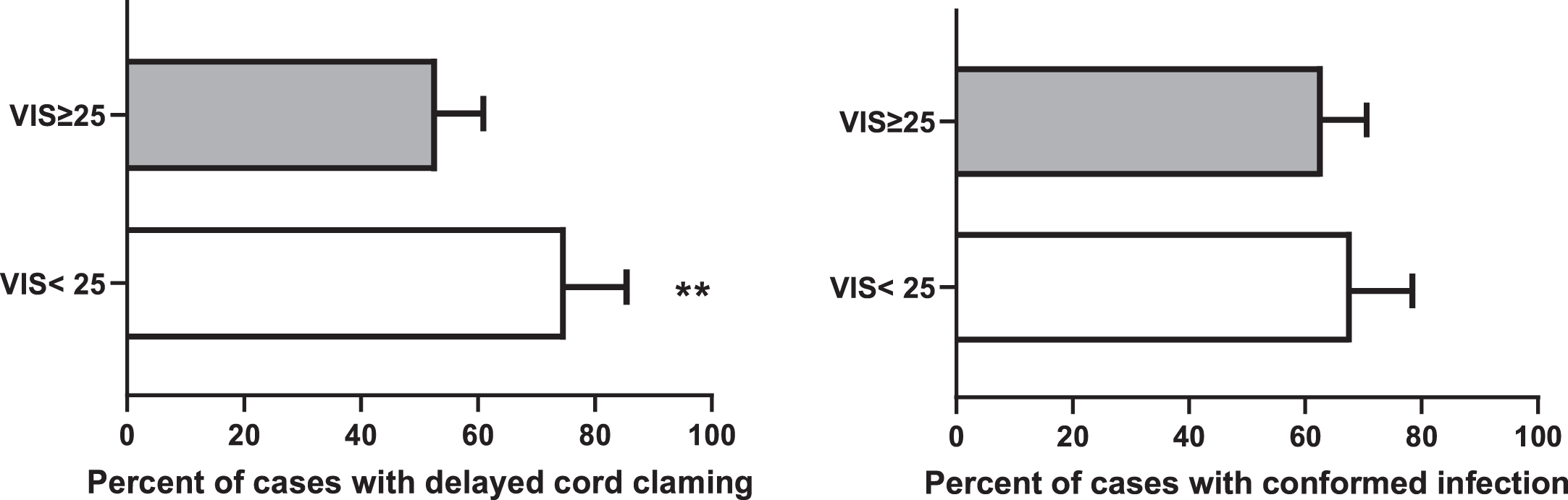
The association between VIS and percent of cases with delayed cord clamping, and conformed infection, **= p value < 0.01.
We have examined the predictive value of the vasoactive inotropic score in preterm infants with CSC aiming to predict intractable hypotension early which might alert the clinical team to consider different management strategy or consider to formulate a physiologic based medical recommendation by utilizing the new emerging techniques like targeted neonatal echocardiography and near infrared spectroscopy as an alternative to empiric approach [5, 11]. This study was conducted before implementing the physiologic based integrated hemodynamic approach, which might explain the high VIS in significant number of cases [5]. The formulated medical recommendation could be either discontinuation of a cardiovascular medication causing side effects more than supporting systemic circulation, or consider more investigations to elucidate the pathophysiologic mechanism [12, 13]. We found that VIS ≥25 was associated with higher mortality in preterm infants with CSC and is an alert number to start considering other modalities of treatment based on further imaging (TNE) Targeted Neonatal Echocardiography to assess underlaying pathophysiologic mechanism [14, 15]. This is the first study to our knowledge describing the value of VIS in this population but it has been validated in older children with shock [(8)].
Current research confirms that the measurement of blood pressure does not reflect either tissue perfusion or oxygen delivery [16, 17], and current therapeutic interventions for hypotension are not associated with improved in-hospital outcomes or neurodevelopmental outcomes [18, 19]. This could be related to lack of insight regarding the significance of physiologic markers which reflect variations in blood flow, together with adopting empirical cardiovascular support without assessment of the underlying pathophysiology [12, 20]. Identifying whether CSC a result of impaired preload, afterload, contractility, or the oxygen-carrying capacity (or a combination of those factors) can facilitate a more targeted and more meaningful approach to management, we analysed the preterm infants with CSC before implementing our hemodynamics protocol, which could explain high VIS in significant number of cases [21, 22]. We reported the impact of integrated evaluation of hemodynamics on clinical outcomes including VIS, and the time to clinical recovery and both were significantly lower in the group managed with the formulated pathophysiologic medical recommendation compared to infants managed with empiric approach [5]. It is not uncommon that in refractory CSC, the number and/or dose of cardiovascular medications is empirically increased. This approach may overlook the detrimental side effect of these drugs, which may increase the risk of death in some situations [5, 6]. VIS has been validated in neonates post cardiothoracic surgery and it was predictive of poor short-term outcomes [7, 23]. The strengths of this study are using the VIS score as a marker of impending and intractable CSC and validating VISct which reflects the impact of the cumulative doses of cardiovascular drugs used before death or discharge. The limitations of this study are small sample size and the retrospective design and the lack of comparison with similar cases managed with physiologic approach.
Conclusion
VIS maybe useful in predicting severity of the CSC and mortality in preterm infants, we found that VIS ≥25 was associated with higher mortality in preterm infants. This is the first study to our knowledge describing the value of VIS in this population.
Funding
No funding was secured for this study.
Conflicts of interest
The authors have no financial relationships to disclose and no conflict of interest.
Ethics approval
Was obtained from University of Manitoba Research Ethics Board.
Consent to participate
It was a retrospective chart review study.
Consent for publication: Obtained and the material is original research, has not been previously published and has not been submitted for publication elsewhere while under consideration.
Availability of data and materials: Available.
Authors’ contributions
Reem Amer: Designed the study, collected the data, wrote the manuscript.
Mary Seshia: Reviewed the manuscript.
Yasser Elsayed: Supervised the protocol design, reviews the statistical analysis, reviewed the manuscript.