
Abstract
BACKGROUND:
This study prospectively investigated the levels of energy metabolism hormones in very preterm neonates to identify their change over time and association with intake of maternal milk as well as weight gain velocity.
METHODS:
We measured and compared the leptin, adiponectin, ghrelin, and insulin-like growth factor I (IGF-1) levels in the urine of 70 very preterm neonates, before the initiation of any enteral feeding (baseline level) and twice within 14 days on full enteral feeding (FEF). Regression models identified the role of intake of maternal milk on the levels of the tested energy metabolism hormones in the enteral-fed infants. We also analyzed the adequacy of the weight gain velocity defined by the fetal-infant growth reference (FIGR). Additionally, we collected and analyzed the infants’ clinical and feeding characteristics during the birth hospitalization.
RESULTS:
The preterm infants’ baseline levels of the energy metabolism hormones significantly predicted their increase at the end of two weeks of observation on FEF. The leptin level was associated with increased intake of maternal milk, whereas the feeding volume was associated with increased ghrelin and IGF-1, and decreased leptin and adiponectin. Infants with comparable FIGR had higher leptin levels than those with inadequate weight gain velocity.
CONCLUSION:
Early postnatal levels of leptin, adiponectin, ghrelin, and IGF-1 predicted the increase of these hormones in the fully enteral fed very preterm neonates. Moreover, greater intake of maternal milk by the study infants contributed to an increased leptin-associated weight gain velocity.
Introduction
The American Academy of Pediatrics recommends the use of appropriately fortified breast milk as a nutritional standard for feeding preterm neonates [1]. The mammary glands function similar to the placenta by providing bioactive components to the maternal milk by diffusion or receptor-mediated mechanisms [2]. There is compelling evidence that maternal milk is an essential source of energy metabolism hormones [3–7]. Among the hormones involved in the energy metabolism processes are leptin, adiponectin, ghrelin, and insulin-like growth factor I (IGF-1) that take part in the regulation of various activities including but not limited to anti-inflammatory and antioxidant [8, 9], homeostasis [2, 10], and the infants’ growth [2, 11]. However, knowledge about the concrete functional role of the energy metabolism hormones in the infant’s growth is incomplete [12]. The existing data comparing the blood levels of energy metabolism hormones of breastmilk-fed to formula-fed infants [13–15] and the infants’ growth [14, 16–19] are inconsistent. It is still not known whether the concentration of the energy metabolism hormones in preterm neonates is associated with the amount of human milk in the infants’ diet. Theoretical and practical aspects of the contribution of human milk to metabolic-functional proteins and their association with infant health outcomes are of growing interest [2]. For instance, identifying the pattern and role of energy metabolism hormones in the growth of preterm neonates is of primary interest because impaired growth increases the risk for preterm birth-associated complications [20].
We designed a prospective cohort study to: (i) outline the alteration of the leptin, adiponectin, ghrelin, and IGF-1 levels in the urine of very preterm neonates, before the initiation of any enteral feeding, and two times during the 14 days on full enteral feeding (FEF), (ii) identify the levels of energy metabolism hormones in association with the proportional intake of maternal milk on FEF, and (iii) assess the role of the energy metabolism hormones in weight gain velocity of the studied very preterm neonates. Although the tested hormones have well-known biological properties, our study will improve the understanding of alterations in the levels of leptin, adiponectin, ghrelin, and IGF-1 and the beneficial role of maternal milk in the metabolic adaptation and growth of very preterm neonates.
Material and methods
We enrolled infants born at a gestational age of 32 and fewer weeks without congenital anomalies and maternal human immunodeficiency virus, to prospectively test the energy metabolism hormones (leptin, adiponectin, ghrelin, and IGF-1) in the first 48 hours of life, before the initiation of any enteral feeding (baseline level), and on day 7 and 14 of FEF. In addition, the following clinical data were collected: gestational age (GA, weeks), birth weight (BW, grams), gender (male, female), morbidities (bronchopulmonary dysplasia, intraventricular hemorrhage of any grade, sepsis), and procedures (blood transfusion, surgery, mechanical ventilation, phototherapy during FEF). The collection of feeding information included the duration (days) on total parenteral nutrition (TPN), day of life (DOL) at the initiation of trophic feeds (TF), weeks of postmenstrual age (PMA) at the achievement of FEF and PMA at day 14 on FEF. Overall daily enteral feeding volume in milliliter (mL), the amount of maternal milk in the daily nutritional intake (mL), method of enteral feeding i.e., whether with or without orogastric (OG) or nasogastric (NG) tubes, and the infant’s daily weight in grams (g) from day 1 to 14 on FEF were collected. We assessed the weight velocity of the infants during the 14 days on FEF by comparing their median daily weight gain in grams per kg with the median fetal-infant growth reference (FIGR) between 23 and 40 weeks of 14.8 g/kg/day [21].
Characteristics of FEF
Feeding related data were collected daily for 14 days after the initiation of FEF. We calculated the percent of maternal milk intake per day (% /d), the feeding volume in milliliter per kilogram per day (mL/kg/d), and caloric intake in kilocalories per kg per day (kcal/kg/d). Fortification of maternal milk to 24 kcal/oz (80 kcal/100 mL) was initiated when enteral intake reached 100 mL/kg/day. During the study period, mother’s own milk and/or preterm formula were the only options for the feeding of the neonates admitted to the neonatal intensive care unit (NICU) at our institution. Donor milk was not available. We used an average caloric content of human milk of 20 kcal/oz (66.7 kcal/100 mL) [22, 23] and 4 kcal/oz (13.3 kcal/100 mL) in one pack of commercial powder fortifier (0.9 g) to calculate the caloric intake. The daily information about the maternal milk intake was utilized to calculate the average proportional intake of maternal milk during the 14 days on full enteral feeds. We used the same classification as in the previous report [24] to categorize the proportion of maternal milk in the diet of the very preterm infants: predominantly exclusively breast fed infant if the mean intake of maternal milk was 85% or more (Group1), partially breastfed if the intake of maternal milk ranged from 35% to 84.9% (Group 2), and predominantly formula-fed if the proportion of maternal milk in the infant’s FEF was 34.9% or less (Group 3).
Urine sample collection and analysis
Urine samples were collected on three separate occasions: (i) within 48 hours after birth (before the initiation of any enteral feeding), (ii) on day 7, and (iii) day 14 of FEF, and correspondingly coded as 1, 2, and 3, in addition to the assigned personal code. Approximately 3 mL of urine was obtained at the three above-mentioned epochs from each enrolled infant by placing cotton gauze pads in the infant’s diaper, transferring urine-soaked gauze pads to 20 mL syringes, and then squeezing out the urine from the gauze pads into preservative-free containers. The time of urine collection was dependent on the infant’s diaper change by the nurse, which was generally within 3 hours after a feed. Collected samples were centrifuged at 2000 g for 5 minutes, aliquoted, and then stored at –80 °C in microplastic containers until further assay. After completing the study enrollment and specimen collection, the aliquoted urine sample were thawed at room temperature and then processed further. The thawed aliquots were not refrozen. The measurement of energy metabolism hormones in the urine has been previously validated [25–28]. Urine specific gravity, which is a measure of the ratio of the density of 1 mL of urine to the density of 1 mL of distilled water, was calculated for each urine sample prior to the enzyme-linked immunosorbent assay (ELISA). The measured specific gravity was used to adjust for differences in the hydration on the obtained energy metabolism hormones levels. The coding of samples and ELISA testing procedure ensured the simultaneous measurement of the three urine samples of each study participant on the same microplate, by a laboratory technician blinded to the infant’s clinical information. The following energy metabolism hormones specific ELIZA kits were used: (i) Human Leptin (R&D Systems, Minneapolis, MN, USA) with assay sensitivity of 0.128 ng/mL (range 0.3–20 ng/mL), (ii) Human Adiponectin (R&D Systems, Minneapolis, MN, USA) with assay sensitivity of 0.891 ng/mL (range 3.9-250 ng/mL), (iii) Human Ghrelin (EMD Millipore Corporation, Billerica, MA, USA) with assay sensitivity 0.03 ng/mL (range 0.05–5 ng/mL), and (iv) Human IGF-1 (R&D Systems, Minneapolis, MN, USA) with assay sensitivity 0.0138 ng/mL (range 0.125–8 ng/mL). Each sample was assayed in duplicate, and the measurements were carried out as per the manufacturer’s protocol using a SpectraMax i3 multi-mode microplate reader (Molecular Devices, San Jose, CA, USA). None of the result of the analyzed energy metabolism hormones was below the lower limit of detection.
Statistical analysis
We compared the infants’ characteristics and urinary levels of energy metabolism hormones in the feeding and weight gain groups using chi-square and analysis of variance (ANOVA) followed by the Tukey test. We also used nonparametric Kruskal-Wallis ANOVA for continuous data as needed. Repeated measurement ANOVA was used to outline the changes in the energy metabolism hormones tested at three points: within 48 hours after birth, at day seven, and day 14 on FEF. We constructed stepwise linear regression models to identify if the proportional quantity of daily maternal milk intake was predictive of the levels of energy metabolism hormones on day 14 in the urine of the studied neonates. The energy metabolism hormones measured after birth were included in each model, in addition to the variables that showed a difference between the feeding groups at a level of P < 0.15. Additionally, we constructed a stepwise linear regression model to identify which energy metabolism hormones and other relevant factors were associated with the median weight gain of the studied very preterm infants in the 14 days of FEF. Data are presented as percentages (%), means, medians with the interquartile ranges (25th and 75th percentiles), regression coefficient (β), or odds ratio (OR) with 95% Confidence Interval (95% CI). We used STATISTICA 13.2 for the data analysis. All statistical tests were two-sided, with a significance level set at a P-value of less than 0.05. The study was approved by the Institutional Review Board (IRB), which required parental consent (IRB Protocol Number 0220120055).
Results
The study included 70 infants. Group 1 (n = 27) had infants fed predominantly with breast milk, including 16 on exclusive feeding with maternal milk. The mean proportion of maternal milk in the Group 1 infants was 98.0% (95% CI 96.6% –99.4%). Group 2 was comprised of 16 neonates on partial feeding with breast milk where the mean proportion of maternal milk was 62.7% (95% CI 55.4%, 70.0%). Group 3 included 27 neonates on predominantly preterm formula, including ten neonates fed exclusively preterm formula, and the average proportion of maternal milk was 6.6% (95% CI 3.3%, 9.9%). In general, the means of the gestational age and PMA at the achievement of FEF were 28.7 weeks (95% CI 28.1, 30.1) and 31.0 weeks (95% CI 30.8, 31.8), respectively. The majority (94.3%) of the studied infants were fed through an OG or NG tube. As shown in Table 1, the gestational age of the neonates in Group 1 was lower than in Group 2 and 3. The feeding method, feeding volume, caloric intake, PMA at FEF initiation, and the end of 14 days on FEF were comparable (Table 1).
Feeding group based comparison of patients’ characteristics
Feeding group based comparison of patients’ characteristics
*Median, and interquartile range (IQR); GA, gestational age; BW, birth weight; NPO, nil per os; DOL, day of life; TF, trophic feeds; PMA, postmenstrual age; FEF, full enteral feeds; OG, oro gastric; NG, nasogastric; PO, per oral; **Mean (95% CI).
Table 2 shows a comparison of the tested energy metabolism hormones within and between groups. None of the result of the analyzed energy metabolism hormones was lower than the sensitivity limit for detection. The within-group comparison revealed a significant increase in the urinary levels of leptin, adiponectin, ghrelin, and IGF-1 from the baseline to day seven and day 14 on FEF. Comparison of feeding groups showed a higher level of leptin in infants in Group1 than those in Group 3 but no difference in the other tested hormones (Table 2). Table 3 presents the significant findings from the stepwise linear regression models that were constructed to identify the factors associated with the levels of leptin, adiponectin, ghrelin, and IGF-1 on day 14 of FEF. In addition to each of the hormones, their baseline levels, gestational age, gender, PMA at FEF achievement, PMA at 14 days of FEF, average feeding volume, and proportion of maternal milk intake in their diet were included. Baseline levels were the main predictors of each tested energy metabolism hormones at the end of day 14 on FEF (Table 3). Furthermore, the mean feeding volume intake during the 14 days on FEF was associated with decreased leptin and adiponectin, and increased ghrelin and IGF-1 in the urine of the studied infants. The proportional intake of maternal milk was directly associated with the concentration of leptin, and indirectly with the level of IGF-1 (Table 3).
Comparison of energy metabolism hormones, within and between feeding groups
Comparison of energy metabolism hormones, within and between feeding groups
IGF-1, insulin-like growth factor 1.
Variables contributing to change in energy metabolism hormone levels on day 14 in fully enteral fed very preterm neonates (β with 95% CI)
‡EMH, energy metabolism hormones; IGF-1, insulin-like growth factor 1; *P < 0.05; **P < 0.01; ***P < 0.001.
Among the 70 studied infants, 30 (42.9%) had a median weight gain of less than 14.8 g/kg/d, ranging from 4.8 g/kg/d to 14.7 g/kg/d. In 40 (57.1%) infants, the median daily weight gain was 14.8 g/kg/d or more, and ranged from 14.8 g/kg/d to 29.5 g/kg/d. Comparison of the infants based on growth velocity less than 14.8 g/kg/d to those with 14.8 g/kg/d or more, showed no difference in gestational age, birth weight, gender, and feeding characteristics (Table 4). There was no difference in the neonatal morbidities and type of intervention except for increased use of mechanical ventilation in neonates with a growth velocity lower than the FIGR (Table 4). Comparison of energy metabolism hormones revealed higher leptin levels in infants with adequate median growth velocity (Fig. 1). We constructed a stepwise linear regression model where median weight gain within 14 days was entered as the continuous dependent variable. In addition to the mean level of leptin, mechanical ventilation coded (1) if yes and (0) if no was entered in the model to identify the independent association of leptin with growth velocity, which was entered as a continuous variable. Although the other characteristics were comparable (Table 4), factors that could be associated with the growth of the preterm infants (gestational age, gender, duration of NPO, the proportion of maternal milk intake, and volume and caloric intake in the diet, PMA at the end of FEF) were also entered in the model. The risk for inadequate weight gain as compared to FIGR was reduced in association with increased levels of leptin (OR = 0.57, 95% CI 036, 0.89, P < 0.02) and increased in the mechanically ventilated neonates (OR 1.91 95% CI 1.1, 3.33, P < 0.03).
Comparison of weight gain groups comparison by patients’ characteristics
Comparison of weight gain groups comparison by patients’ characteristics
*Median, and interquartile range (IQR); GA, gestational age; BW, birth weight; NPO, nil per os; DOL, day of life; TF, trophic feeds; PMA, postmenstrual age; FEF, full enteral feeds; **Mean (95% CI).
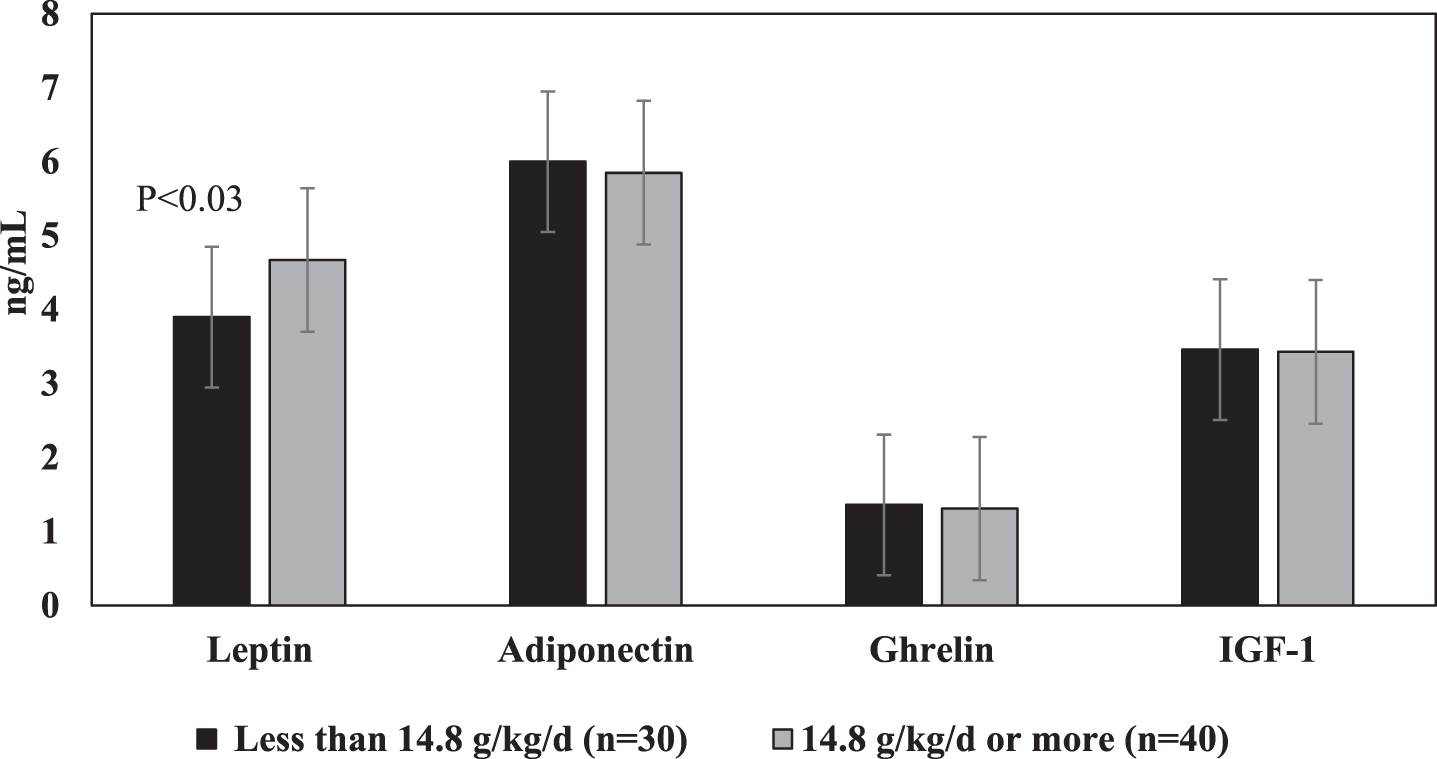
Levels of energy metabolism hormones and growth velocity. IGF-1, insulin-like growth factor 1.
This study is the first that analyzed the levels of human milk contained proteins with metabolism and energy conversion properties, which were measured in the urine of very preterm neonates from the stage before initiation of enteral feeding to up to 2 weeks on FEF. The primary purpose was to identify the postnatal changes in leptin, adiponectin, ghrelin, and IGF-1 and the role of maternal milk intake in the modification of levels of energy metabolism hormones and their function in the growth of very preterm neonates. In our study, the baseline levels of the tested hormones predicted the significantly increased leptin, adiponectin, ghrelin, and IGF-1. The intake of maternal milk is associated with increased leptin and decreased IGF-1. Moreover, the levels of ghrelin and IGF-1 were directly, and leptin and adiponectin were indirectly related to the average feeding volume in the studied fully enteral fed neonates. Very preterm neonates with a growth velocity comparable with the FIGR [21] had a higher urinary level of leptin than infants with lower FIGR growth. In addition, the study revealed a significant risk for inadequate growth velocity in very preterm neonates who underwent mechanical ventilation during the NICU admission.
To our knowledge, the discussion of the study findings is limited to a few investigations in this regard in prematurely born infants. In accord with our results, the analysis of leptin levels in the blood of very preterm infants showed an increased leptin level from birth to up to 36 weeks of PMA [29]. A study did report increased IGF-1 in the blood and a positive association of the increase with the infants’ growth but no change of leptin and ghrelin levels in the first eight weeks of life in very low birth weight infants [17]. However, it has been shown that although IGF-1 is particularly essential for the regulation of intrauterine, it is not for postpartum growth [30], and nutrition does not control the IGF-1 levels in preterm infants [31].
There is inconsistency in the reported data regarding the alteration of IGF-1 levels in infants within the first year of life in breastfed and formula-fed term infants showing increased [32] or decreased [16] blood levels of IGF-1 in breastfed infants. Serrao et al., [33] reported a lack of relationship between the concentrations of IGF-1 in breast milk and IGF-1 in the blood of preterm infants, possibly due to the limitation of intestinal absorption of milk-borne IGF-1. Moreover, supplementation of preterm formula with IGF-I did not affect the anthropomorphic parameters of the neonates [34]. In our study, the leptin levels in the urine of very preterm infants were directly associated with the intake of maternal milk, maybe because the infant formula does not contain leptin [35]. The correlation of the leptin levels in maternal milk with those in the infant blood [36] and the previously reported increased leptin levels being associated with the infants’ weight gain [14, 18] support our study results. However, studies performed during infancy reported either higher [13, 37] or lower [14, 16] levels of leptin in the blood of breastfed compared to formula-fed infants, as well as no association of leptin with the infants’ weight gain [16]. One report showed a direct association of adequate weight gain in breastfed term infants at age 2–3 months with breast milk levels of IGF-1, leptin, ghrelin, and adiponectin [19]. In addition to the association of adequate growth with increased leptin levels, mechanically ventilated neonates more likely had recorded inadequate FIGR growth velocity, which corresponded with previously presented data [38]. In our study, the level of ghrelin decreased in the urine of very preterm neonates who received an increased proportion of maternal milk but increased in association with the feeding volume, possibly because ghrelin is present in infant formulas [39].
We want to acknowledge the limitations of the study. First, two weeks of follow-up after the achievement of FEF assigned at the study design stage could be inadequate for assessing the alteration of the energy metabolism hormones and the infants’ growth. Analysis of the NICU hospitalization showed that follow-up extension for at least one week more would have been possible for 65.3% of the enrolled neonates. Second, FIGR [21] was suitable for assessing the growth velocity because the studied infants were less than 37 weeks of PMA at the end of the 2 weeks on FEF. However, like all others, this method too has not been standardized for evaluating the growth velocity of preterm infants [40]. Third, we did not measure the levels of the energy metabolism hormones in the maternal milk, even though there is a reported risk of lactation stage variability of some of the hormones in preterm maternal milk [3].
Conclusion
Postnatal increase in the leptin, adiponectin, ghrelin and IGF-1 levels in the urine of the fully enteral fed very preterm neonates depends on their concentration at or soon after birth. An increased intake of maternal milk contributes to the level of leptin, which is the only one among the tested energy metabolism hormones that significantly reduced the preterm infants’ risk for impairment of growth velocity during the birth hospitalization.
Conflicts of interest
The authors declare that they have no conflicts of interest.
Funding
None.
Human research statement
The research was conducted in accordance with the ethical standards of all applicable national and institutional committees and the World Medical Association’s Helsinki Declaration.