
Abstract
OBJECTIVE:
Methylxanthines are the most commonly prescribed drug in neonatal setups. However, Clinicians show indecision in choosing the right agent for Apnea of Prematurity in most of the developing countries. Present study aimed to compare rate of mortality and survival with normal neurodevelopment outcome at 18 to 24 months of corrected age, between Caffeine- and Aminophylline-treated infants for apnea of prematurity.
METHODS:
240 infants were randomly allocated to caffeine and aminophylline for apnea of prematurity during February 2012 to January 2015. Long-term neurodevelopmental assessment was done only from children who had attained corrected age of 18 to 24 months during April 2014 to February 2016. Cognitive, language and motor deficits were assessed by Bayley Scale of infant and toddler development (BSID – III). Postnatal characteristics such as hearing and visual impairments during NICU stay were noted and same were followed up.
RESULTS:
Infants allocated to caffeine group showed 83% less risk of getting cognitive impairment (RR 0.16; CI 95% range 0.02 to 1.36), 50% less risk of developing motor deficits (RR 0.50; CI 95% range 0.12 to 1.95) and 24% less risk of developing language problems (RR 0.76; CI 95% range 0.36 to 1.58). However in all the neurodevelopment domains the difference between groups was not statistically significant. Risk of mortality in caffeine group was 9% less over aminophylline group which was statistically non-significant (RR – 0.92; CI 95% range – 0.45 to 1.84; p = 0.81). Physical growth parameters were found to be similar in both the groups. Risk of developing visual abnormality and hearing impairments was also statistically non-significant between the groups.
CONCLUSION:
Caffeine and aminophylline showed similar effects in reducing the rate of mortality and improving the survival without neurodevelopment delays; though the clinical significance of caffeine over aminophylline cannot be undermined.
Introduction
Apnea of prematurity (AOP) is one among the common problem in premature newborns with low birth weight [1]. Multiple, frequent and recurrent apneic episodes may contribute to neurodevelopmental outcomes [2, 3]. For more than 40 years theophylline and caffeine are the methylxanthines used as main stay to treat AOP [4]. This group of drugs are mainly proposed as central stimulants besides it lowers the threshold of central chemoreceptor to carbon dioxide and improve the contractility of respiratory muscles [3, 5]. Methylxanthines are well known non selective antagonists of adenosine receptors [6]. Adenosine is known to preserve ATP levels in brain and protects brain cell during experimentally induced hypoxia and ischemia in different animal models [7]. Preterm infants are more prone to energy expenditure. Administration of methylxanthines further enhance oxygen consumption which can have detrimental effect on the growth and development [8, 9]. J. A. Kuzemko was the first to accentuate aminophylline therapy for AOP [10]. In recent decades caffeine has been highlighted to be a safer and convenient therapy for AOP [11]. International CAP trial also documented the long-term safety and efficacy of caffeine by comparing it with placebo group [12, 13]. Many trials have reported the short term outcomes of caffeine compared with aminophylline [14]. We previously assessed comparative acute adverse events and short term effectiveness before discharge of the study participants which concluded aminophylline is as effective as Caffeine [15]. However, there is dearth of literature about the effectiveness and safety of caffeine versus aminophylline in terms of long-term outcomes in preterm population. Therefore the present study aimed to compare long-term neurodevelopmental outcome of caffeine versus aminophylline prescribed for AOP in preterm neonates with≤34 weeks of gestational age. We hypothesized caffeine is equally effective over aminophylline in long-term neurodevelopmental outcome.
The objective of this study was to determine whether caffeine treated group decreases the mortality rate and improves the survival rate with normal neurodevelopmental outcomes at corrected age (CA) of 18 to 24 months follow up. Study also assessed difference in growth parameters, hearing and visual abnormalities.
Materials and methods
Present study is a part of Indian Council of Medical Research (ICMR) funded project which was conducted to report the short and long-term effects of caffeine and aminophylline. This study was undertaken after obtaining approval from Institutional Ethics Committee (no. IEC 30/2011). Main trial was registered in the Clinical Trials Registry of India (No CTRI/2012/08/002904). The study was conducted in neonatal Intensive Care Unit of Kasturba Hospital, Manipal. Written informed consent was taken from any one parent. The trial period was set from February 2012 to January 2015. Study population included preterm neonates admitted with≤34 completed weeks of gestation experienced 6 or more apneic spells in 24 hours, or newborn with multiple apneic episode requiring bag and mask ventilation for termination of apneic spells. Any preterm newborn with secondary causes of apnea (sepsis, patent ductus arteriosus, depression from medication) and major congenital anomalies were excluded from the study. Any conditions which interferes neurodevelopment impairment including chorioamnionitis, culture positive sepsis, periventricular leukomalacia, hypoglycemic neonates, more than or equal to grade III Intracranial Hemorrhage were excluded for the follow up study.
Participant flow and follow-up
A total of 240 infants were included in the main study after initial screening for inclusion criteria. By computer generated block randomization techniques newborns were randomly assigned to either caffeine or aminophylline intervention group.
Interventions to caffeine group received a loading dose of 20 mg/kg of caffeine citrate (10 mg/kg caffeine base) diluted in 5 % dextrose and given for 30 minutes then to continue on a maintenance dose of 5 mg/kg (2.5 mg caffeine base) 24th hourly iv or oral preparation of Cafirate solution - 20 mg/ml if no adequate response achieved then the dose was optimized up to 7.5 mg/kg. Neonates allocated to Aminophylline group received a loading dose of 5 mg/kg of aminophylline calculated according to the weight and diluted in 5 % dextrose and followed with a maintenance dose of 1.5 mg/kg 8th hourly (Inj. aminophylline 250/10 ml). If no adequate response were seen dose was titrated up to 2 mg/kg.
To assess long-term neurodevelopment outcome, data were collected only from children who had attained CA of 18 to 24 months during April 2014 to February 2016. Perinatal characteristics such as gestational age, birth weight, gender, APGAR scores, cried at birth, rescue surfactant therapy, need for resuscitation, head circumference, mode of delivery and gravida status were collected from medical records. Postnatal characteristics such as hearing and visual impairments during NICU stay were noted and were followed up at 18 to 24 months of CA. Hearing screening was done prior to discharge using both auditory brain stem evoked response (ABR) and Oto-Acoustic emission (OAE). Abnormal screening was reevaluated at every 3 to 6 months follow up. Audiometry was performed to determine the hearing loss or requirement of amplification with hearing aids or cochlear implants. ROP screening was done till 44 weeks of corrected gestation age (CGA) and abnormal screening were followed up and reevaluated at 6, 12, 18 and 24 months of CA. Visual deficits were documented from the outpatient files as refractive errors diagnosed in study children by regular ophthalmology examination during follow up visits and visual acuity of less than 20/200 [12]. Cognitive, language and motor deficits were assessed by Bayley Scale of infant and toddler development (BSID – III). Score of less than 85 on BSID -III was considered to be abnormal outcome [16]. As physical growth assessment weight, height and head circumference were measured at 24 months CA.
Primary outcome was to assess infant survival with one or more of the following neurodevelopmental disabilities: Cognitive delay, Language delay and motor deficits at the age of 18–24 months. Secondary outcome was set to assess risk of mortality before 18–24 months CA, difference in growth parameters [i) weight ii) height iii) head circumference] between groups and assessment of hearing loss and vision abnormalities.
Statistical analysis
Data was entered in Microsoft Excel and analyzed on SPSS for Windows (version 15, Bangalore, South-East Asia). All continuous variables were summarized using mean and standard deviation (SD) for normally distributed data and median and interquartile range (IQR) were reported skewed distribution. To evaluate statistical significance for continuous variables between groups, Independent sample t test was performed. In case of non-normal distribution, Mann Whitney U test was performed. Chi-square or Fisher’s exact tests were applied for binary/categorical outcomes as appropriate. Two-sided 95% confidence intervals (CI) and a p-value of less than 0.05 were considered to be statistically significant.
Results
Over 240 neonates who were randomly allocated for either Caffeine or Aminophylline group during study period, only 79 infants were evaluated for neurodevelopmental outcomes. Remaining 41% infants out of 134 who had attained CA of 18–24 months from April 2014 to February 2016 were lost to follow up depicted in study flow (Fig. 1).
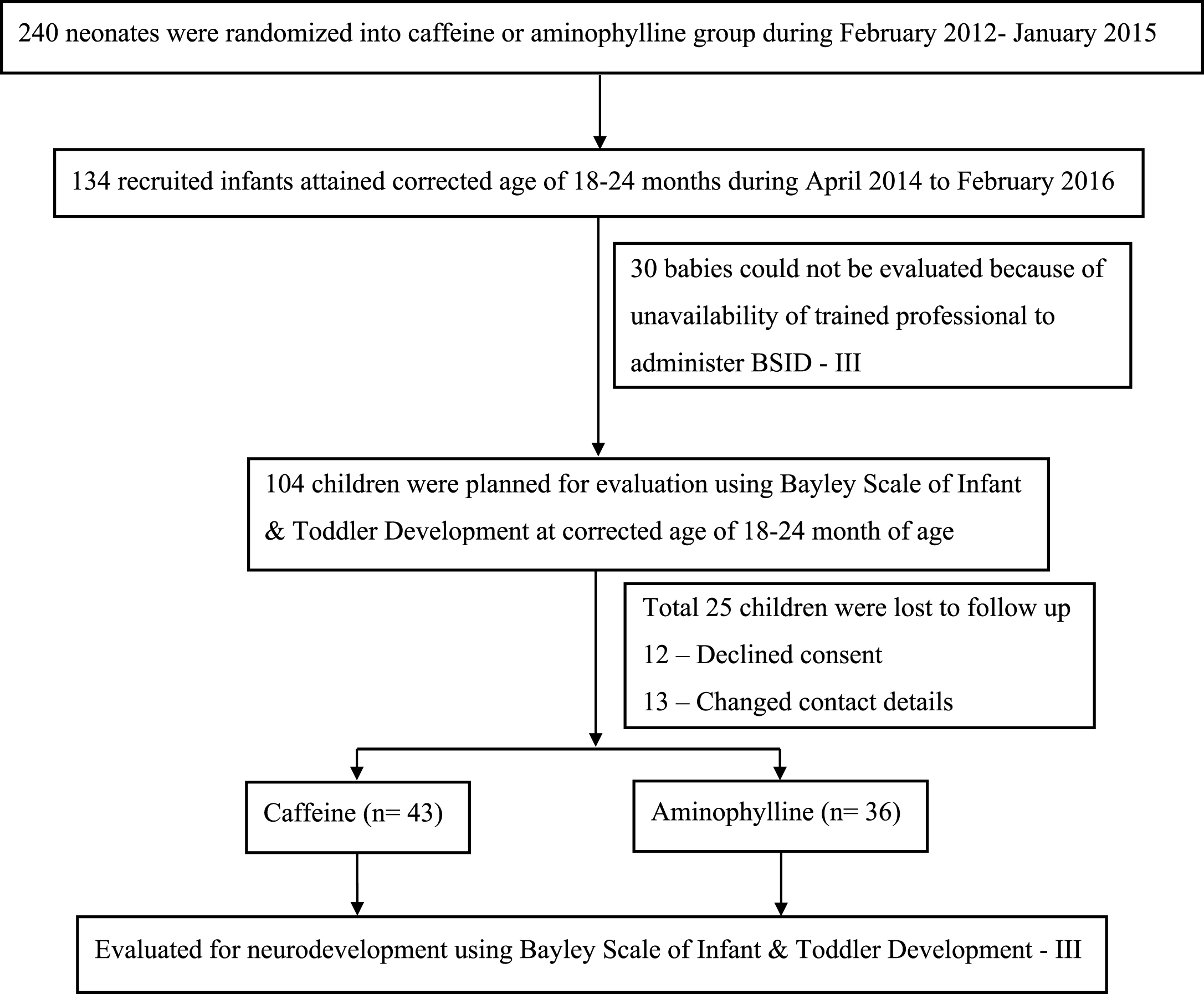
Flow diagram of the follow up.
The baseline characteristics including maternal and neonatal factors for both the groups are reported in Table 1. Maternal factors included parity, type of gestation, mode of delivery and neonatal characteristics included – gestational age, birth weight, head circumference, cried at birth, need for resuscitation, APGAR at 5 minutes, Small for Gestational Age (SGA) and surfactant therapy. Both Caffeine and Aminophylline babies were similar in maternal and neonatal characteristics.
Demographic characteristics
LSCS – Lower Segment Caesarean Section, VD – Vaginal Delivery; adata are presented as n (%); analysis was done by Chi – Square test, bdata are presented as n (%); analysis was done by Fisher’s exact test. #Values are presented as mean±SD; analysis was done by Independent sample t test, $values are presented as median (IQR); analysis was done by Mann Whitney U test.
Incidence of mortality was found to be 11.2% in Caffeine treated infants where against 12.2% in Aminophylline group. Risk of mortality in Caffeine group was only 9% less over Aminophylline group however statistically found similar (RR – 0.92; CI 95% range – 0.45 to 1.84; p = 0.81). Composite scores of three components – cognitive, language and motor were calculated using BSID – III manual. Both the groups showed similar mean scores. There was no statistical significant difference between two groups (Table 2).
Composite scores of BSID III components at 18–24 months of corrected age
Values are presented as mean±SD; analysis was done by Independent sample t test.
Based on scoring attained in congintive, language and motor domain, infants were categorized into adverse neurodevelopmental outcome and normal categories. Only one child who was on Caffeine during NICU stay had abnormal cognitive outcome (2.3% vs 13.9%; RR 0.16; CI 95% range 0.02 to 1.36). Clinically more number of children who had received Caffeine was found to be in normal category in motor and language domain however this difference was statistically non-significant (Table 3).
Adverse neurodevelopmental outcome and normal stratification of infants evaluated using BSID – III at 18–24 months of corrected age
Data are presented as n (%); analysis was done by Fisher’s exact test.
Mean weight, height and head circumference at 24 months of CA was not significantly different between the groups. Total 22 infants had ROP (Stage I- seven, II- four and III -eleven) and 6 had hearing abnormality at discharge. Together 28 infants were assessed for improvement in vision and hearing problems respectively. Out of 11 babies in Caffeine group who had ROP at discharge (5 neonates with stage III), 28% of infants had improved. Out of 11 babies in Aminophylline group (6 neonates with stage III), only 9% infants had improvement. Infants received Caffeine had 40% lesser risk of developing visual abnormalities (RR – 0.60; CI 95% range 0.34 to 1.04; p = 0.11). Out of 5 neonates who were on Caffeine with hearing abnormality, 3 infants showed improvements. Where against 1 baby with Aminophylline who had hearing impairment persisted with the same problem at follow up. However statistically Caffeine group showed 1.5 times higher risk of developing hearing loss over Aminophylline group (RR – 1.50; CI 95% range 0.15 to 14.67; p = 0.61). Results of vision and hearing abnormalities did not show any significant difference between groups (Table 4).
Comparison of physical growth, hearing loss and vision abnormality at two years between the groups
*Values are presented as mean±SD; analysis was done by Independent sample t test, aData are presented as n (%); analysis was done by Fisher’s exact test.
Present study was undertaken as ICMR funded project to document the short and long-term effects of Caffeine versus Aminophylline. In short term effects we evaluated apneic episodes that were found to be similar in both the groups during first 3 days and 2nd week of therapy. However standard doses of aminophylline significantly reduced apneic spells in 4th to 7th day of therapy (p = 0.03). No statistically significant difference was seen in successive events of apnea rate and isolated desaturations in the first and second weeks of methylxanthine administration. Duration of stay in the NICU and hospital ward was similar in both groups. Mean HR was found to be high in aminophylline treated neonates at day 3 of therapy (p = 0.005). Risk of developing tachycardia in caffeine treated neonates was 69.2% less over aminophylline group [15]. As long-term effects we planned to study the survival rate and neurodevelopmental outcomes of recruited infants who attained corrected age of 18 to 24 months during the study period. Average incidence of mortality was reported to be 11.7% with no significant difference between the groups. Mortality rates reported in our study are in consensus with the previous multi-centered placebo controlled trials conducted which also demonstrated no significant differences in mortality rate [12].
Preterm infants are at high risk of neurodevelopmental delays [17]. This can be attributed to their immature central nervous system, physiological instability, underdeveloped organs and inability to maintain their internal homeostasis [18]. Respiratory system is especially not well developed till term age and it could be one of the major factors determining the developmental outcome in preterm infants [19]. Inability to regulate respiration and recurrent apneic episodes can further enhance the chances of neurodevelopmental delays in preterm infants. Studies have reported that last trimester is the crucial period in the brain development of the child. This is the period of corticogenesis and myelination, any discrepancies encountered during this period can lead to serious long-term neurodevelopmental sequelae [20]. It has been reported that apnea is prone to develop in preterm population. Recurrent apneic episodes and severity increases in babies born at lower gestational ages. Methylxanthine remains a mainstay of therapy to treat AOP.
Both methylated xanthines exert common mechanism of actions including calcium release, phosphodiesterase inhibition, GABAA receptor inhibition and antagonism of adenosine receptors [21]. Adenosine is the well-known neuromodulator which has an important role in neonatal respiratory activity [22]. By non-selectively antagonizing adenosine receptors, Methylxanthines provoked a new topic of debate. Methylxanthines are proclaimed as psycho-stimulants but whether to consider as neuroprotective or produce deleterious adverse effects on developing brain is still a controversy [23]. Caffeine triggered neuronal death accompanied by cell body shrinkage in neonatal rat brain [24]. In contrast chronic caffeine intervention in neurodegenerative animal models highlighted a broad spectrum neuroprotection [25]. Theophylline worsened brain injury in hippocampus region in both normoglycemic and hyperglycemic ischemia demonstrated in cerebral ischemic model in rats [26]. In contrast theophylline reduced brain injury in hypoxia-ischemia model in immature 7 day old rats [27].
Initially long-term methylxanthine therapy for asthma was portrayed to have significant adverse effects on cognitive and emotional development in children with 7 to 8 years of age [28]. Since this was reported with lesser evidence, in addition both caffeine and theophylline are closely identical; a meta-analysis was undertaken to present cognitive and behavioral effects on children. This analysis reported that either drug were not associated with unfavorable acute effects on behavior and cognitive function [29].
Methylxanthines are commonly used drug worldwide to treat AOP. The present study reported the differences in language, cognition, motor function as a neurodevelopmental domain. In addition growth, hearing and vision were assessed in study participants during their 18 to 24 months of CA. Although we could not found statistical difference, results revealed higher number of children allocated to Caffeine group was in normal category in all the domains as compared to Aminophylline. Our results are in line with 2007 CAP trial which also reported Caffeine improved the rate of survival without neurodevelopment disability in very low birth weight babies. CAP trial included various sites in western countries and was placebo controlled [12]. Present study compared outcomes of caffeine with aminophylline treated infants because aminophylline is an intravenous form of conventional and prototype drug theophylline. This is easily available and less expensive drug in many developing countries. Majority of the studies highlighted short term safety of caffeine over aminophylline but none of them assessed neither long-term benefits/risks of aminophylline nor long-term effects of caffeine compared over aminophylline [14]. Along with survival rate and neurodevelopment outcome present study compared differences in growth parameters which reported to be similar in both the groups. In addition, we followed up infants with ROP and hearing abnormality at discharge until 18 to 24 months of CA. Follow-up results of vision and hearing abnormalities did not show any significant difference between groups. A recent study [30] reported the prevalence of ROP and brain damage as 6% and 13%. In the present study, the neonates with secondary causes of apnea including brain damage were excluded during initial screening. Among total recruited infants in the main trial, prevalence of ROP was found to be 7.1%. However, we did not correlate co-morbidities with mortality or neurodevelopmental outcomes as reported in Schmidt et al., 2015.
Limitation
Authors revealed there was initial loss of information due to staff deficiency. Investigators were not blinded on patient allocation. All recruited neonates were not followed up for their vision and hearing assessment.
Conclusion
Caffeine versus aminophylline treatment for AOP, the risk of mortality and survival with normal neurodevelopment in terms of cognitive, motor and language were statistically similar. No significant difference in hearing and vision in both groups. Physical growth was also found to be similar in both the groups.
Funding sources
Indian Council of Medical Research (ICMR), New Delhi.
Project number
(IRIS.ID:2010-00970, RFC No.RHN/Ad-hoc/36/2011-12 Date: 12.01.2012).
Conflicts of interest
Authors have no conflicts of interest to disclose.
Footnotes
Acknowledgments
Authors are highly indebted to ICMR for providing essential funding to carry out the project. Authors would also like to express their heartfelt gratitude to the parents who voluntarily gave consent for their infant participation in the study. We hereby declare the above stated funding agency does not have any role in study design, in the collection, analysis and interpretation of data; in the writing of the report; and in the decision to submit the article for publication.