
Abstract
Infants in the NICU setting often require emergent bedside surgical procedures, during which, they are at high risk for developing hypothermia. Reasons for hypothermia in infants include poor temperature regulation, decreased fat stores to maintain temperature, increased insensible losses. Neonatal hypothermia is associated with an increased risk of sepsis, cardiorespiratory failure (pulmonary hypertension), hypoglycemia and death. In this case series, we describe the novel use of servo-controlled water blanket system as a method to actively maintain normothermia during three surgical cases. Although water blanket systems are frequently used in the neonatal ICU to provide active hypothermia treatment, to our knowledge there have been no prior reports of this system being deployed in normal and low-birthweight infants in the perioperative period.
Introduction
Hypothermia is a significant contributing factor in neonatal morbidity and mortality [1]. Infants are at risk for hypothermia due to increased insensible losses [2], decreased stores of brown adipose tissue [3], and proportionally large body surface area. Poor thermoregulation increases risks of sepsis [4], hypoglycemia [5], increased metabolic stress [6], pulmonary hypertension [7], and death [1, 8].
Infants undergoing surgery are at added risk for hypothermia due to evaporative heat loss from exposed bowel, impaired thermal homeostasis from general anesthesia [9], instillation of irrigation fluids, and ineffective provision of conventional thermal support (i.e., radiant warmers) [9]. Not surprisingly, improved perioperative temperature management is a high-priority target for many institutions.
There is some published evidence that supports the use of forced air thermal management systems improving postoperative temperatures compared to conservative (non-active) treatment [9]. Significant drawbacks of these devices are the lack of servo control, lack of availability outside the operating room, reports of burns associated with use [10], and limited experience in smaller neonates (those with weights less than 2000 grams).
Water blanket systems have been extensively used in Neonatal Intensive Care Units (NICUs) globally since the mid-2000 s to provide active therapeutic hypothermia treatment for infants suffering from hypoxic ischemic encephalopathy. As a result, there is considerable staff experience and familiarity with these systems which can be leveraged in a preventative context to provide active normothermia treatment. In comparison to forced air systems, water blanket systems are readily available in the NICU, have active servo control mechanisms, and utilize core temperature monitoring.
In this report, we describe the novel usage of a water blanket system to maintain temperatures in the perioperative period for infants undergoing bedside surgery in the NICU.
Treatment protocol
A common treatment protocol was used for all the infants described in this report. First, all positioning and monitoring devices (i.e., ECG electrodes) positioned between the water blanket and infant were moved to prevent potential pressure injuries. Next, a provider inserted a rectal temperature probe (General Purpose Temperature Probe, DeRoyal Industries, Powell, TN) to a depth of 2.5–3.5 cm and placed them on the water blanket (Neonatal Arctic Gel Pad, BD, Franklin Lakes, NJ, USA) connected to the water blanket control system (Arctic Sun Stat, BD, Franklin Lakes, NJ, USA) at least 30 minutes before the case started. As the patient goal temperature was defined between 36.5 and 38 °C, the lower control limit was set to 36.5°C and the upper control limit was set to 38°C. As a safety measure, water temperature was limited to a maximum of 40°C was selected, consistent with manufacturer recommendations. After completion of each case, the infant was placed back to their original means of thermal support (e.g., isolette or warming table) and the water blanket system was transitioned to monitoring mode. During this time, the infant’s temperature was passively monitored without providing water blanket thermal support; the system only engaged if the core temperature fell below 36.5°C. If active treatment did not start during monitoring mode, the device was discontinued, and routine care resumed.
For all cases, device output was captured for offline review including core patient temperature and water temperature; all data points were automatically recorded once per minute. For each case, the duration of normothermia treatment, surgical case time, mean core temperature, mean water temperature, and proportion of treatment time within goal temperature range (defined as 36.5–38.0°C) were recorded. Written informed consent was obtained from the parents of all patients for publication of this case report.
Case 1
An 11-day old, former 33-week infant underwent a left sided congenital diaphragmatic hernia (CDH) repair. The infant was delivered due to severe intrauterine growth restriction and had a relatively uncomplicated clinical course prior to surgical repair. As this was the first case using the water blanket system, the patient was placed on the water blanket well in advance of the surgery start to allow time for adjustments. Close monitoring revealed that the initial patient upper control temperature selection of 37.3°C did not provide sufficient thermal support to maintain core temperature above 36.5°C (see Fig. 1) and upper control limit was changed to 38°C for the remainder of the case. After the case, the water blanket was found to be saturated with irrigation fluid, and per manufacture guidelines, the monitoring period was terminated early, after 12 minutes.
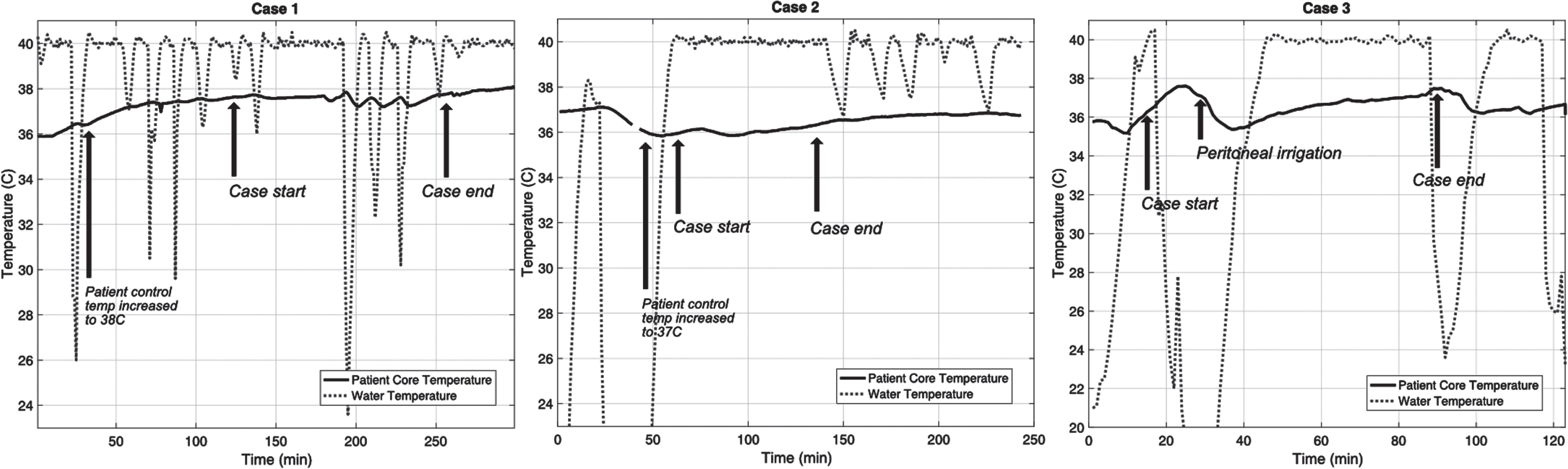
Plots of core body temperature and water temperature for all three cases. In case one (left), the target temperature was increased to 38 C at the first arrow. In case 3, note the significant drop in core temperature after peritoneal irrigation was performed.
The second case was a 6-day old, former 39-week infant also undergoing left-sided CDH repair. The infant’s hospital course prior to the surgery was complicated by marked hemodynamic instability including the need for considerable ventilatory support, inhaled nitric oxide, inotropic medications, and significant sedation needs. As the patient had a greater body weight, a lower patient control temperature was initially selected (36.5°) but was later increased to 37°C due to below target temperatures. All out-of-goal values were below goal and occurred at the beginning of the case.
Case 3
The third case was a 22-day old, former 23-week infant undergoing an exploratory laparotomy for spontaneous intestinal perforation and included resection of large and small bowel. The infant’s pre-operative course was been complicated by respiratory failure, hemodynamically significant patent ductus arteriosus, and intraventricular hemorrhage. As shown in Fig. 1, a significant drop in core body temperature occurred during peritoneal irrigation. As with the second case, all out-of-goal values were below goal and occurred at the beginning of the case.
Comparison with historic controls
130 historic control infants were identified in the three years prior to start of active normothermia; 88/130 (68%) were premature (defined as corrected gestational age at time of surgery less than 36 weeks). Although standard care does not capture temperature data with the same resolution as the active normothermia device, body temperature was intermittently monitored during procedures and one hour after the end of the case. Intraoperatively, the lowest recorded temperature was 35.7°C in the active normothermia group compared to 31.9°C for the historic controls.100% of the infants who used active normothermia had a body temperature > 36.5°C one hour after the end of the surgical case, compared to only 63% of historical controls.
Discussion
In this series of three cases, we have demonstrated that perioperative active normothermia treatment using a water blanket system is both feasible and safe in the low and normal birth weight population. This approach generates intraoperative and postoperative temperature outcomes superior to standard care.
Regardless of infant weight at the time of surgery, there is marked and persistent loss of heat during bedside surgery. In all three cases, during the operation, the water temperature hovered close to the maximum of 40°C, an indirect indicator of significant heat loss. Indeed, during the first case, we identified that our initial patient lower control temperature selection of 37.3°C was insufficient, as the ± 0.5°C tolerance of the water blanket allows the core temperature to drop as low as 36.8°C, perilously close to the bottom of the goal range at 36.5°C. Such a limited margin leaves the patient vulnerable to hypothermia in the setting of an acute thermal stress, such as peritoneal lavage. This concern was further validated in the second case when a lower control point was insufficient to maintain core temperatures within the goal range.
Descriptive statistics
Active normothermia treatment has significant potential to provide better perioperative temperature control in all neonates undergoing bedside surgery. Quality improvement efforts will be needed to optimize the approach and achieve maximal benefit. As hypothermia may influence a wide range of organ function, other parameters (including acid-base status, blood glucose, and changes in ventilatory needs) should be compared in a larger sample against similar historical controls.
Disclosure statements
The authors have no conflicts of interest to declare. This study received no funding.