
Abstract
BACKGROUND:
Persistent pulmonary hypertension is a problem that leads to high morbidity and mortality in preterm infants. In clinical studies, oxidative stress (OS) contributes to the development of pulmonary hypertension (PH). The most specific biomarker of OS in preterm infants is urinary 8-hydroxy-2-deoxyguanosine (8-OHdG).
The aim of the study was to determine the clinical correlation between the value of 8-OHdG and the level of a mean pressure in the pulmonary artery (mPAP) in premature infants with respiratory distress syndrome (RDS) and asphyxia in the early neonatal period.
METHODS:
Determination of the urinary 8-OHdG value and PH in 96 premature infants born at gestational age of 26–32 weeks on the 1st and the 3rd–5th days of life in two groups: group I –52 children with respiratory distress syndrome; II –44 children with RDS associated with perinatal asphyxia.
RESULTS:
The 2nd group of children had higher average mPAP level, mmHg, both in the 1st and in the 3rd–5th day of life compared with the 1st group. The value of the urinary 8-OHdG correlated with the manifestation of PH that required prolonged respiratory support in group II.
CONCLUSION:
Perinatal asphyxia in preterm infants with RDS on the 1st day of life complicates the course of PH, as indicated by a higher level of the urinary 8-OHdG and correlated to mPAP. Gender characteristics of the dynamics of 8-OHdG levels in children with perinatal pathology reveal reduced adaptability and reactivity of boys to OS at birth.
Introduction
Persistent pulmonary hypertension (PPH) is a syndrome that complicates the early neonatal period and leads to high morbidity and mortality in preterm infants. The mechanisms of transformation of the cardiovascular, respiratory, and central nervous system in the cohort of preterm infants with PPH are still poorly explored. The studies on the role of the PPH in the remodeling of the cardiorespiratory system focus on searching for the best strategy in managing this pathology, especially in the population of premature infants [1, 2].
PPH develops as a result of persistent vasospasm resulting from hypoxia, acidosis, hypothermia, hypoglycemia, and polycythemia. Reactive oxygen species, like superoxide and hydrogen peroxide (H2O2), induced by hypoxia, lead to vasoconstriction as well [3].
The value of the urinary 8-OhdG is known as one of the most specific markers of nucleotide damage due to OS in premature infants [4–6].
The paper‘s aim is to establish the clinical correlation between the value of 8-OHdG and the level of a mPAP in premature infants with RDS and asphyxia in the early neonatal period.
Methods
Study design and participants
This prospective cohort study included 96 infants born prematurely at gestational age of 26/1–32/6 weeks, all of them were nursed in the intensive care unit for premature newborns in conformity with the modern standards. All parents gave an informed consent statement.
We studied the correlation between mPAP and the value of the urinary 8-hydroxy-2-deoxyguanosine in infants with RDS and RDS associated with perinatal asphyxia.
Infants were divided into two groups; group I consisted of 52 children with RDS without perinatal asphyxia, group II embraced –44 children with RDS associated with perinatal asphyxia. There were 48 (50%) boys and 48 (50%) girls among the babies. The inclusion criteria for both groups were based on manifested PPH, determined with the help of ECHO-KG monitoring according to the European recommendations [7]; gestational age 26/1–32/6 weeks, presence of RDS, presence of RDS associated with perinatal asphyxia.
Exclusion criteria: gestational age < 26/1 or > 32/6 weeks, congenital heart disease, early neonatal sepsis, presence of hemodynamically significant patent ductus arteriosus.
Evidence of birth asphyxia was based on a pH≤7.0 and/or a base deficit≥12 mmol/L in an umbilical cord blood sample during the first hour after birth, 10 min Apgar score≤5 [8].
A quantitative outlining of the value of 8-OHdG, ng/ml on the 1st day of life, and on the 3rd–5th day was provided by ELISA using the DNA Damage ELISA kit, Enzo Life Sciences (USA) as the manufacturer’s instructions require.
Statistical analysis
All computations were made with use of STATISTICA 10 and Microsoft Excel 2019 software. Quantitative data were presented as the median and inter quartile range (IQR; 25th to 75th percentiles).
Using Fisher‘s exact test we analyzed –the quantitative parameters. Significance was assumed at p < 0.05.
Pearson’s linear correlation coefficient (r) was applied to find the correspondence between mean mPAP and the value of the urinary 8-OHdG. Significance was assumed at p < 0.05.
Results
Patient characteristics
The newborns were divided into two groups. All the children of our study were comparable in terms of gestational age and birth weight (Table 1).
General characteristics of patient groups
General characteristics of patient groups
RDS-respiratory distress syndrome.
During the treatment, which included surfactant administration, choosing the most optimal tactics of respiratory therapy (high-frequency ventilation, traditional mechanical ventilation, non-invasive mechanical ventilation, CPAP), correction of metabolic acidosis, hypoglycemia, the following results were obtained.
In group I the average mPAP level, mmHg. of children on the 1st day of life was lower than in group II (24.90±0.41 vs 27.60±0.32, p = 0.037). In the group II regardless of the treatment, the average mPAP, mm Hg. of children increased on the 3rd–5th day of life. Yet in group I the average mPAP reduced during the treatment (29.20±0.67 vs 19.95±0.30, p < 0.001).
Concurrently the levels of urinary 8-OHdG, ng/ml, were examined: on the first day of life in children of group II the indicator was higher than in children of group I (3.08±0.02 vs 2.79±0.02, p < 0.001). By the 3rd–5th day of life, in children of group II, we noted an increase in the level of 8-OHdG while in group I the indicator decreased (3.43±0.01 vs 1.29±0.04, p < 0.001).
The children in group II received longer respiratory support (in days) (7.33±0.61 vs 4.04±0.41, p = 0.0031) (Table 2).
Comparison of the level of oxidative stress and PPH in newborns by groups
Comparison of the level of oxidative stress and PPH in newborns by groups
RDS-respiratory distress syndrome; mPAP-mean pulmonary artery pressure; 8-OhdG-8-hydroxy-2-desoxyhuanosine.
Regarding the gender characteristics, the following distribution of 8-OHdG levels, ng/ml, was obtained: on the 1st day of life in boys, the level of the urinary 8-OHdG was 2.63±0.01, in girls it was 2.54±0.02 (p = 0.003). The level of the urinary 8-OHdG in boys elevated to 7.2% by 3–5 days and amounted to 2.82±0.02; in girls it decreased by 43.3% –1.44±0.05 (p = 0.004).
Correlation analysis of the mPAP, mmHg. and 8-OHdG, ng/ml, in both groups on the first and 3rd–5th days of life showed a number of regular matches. In children with RDS on the first day of life, the correlation coefficient was 0.78, p = 0.001, however, by 3–5 days of life, the correlation coefficient decreased to 0.70, p < 0.001 (Figures 1 and 2).
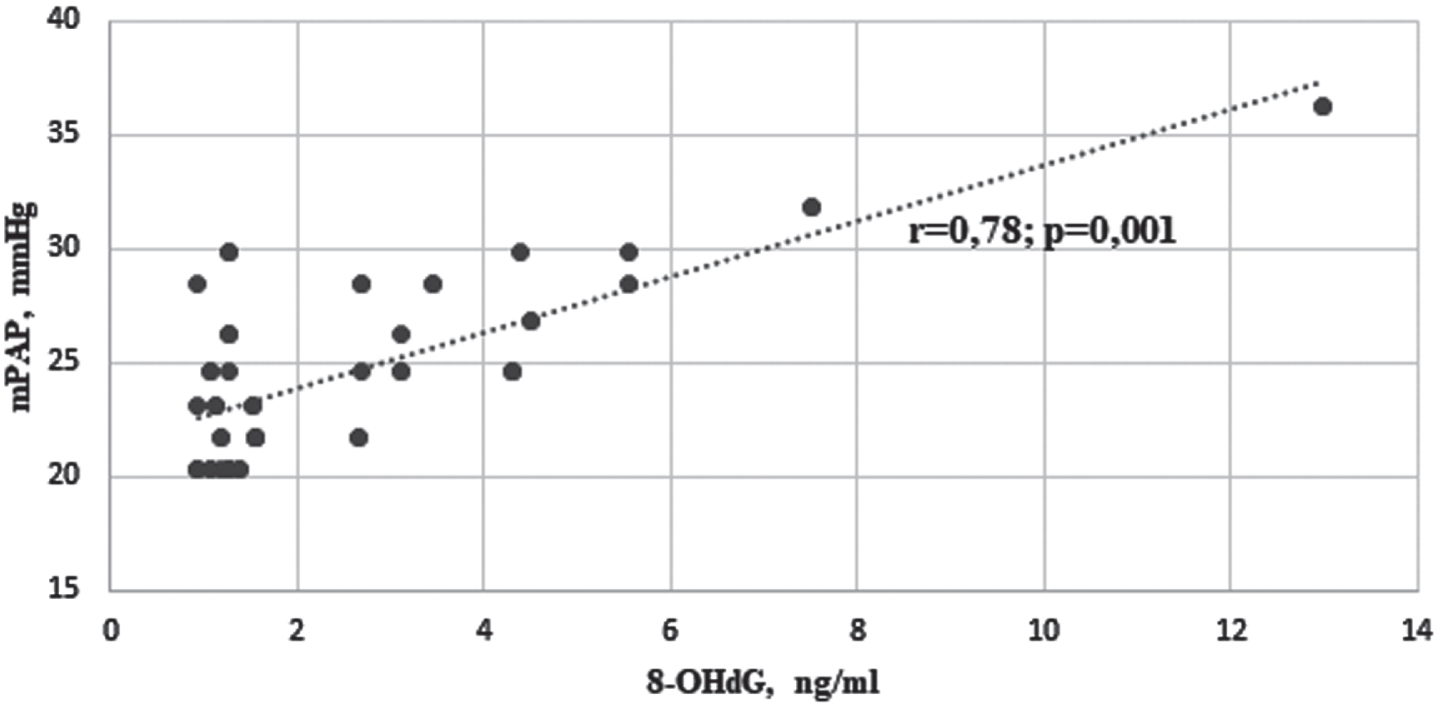
Correlation between mPAP and 8-OHdG levels in children with RDS on the 1st day of life.
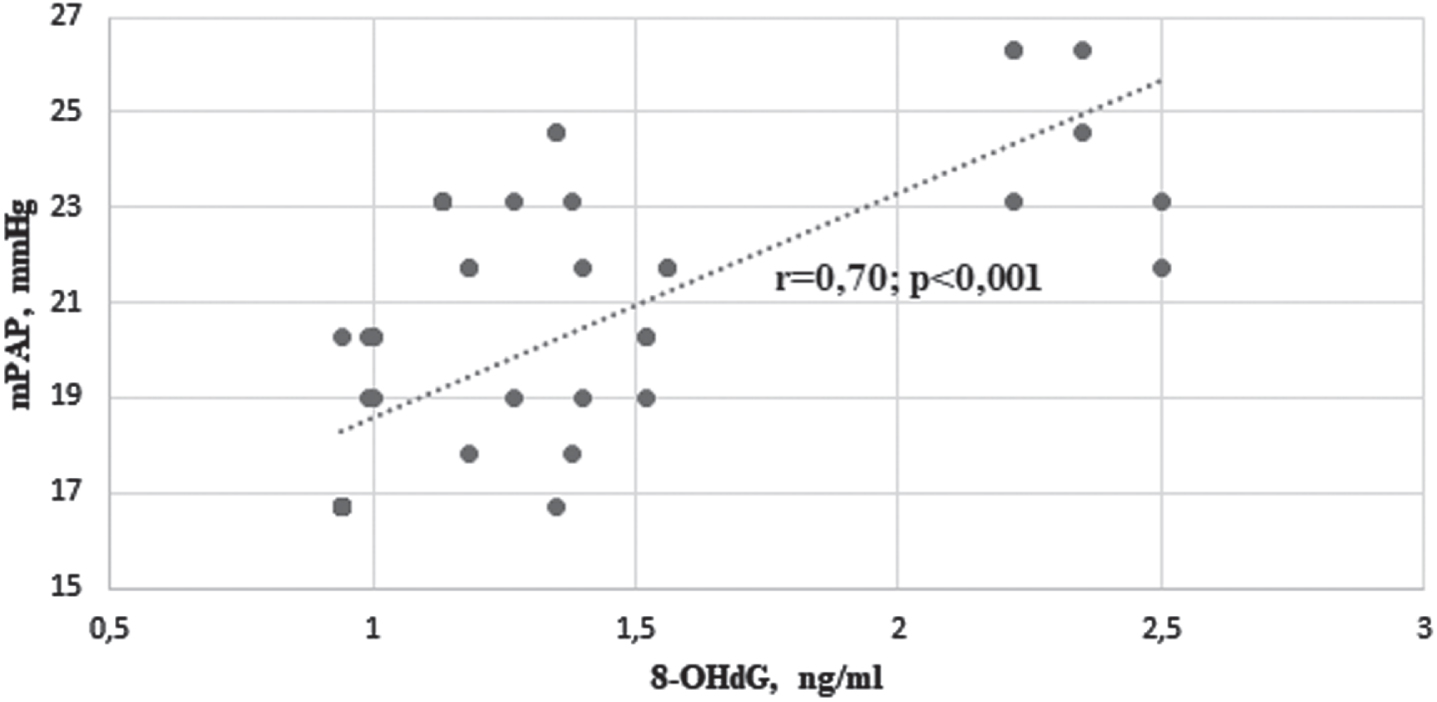
Correlation between mPAP and 8-OHdG levels in children with RDS on the 3rd–5th days of life.
In the group of children with RDS and with associated birth asphyxia on the first day of life, the correlation coefficient was 0.72, p = 0.02; on days 3rd–5th it reached 0.70, p < 0.001 (Figs. 3 and 4).
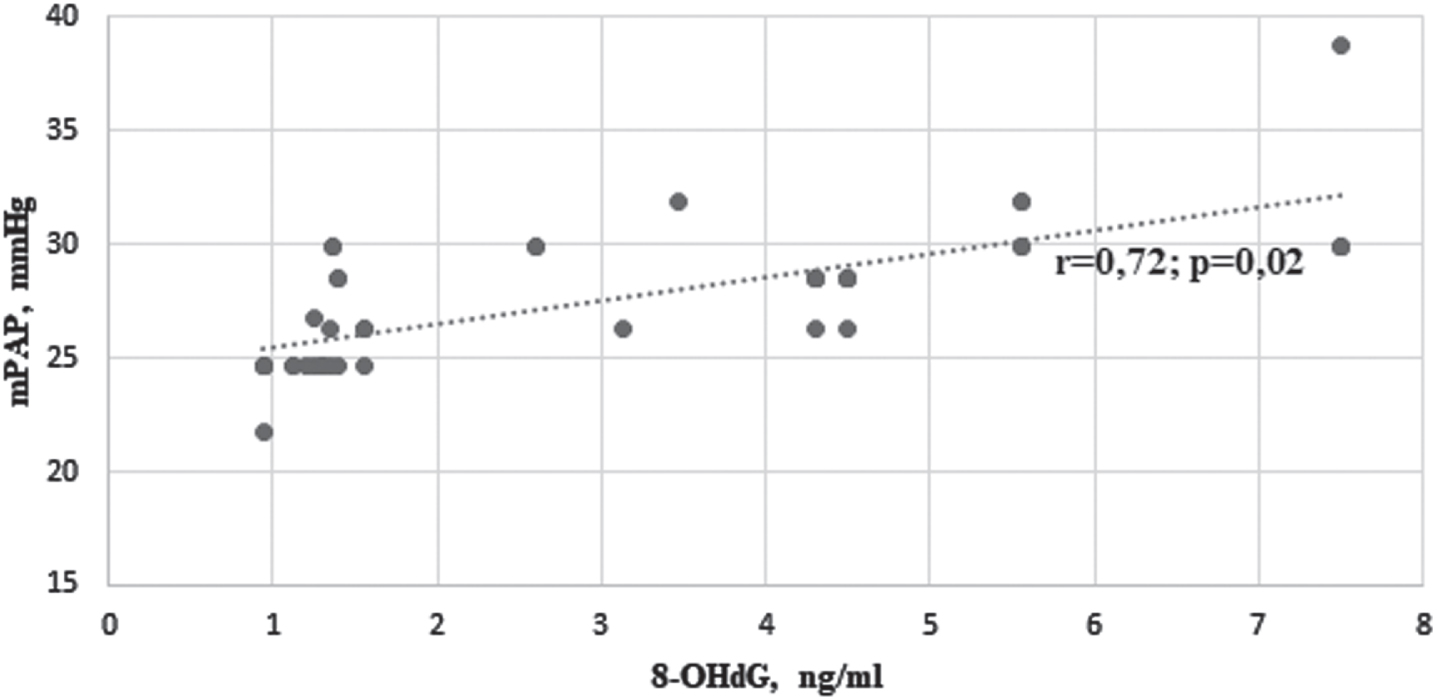
Correlation between mPAP and 8-OHdG level in children with RDS and birth asphyxia on the 1st day of life.
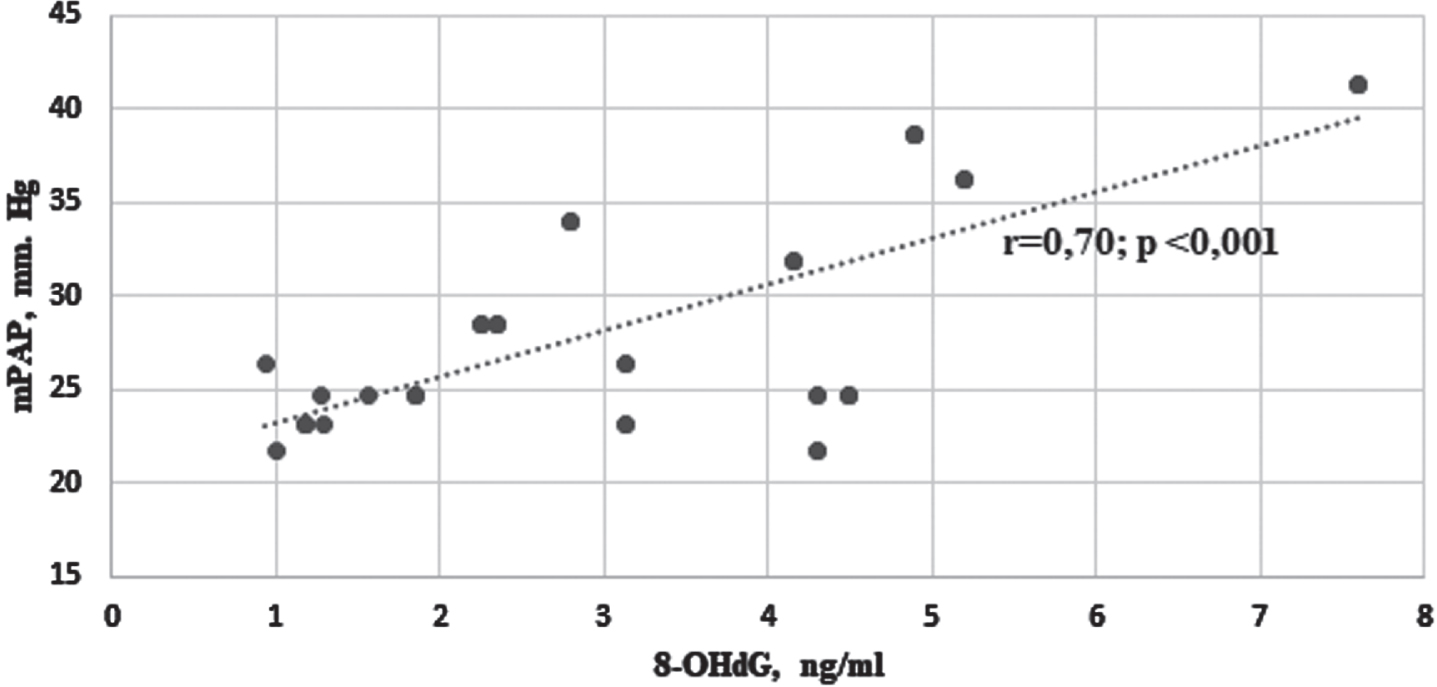
Correlation between mPAP and 8-OHdG level in children with RDS and birth asphyxia on days 3–5 of life.
Modern technologies can significantly improve the quality of caring for low birth weight infants and reduce the number of complications. However, PPH still remains a serious clinical problem for diagnostics and treatment, particularly in the population of premature infants.
A fetus has high pulmonary vascular resistance due to low oxygen partial pressure in arterioles and alveoli. Normally, from the moment of the umbilical cord clamping and beginning of spontaneous breathing, the partial pressure of oxygen in the alveoli increases. Still, birth asphyxia contributes to maladaptation of the cardiorespiratory system, with a further mPAP increase and the progression of PH [9–11, 13].
Another cause of PPH in preterm infants with RDS is abnormal pulmonary vasoconstriction as a result of unexpanded lungs. Therefore, therapeutic strategies usually included pulmonary recruitment and surfactant administration that helps to reduce increased mPAP [14].
In our observations, on the first day of life, the following values of mPAP in the group of children with perinatal asphyxia amounted to (mm Hg): 27.60±0.32; by 3rd–5th days of life, the average mPAP increased to 29.20±0.67 mmHg, by 5.79% against the initial value.
In the group of children with RDS on the first day of life, the average mPAP was 24.90±0.41 mmHg, which a decreased to 19.87% by days 3–5.
Thus, the level of mPAP in children with RDS and its dynamics pivot on the force of asphyxia, as the literature data evince [9–11, 14]. Infants born with asphyxia and < 32 weeks of gestation usually require primary resuscitation with positive pressure ventilation and supplemental oxygen, which releases large amounts of free radicals. In children < 32 weeks of gestation, the production of antioxidants, such as superoxide dismutase, catalase and glutathione –is reduced [5]. Hence, a decrease in the partial pressure of oxygen in blood, causes disruption in production of the nitric oxide synthase enzyme, which is necessary for the synthesis of nitric oxide (NO), known as the endogenous vasodilator. The key factor in reducing the bioavailability of endogenous NO in tissues is the activation of superoxide anions due to oxidative stress caused by asphyxia [10, 14]. In addition, free radicals are the factors damaging the surfactant [14].
According to our data, the level of OS determined by the value of the urinary 8-OHdG (ng/ml) in premature infants in the group with RDS associated with asphyxia on the first day of life was 3.08±0.02. By 3rd–5th days, there was noted an increase in the level of 8-OHdG by 11.3%.
In the group of children with RDS, the value of 8-OHdG on the first day of life was 2.30±0.09 ng/ml, and by days 3–5 it was 1.29±0.04, i.e., decreased by 53%.
Consequently, asphyxia contributes to an increased level of OS in children with perinatal pathology. The studied OS biomarker indicates the severity of the condition and PPH, which requires a longer respiratory support (4.04±0.41 vs 7.33±0.61, p = 0.003). Similar results were obtained by Z. Elkabany, et al., who established a direct moderate positive correlation between the level of the 8-OHdG and the number of days on mechanical ventilation (r = 0.574, p = 0.02) [15].
The substantiated positive moderate correlation between the level of the urinary 8-OHdG and mPAP may give the green light for adopting it and applying in practical management of premature newborns with RDS. The gender characteristics of the levels and dynamics of 8-OHdG indicate a lower adaptability and reactivity of the antioxidant system in male newborns, which have already been verified in several previous studies [12, 17].
Conclusions
Our investigations allows us to summarize the following outcomes: Perinatal asphyxia complicates the course of RDS in newborns due to stronger manifested PPH and a higher level of OS; The value of the urinary 8-OHdG, which indicates the level of OS at birth, correlates with the mPAP in newborns with RDS and RDS associated with birth asphyxia in the early neonatal period; A decrease in the 8-OHdG level is a favorable prognostic sign of the course of RDS and it is associated with a decreasing mPAP; Gender characteristics of the dynamics of 8-OHdG levels in premature infants with RDS and asphyxia with perinatal pathology confirm the reduced adaptability and reactivity of boys to OS in the early neonatal period.
Conflict of interest
Tetiana Klymenko: none.
Mariia Kononovych: none.
Human research statement
Ethics approval was obtained from appropriate local ethics committee and research was conducted in accordance with the World Medical Association‘s Helsinki Declaration.
Disclaimer statement
This research received no external funding.