
Abstract
BACKGROUND:
The utility of determining maternal-neonatal surface colonization as detected by standard microbiological cultures around the time of birth is unclear. The aim of this study is to evaluate the association between maternal and neonatal surface colonization at birth and neonatal early onset sepsis (EOS).
OBJECTIVE:
To investigate the association of white matter hyperintensities (WMHs) present in the brain with AD CSF biomarker levels.
METHODS:
We conducted a case-control study of newborns admitted to the neonatal department of a referral women’s and children’s hospital from 2009 to 2017. Cases were infants with blood-culture-confirmed EOS (<3 days of life), and controls were infants without EOS randomly chosen based on the cases’ date of birth. Maternal genitourinary and neonatal ear swab cultures were used to determine bacterial surface colonization status.
RESULTS:
Fifty-one infants were diagnosed with EOS during the study period, where Escherichia coli (45%), and Group B Streptococcus (23%) accounted for 68% of infecting organisms. Compared to infants without EOS, those infected were more likely to have surface colonization of the mothers (60% vs 40%, p = 0.048) and infants (90% vs 11%, p < 0.001). In univariate analysis, chorioamnionitis [7.1 (95% CI 2.9, 16.8)], small-for-gestational-age [OR 0.08 (95% CI 0.02, 0.4)], exposure to antibiotics around time of birth [2.3 (95% CI 1.0, 5.1)], maternal surface colonization [2.2 (95% CI 1.0, 4.9)] and neonatal surface colonization [23.5 (95% CI 7.3, 76.1)] were significantly associated with EOS. Adjusting for potential confounders, neonatal colonization remained significantly associated with neonatal EOS [AOR 15.0 (95% CI 3.5, 64.2), p < 0.001].
CONCLUSION:
In our setting with predominant Gram-negative EOS, neonatal colonization but not maternal colonization was significantly associated with EOS in the newborn.
Abbreviations
adjusted odds ratio early onset sepsis prolonged rupture of membranes small-for-gestational age
Introduction
Sepsis is the third most common cause of death among neonates globally, accounting for approximately a quarter of neonatal deaths annually [1, 2]. Approximately half of all deaths related to infections and sepsis occur within the first week of life [3]. Early-onset sepsis (EOS), occurring within 3 days of life, is associated with higher rates of mortality and morbidities compared to late-onset sepsis [4]. Microbial colonization of the maternal-infant surfaces are believed to be important in the development of EOS in newborns [5]. Transmission and subsequent colonization of the neonatal skin and surfaces with bacteria is thought to precede invasive infection in the newborn.
Several described antenatal factors are thought to modulate the risk of bacterial colonization of the maternal and neonatal surfaces including: exposure to placental chorioamnionitis, maternal antibiotics and prolonged rupture of membranes (PROM) [6]. The utility of perinatal surface bacterial swabs by standard bacterial cultures around the time of birth, as an indicator of microbial abundance, and its relation to the risk of EOS in the newborn infant is unclear. Limited studies, focused on examining the association between maternal-neonatal surface cultures and EOS, have described positive association between maternal genital and neonatal surface colonization and neonatal EOS [6–8]. We performed a case-control study to investigate the association between perinatal maternal-neonatal surface colonization and neonatal EOS
Methods
Study design and site
We set up a case-control study of all neonates with EOS who were born and admitted to the Department of Neonatology, KK Women’s and Children’s Hospital (KKH), Singapore over a 9-year period (2009–2017). KKH is an 830-bed tertiary-level referral hospital with 40 neonatal intensive care unit (NICU) and 50 special care nursery beds. The hospital is the only specialist women’s and children’s public hospital in Singapore, providing care for around 11,500 pregnant women and 1200 preterm infants annually. An estimated 180–200 infants <32 weeks’ gestation (of which about 90 are ≤28 weeks) are admitted to KKH NICU annually.
Definition and selection of cases and controls
Cases were defined as neonates with EOS (defined by a positive blood-culture using standard bacterial culture techniques within 72 hours of life). A single control was selected for each EOS neonate case. Controls were neonates with no evidence of EOS and were chosen from a sequential list generated based on the date of birth (birth within 3 days of cases), from the KKH Neonatal Database. This database prospectively records clinical information for infants admitted to the Neonatal Intensive Care Unit at KKH. Infants with major congenital anomalies, stillbirths, and labor-room deaths were excluded. Patients without maternal or neonatal swabs were also excluded from the analysis.
Data collection
Perinatal, neonatal, and maternal information were obtained from the KKH Neonatal database [9]. Clinical information extracted included basic demographics, pregnancy course, birth parameters and perinatal microbiological sample results of both mother and baby. Gestational age was defined based on obstetric history and prenatal ultrasound. An infant was considered small-for-gestational age (SGA) if the birth weight was <10th percentile according to Fenton growth charts [10]. Histologic chorioamnionitis was defined as the presence of inflammatory cells in the chorioamniotic membrane, umbilical cord, and/or the placental disc [11]. PROM was considered positive when the duration of maternal rupture of membranes >18 hours. Exposure to antenatal maternal antibiotic was a situation where the mother received antibiotics within 4 hours of birth.
Maternal bacterial colonization was defined as the presence of bacteria from any cultures performed from placental swabs or genital swabs (apart from routine screening) or urine cultures 7 days prior to delivery. The decision to obtain maternal swabs was at the discretion of the obstetrician based on concerns for possible maternal infection and/or PROM. Neonatal bacterial colonization was determined from bacterial culture of universal single ear screening swab routinely performed on admission of all neonates in the unit. Concordance of bacterial swabs was defined as the presence of the same bacteria, with the same antimicrobial resistance patterns of surface swab cultures with EOS isolate. For analysis of maternal and infant surface colonization among the cases, only concordant swabs were included in the analysis, in order to determine the contribution of maternal and infant colonization with the same EOS organism.
Laboratory methods
All blood samples were inoculated into a paediatric blood culture blood using standard aseptic techniques and incubated. All swab samples taken were inoculated on MacConkey agar and 5% sheep blood agar as appropriate and incubated. Identification of organisms present and the antimicrobial susceptibility of organisms were determined using the VITEK-MS system (bioMérieux Inc., Marcy l’Etoile,France). Single blood cultures with coagulase-negative staphylococci, corynebacteria spp, bacillus spp, or multiple organisms isolated from a single blood culture were considered contaminants and not included.
Analysis plan
Continuous data were presented as median (range), and categorical variables were presented as proportions (%). We compared the variables of interest using χ2 test and Mann-Whitney U test, as appropriate. Multivariable logistic regression analysis was performed with the following predetermined clinically relevant variables: vaginal delivery, presence of histologic chorioamnionitis, PROM, SGA status, antenatal steroids, maternal antibiotics and surface colonization status. Odds ratios (ORs) and adjusted odds ratios (AORs) were expressed with 95% CIs. A level of significance of α< 0.05 using a 2-tailed comparison was used in this study. Statistical analyses were performed using IBM SPSS Statistics version 23.0 (IBM Corporation, Armonk, New York).
This study was conducted in accordance with the ethical standards of all applicable national and institutional committees and the World Medical Association’s Helsinki Declaration. Ethics approval for this study was obtained from the SingHealth Centralized Institutional Review Board (CIRB No. 2016/2326).
Results
Cases and controls
The overall rate of EOS in our setting over the study period was 0.5 infections per 1000 live births, with annual rates ranging 0.2–0.8 per 1000. A total of 51 cases of blood culture-confirmed EOS over the 9-year period (2009–2017) were identified and included in the study (Fig. 1). A further 51 controls were included in the study. Clinical characteristics of EOS cases and their associated controls are described in Table 1. In the univariate analysis, cases and controls were not statistically significantly different in terms of sex, gestational age, provision of antenatal steroids, maternal age, PROM and having 5-min Apgar score ≤6. However, a higher proportion of cases (infants with EOS) were exposed to histologic chorioamnionitis (71% vs 26%, p < 0.001), and maternal antibiotics (51% vs 31%, p = 0.04). In contrast, SGA status was more common in the control group (33% vs 4%, p < 0.001).
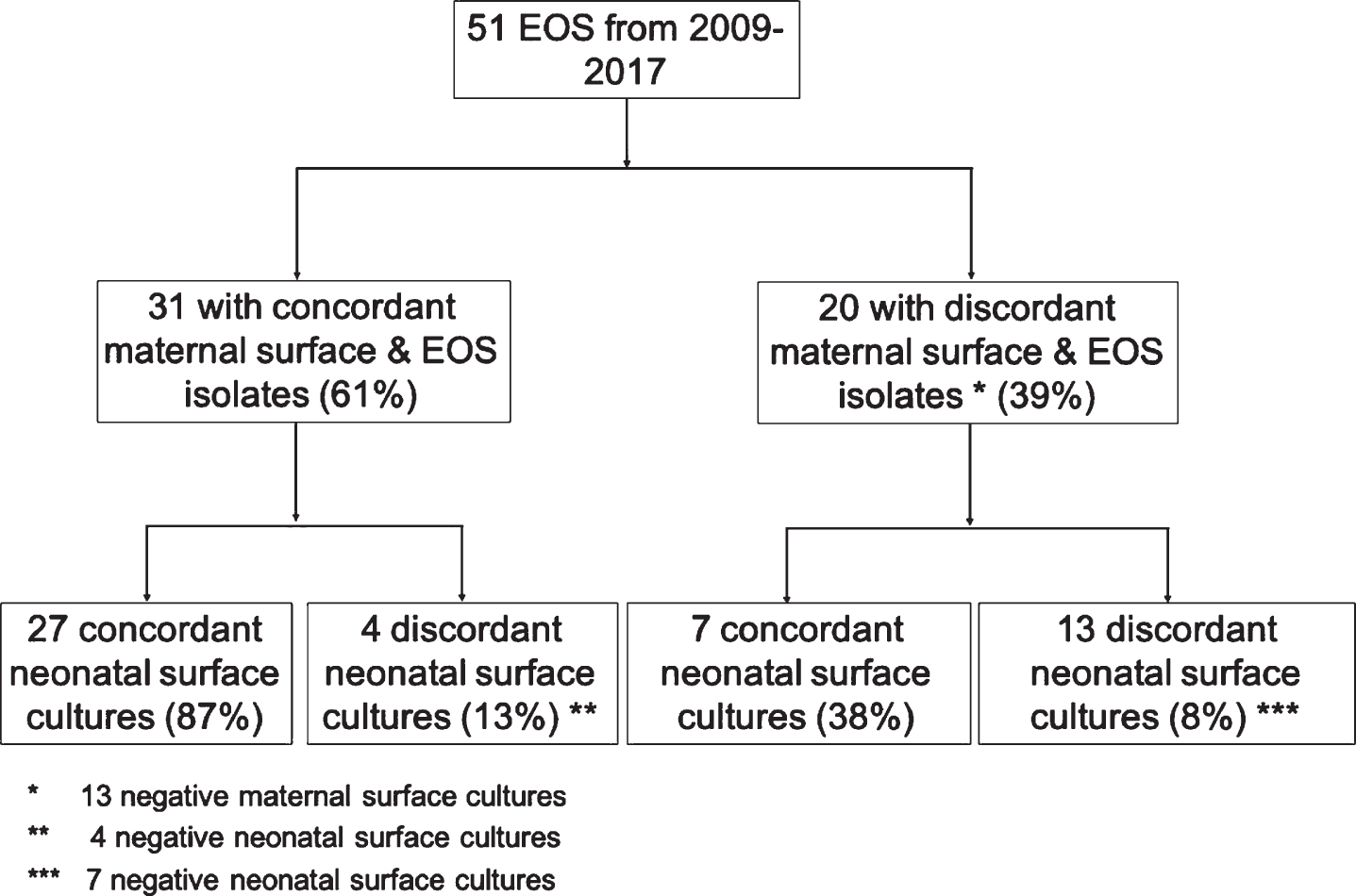
Distribution of surface cultures from mother-infant pairs of cases with early-onset sepsis (EOS).
Characteristics of infants with EOS and those without
EOS, early onset sepsis; GA, gestational age; PROM, prolonged rupture of membranes; SGA, small for gestational age.
Compared to those without EOS, infected infants were significantly more likely to have bacterial surface colonization in the infants and mothers. A total of 60% of mothers of infants with EOS had genitourinary colonization with similar EOS bacteria isolated compared to 40% mothers of controls [OR 2.2 (95% confidence interval (CI) 1.0, 4.9), p = 0.048). Cases also had significantly higher colonization in the ear swab compared to those without (controls) [90% vs 11%, OR 23.5 (95% CI 7.3, 76.1), p < 0.001]. Maternal surface colonization status was significantly associated with histologic chorioamnionitis [69% vs 34%, OR 4.4 (95% CI 1.9, 10.1), p < 0.001)], and maternal antenatal antibiotics [67% vs 40%, OR 3.0 (95% CI 1.3, 6.8), p = 0.008] but not vaginal delivery or PROM. Similarly, infant surface colonization at birth was associated with histologic chorioamnionitis [67% vs 9%. OR 19.8 (95% CI 6.6, 59.3) p < 0.001], exposure to maternal antibiotics [55% vs 25%, OR 3.6 (95% CI 1.6,8.4), p = 0.002], PROM [55% vs 27%, OR 3.4 (95% CI 1.5, 8.0), p = 0.004] and lower gestational age [29 weeks vs 30 weeks. P = 0.046].
Isolated bacterial species
Majority of bacteria species isolated in EOS cases were Gram negatives [n = 36 (71%)]. E. coli (n = 23) and Group B streptococcus (GBS) (n = 12) accounted for 68% of infecting organisms in our population (Table 2). There were three isolates of Pseudomonas aeruginosa, K. pneumonia and L. monocytogenes each, accounting for 18% of all bacteria isolated. Gram negative bacteria also accounted for a higher proportion of the overall infections among infants <32 weeks gestation –25/31 (81%). The distribution of bacterial species and subtypes in maternal genitourinary or neonatal ear swab isolates were similar to EOS case isolates.
Distribution of EOS organisms and surface colonization
Distribution of EOS organisms and surface colonization
EOS, early-onset sepsis.
In univariate analysis, chorioamnionitis [7.1 (95% CI 2.9,16.8)], SGA [OR 0.08 (95% CI 0.02,0.4)], maternal antibiotics [2.3 (95% CI 1.0,5.1)], maternal genitourinary colonization [2.2 (95% CI 1.0, 4.9)] and neonatal ear swab colonization [23.5 (95% CI 7.3, 76.1)] were found to be significantly associated with EOS (Table 1). In the multivariable model adjusting for potential confounders, neonatal ear swab colonization was significantly associated with neonatal EOS [AOR 15.0 (3.5, 64.2), p < 0.001] (Table 3). However, we did not find significant association between maternal genitourinary colonization and EOS [2.1 (0.6, 7.1), p = 0.2] (Table 4).
Multivariable logistic regression analysis to evaluate association between neonatal colonization with EOS
Multivariable logistic regression analysis to evaluate association between neonatal colonization with EOS
EOS, early onset sepsis; PROM, prolonged rupture of membranes; SGA, small for gestational age. Logistic regression model with the following variables: vaginal delivery, chorioamnionitis, PROM, SGA, antenatal steroids, maternal antibiotics, neonatal colonization.
Multivariable logistic regression analysis to evaluate association between maternal colonization with EOS
EOS, early onset sepsis; PROM, prolonged rupture of membranes; SGA, small for gestational age. Logistic regression model with the following variables: vaginal delivery, chorioamnionitis, PROM, SGA, antenatal steroids, maternal antibiotics, maternal colonization.
In this study, we evaluated the association between perinatal bacterial colonization in mother and infants, with neonatal EOS. After adjustment for potential confounders, we determine that neonatal surface colonization, as evidenced by a positive ear swab, was significantly associated with neonatal EOS but not maternal genitourinary colonization. In our cohort of predominantly preterm infants, Gram negative bacteria was isolated in the bloodstream of more than 2/3 of those with EOS. This distribution of bacterial subtypes was also reflected in the patterns of bacteria colonizing the surfaces of mother and infant. Several clinical factors were found to be strongly associated with detection of bacterial surface colonization in mother and infant including preterm births, presence of placental chorioamnionitis and maternal exposure to antibiotics.
Bacterial colonizers in the maternal genital tract are potentially transmitted to the neonate during delivery, specifically when the infant comes into direct contact with the bacterial flora in the genitourinary tract, or with ascending infections [8]. Neonatal surface colonization could lead to culture-positive EOS through the translocation of bacteria into the bloodstream as a result of immature or disrupted skin and mucous barriers [12]. Our finding of the significantly higher odds of EOS in infants with evidence of neonatal colonization, especially in the presence of histologic chorioamnionitis, is consistent with this proposed understanding of EOS pathogenesis. Most studies in this regard have focused on the epidemiology of maternal colonization with GBS and the subsequent neonatal infection [13]. Studies on intrapartum chemoprophylaxis have demonstrated significant reduction in the prevalence of early-onset GBS disease [14]. However, there is limited understanding of the prevalence of maternal colonization with Gram negative organisms, transmission of the bacteria to the neonate and the associated risk for neonatal EOS [12, 15]. This is especially relevant in our setting (and other settings) with a higher prevalence of Gram negative [1].
Based on a recent systematic review by Chan et al, maternal GBS colonization at delivery was associated with 11 times greater odds of GBS EOS in the infant than in situations of mothers without colonization [OR 11.0 (95% CI 3.6, 33.5)] [6]. No data was available for Gram negative infections due to heterogeneity in studies investigated and no evidence-based interventions to reduce such risks. Several earlier studies, mostly in developed countries, have examined the clinical utility of perinatal surface cultures in predicting bacteraemia and the isolated pathogen [16–18]. Most of these studies, which have focused on the utility of routine surface cultures and their association with any sepsis during the course of the admission, have suggested that they are of limited value –with poor sensitivity, specificity and predictive values. However, these studies were evaluating surface cultures done weekly to twice weekly and their association with sepsis throughout the admission. One study from India found significant association between surface colonization of neonates and EOS, in a setting with predominant Gram negative organism colonization and bacteraemia, which is similar to the findings in our study [7].
The utility of surface swabs in the EOS risk assessment of the newborn is currently limited by the turn-around time taken for culture results to be available, which may take up to 2 days for identification of the bacterial organism. Even so, the availability of newer bacteria identification techniques such as real-time polymerase chain reaction and mass cytometry-based systems [19] for use in blood samples and surface swabs, may significantly increase the sensitivity and reduce the time taken for bacteria identification [20, 21]. This would allow for earlier identification of bacterial colonization and this information could be potentially used in risk stratification for EOS. This could open the possibility of modulation of EOS risks via interventions such as administration of antibiotic prophylaxis tailored to the specific pathogens, specifically among newborns with high-risk maternal-neonatal colonization profiles.
We found that maternal-neonatal surface colonization with EOS organisms was significantly associated with exposure to chorioamnionitis, lower gestational age, exposure to antenatal steroids, exposure to maternal antenatal antibiotics and PROM. Previous studies have demonstrated the association between chorioamnionitis and PROM with colonization of infant with pathogenic organisms around the time of birth. Ascending microorganisms from maternal genitourinary tract can colonize mother and infant in-utero or intrapartum. [6]. The increased surface colonization detected in infants of lower gestational age may be related to the differential microorganisms that are present in preterm births compared to term [22]. Of note, antenatal antibiotic exposure during labour and birth was related to increased surface colonization detected in mother and child. The authors speculate that antenatal antibiotics exposure may select for the proliferation of selected microorganisms in the perineum that leads to increased detection of bacteria on the surface of mothers and infant. However, we are unable to study this further without more detailed data on the types and length of antenatal antibiotics exposure.
The limitations of this study are related to the possible inconsistency of swabbing techniques and the sensitivity of bacteria isolation by standard culture methodology. The detection of organism is dependent on factors such as the amount of specimen collected, timing of collection and technique used [13, 23]. While the indications, timing and methods of maternal swabbing in this study are part of standard clinical care, selection bias may occur due to differing obstetrics practices. It is very likely that mothers with chorioamnionitis were more likely to be swabbed than those without. Another potential limitation is the low overall EOS numbers in our study, although the rates of EOS in our study is within that previously reported in the literature –0.3 to 4.0 per 1000 [24–27]. The low numbers precluded further stratification of the analysis by types of organisms –Gram negatives compared to Gram positives. While concordance of the samples in our study was determined based on the similarity of bacterial isolates and antibiotic susceptibilities, verification by molecular methods would have provided additional evidence for concordance. The lack of more detailed information on the types of antenatal antibiotics used, GBS prophylaxis given and the length of exposure would be important as antibiotic exposure would alter the normal colonization patterns of the maternal-neonatal surfaces during the perinatal period. This in turn, may have modified the risk of developing EOS.
Conclusion
In our population with predominant gram-negative early onset infections, neonatal colonization but not maternal colonization, was significantly associated with the development of EOS in the newborn.
Conflict of interest disclosures
The authors have no conflicts of interest relevant to this article to disclose
Funding
No funding was secured for this study.
Data availability
The datasets generated during and/or analysed during the current study are available from the corresponding author on reasonable request.