
Abstract
INTRODUCTION:
Although breast milk is considered the optimal nutrition for infants, it is also the primary cause of postnatal cytomegalovirus (CMV) infection. Preterm infants with postnatal CMV infections are susceptible to a variety of life-threatening conditions.
CASE SUMMARY:
Twin male infants were delivered via emergency caesarian section at 27 weeks’ gestation secondary to maternal complete uterine rupture. The Apgar scores at 1 and 5 min were 1 and 1 for the older twin (Twin A) and 0 and 3 for the younger twin (Twin B). Their birth weights were 1203 g (+ 0.65SD) and 495 g (– 3.79SD) respectively. On day 41, laboratory blood test results for Twin B showed a moderate elevation in C-reactive protein (CRP), thrombocytopenia. CMV quantitative polymerase chain reaction (qPCR) tests in Twin B’s urine and blood as well as in the mother’s breast milk were positive, but stored, dried umbilical cord CMV qPCR tests were negative. Twin B was diagnosed with a postnatal CMV infection secondary to infected breast milk and ganciclovir was commenced on day 52. Treatment was switched to valganciclovir at 74 days of age, but a negative CMV-DNA level in the blood was not achieved. Postnatal CMV infection in this infant led to an exacerbation of pre-existing bronchopulmonary dysplasia (BPD) and he demised at 182 days of age.
CONCLUSION:
Postnatal cytomegalovirus infections may lead to exacerbations of BPD. Early use of raw breast milk in preterm infants should be done with careful consideration of this potential complication.
Introduction
Cytomegalovirus (CMV) infection is one of the most common and well-recognized causes of congenital and perinatal viral infections. Congenital CMV (cCMV) infection occurs in utero and involves multiple organs, including the central nervous system, resulting in neurological sequelae.
Perinatal CMV (pCMV) infections can be caused by exposure to the virus in the mother’s genital secretions, transmission in breast milk, and via the transfusion of infected blood products. Of these routes, breast milk is reported to be the most common route in very low birth weight (VLBW) infants [1]. pCMV infections are the most common and are generally less severe and less important than cCMV infections, with almost 90% of term neonates infected during the perinatal period being asymptomatic [2]. On the other hand, pCMV infections present a significant risk in preterm infants. Maternal anti-CMV immunoglobulin G acquired transplacentally after 34 weeks of gestation is thought to be protective [3]. pCMV infection in pre-term, VLBW infants can cause a sepsis-like illness, pneumonia, hepatitis, and blood abnormalities [4].
pCMV infections in VLBW infants are associated with longer term oxygen requirements, increased ventilator use days and moderate or severe bronchopulmonary dysplasia (BPD) [3, 5]. A prolonged CMV infection also often causes diffuse interstitial necrotizing pneumonia and cystic lung disease leading to fibrosis and exacerbation of BPD [2].
Here we report a case in which a VLBW infant was infected with pCMV via breast milk. Although the infection was treated with anti-CMV drugs, the patient had a poor outcome due to exacerbation of pre-existing chronic lung disease.
Case report
The patient’s mother was a 37-year-old nulliparous woman, who underwent a laparoscopic myomectomy for myomas 4 years prior to her pregnancy. One year after this initial surgery, she developed a uterine perforation and underwent surgical repair with two-layer suturing at the site of the perforation.
She was pregnant with monochorionic-diamniotic twins and at 27 weeks of gestation, complained of sustained abdominal pain for 12 h. The clinical condition of both the mother and fetuses deteriorated rapidly and an emergency caesarean section was carried out, at which point a complete uterine rupture was diagnosed. Two live male babies were delivered. The Apgar scores at 1 and 5 min were 1 and 1 for the elder of the twins (Twin A) and 0 and 3 for the younger of twins (Twin B). Their birth weights were 1203 g (+ 0.65SD) and 495 g (– 3.79SD), respectively. Both twins were intubated, ventilated, and admitted to the Neonatal Intensive Care Unit (NICU). They were fed unpasteurized and unfrozen breast milk that had been stored at 4°C for up to 24 h via nasogastric tube until day 7 of age. After day 7 of age, they were fed breast milk that had been frozen at – 20°C for at least 24 h. Twin B was accidentally extubated at 11 days of age and was reintubated 1 h later at which time he required resuscitation and suffered a left intraventricular hemorrhage (Fig. 1). He was diagnosed with chronic lung disease at 17 days of age and treated with hydrocortisone, followed by dexamethasone at age 34 days. At age 37 days old, his oxygenation improved, and he was extubated and managed with CPAP.
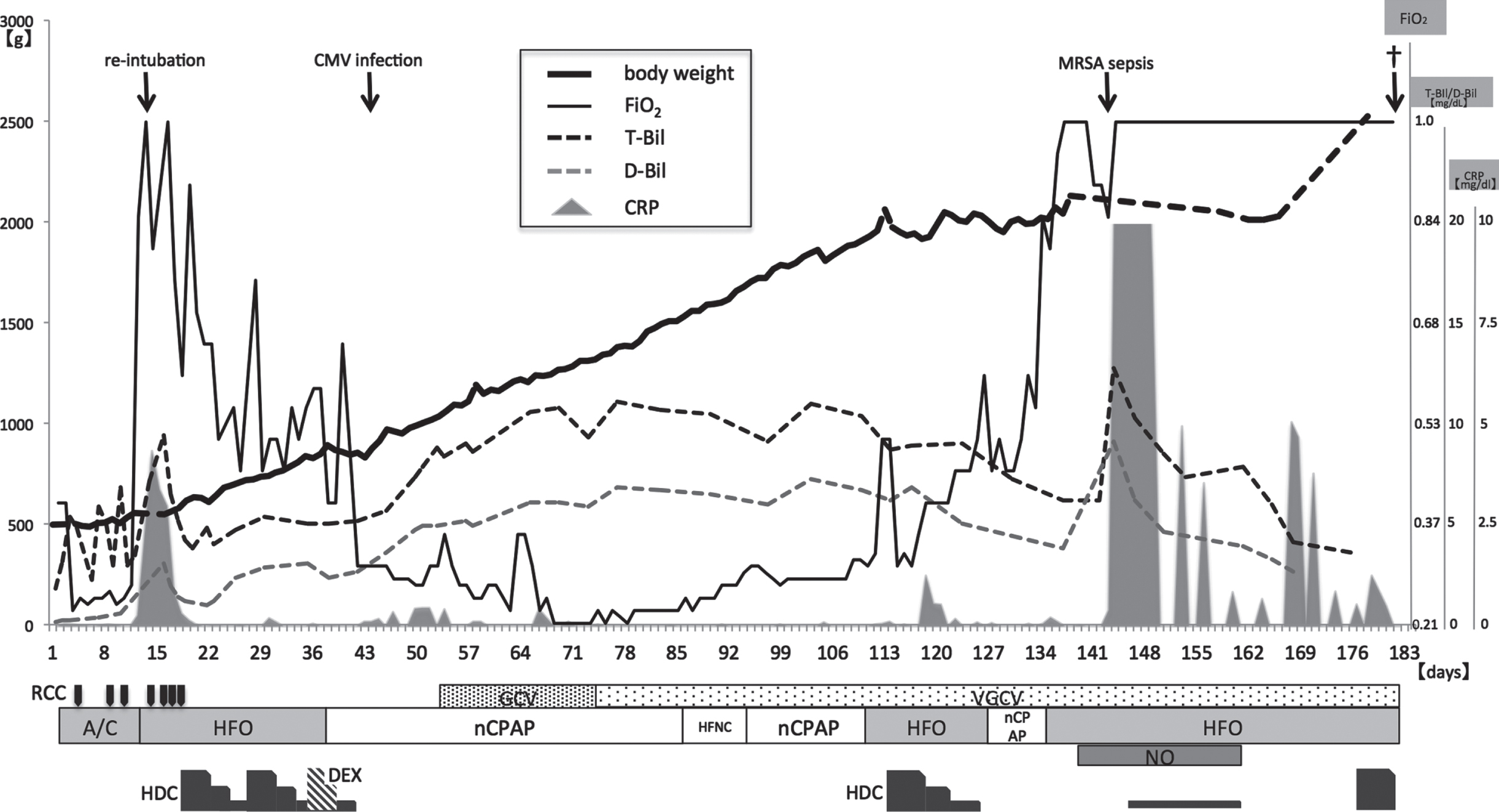
Clinical course in NICU. RCC, Red Cell Concentration; GCV, Ganciclovir; VGCV, Valganciclovir; A/C, Assist control; HFO, High frequency oscillation; nCPAP, nasal Continuous positive airway pressure; HFNC, High flow nasal cannula; NO, Nitric Oxide; HDC, Hydrocortisone; DEX, Dexamethasone.
On day 41, laboratory data showed a moderate elevation of CRP (0.12 mg/L maximum 0.46 mg/dL) with a thrombocytopenia (70×103/μL) and a small increase in the hepatic enzymes: aspartate aminotransferase (AST), alanine aminotransferase (ALT), and direct bilirubin (up to 142 IU/L, 112 IU/L and 7.0 mg/dL, respectively). All bacterial cultures were negative. CMV-specific immunoglobulin G (IgG) was positive (7.5 value), while CMV-specific immunoglobulin M (IgM) was negative (< 0.80 index) in the blood at day 41. CMV IgM converted to positive (2.3 index) at day 57, and CMV IgG increased more than fourfold to 30.8 value at day 71 (Table 1).
Twin B laboratory blood results
CMV qPCR, cytomegalovirus quantitative polymerase chain reaction; CMV IgM, cytomegalovirus immunoglobulin M; CMV IgG, cytomegalovirus immunoglobulin G; ND: not done.
CMV quantitative polymerase chain reaction (qPCR) test was positive both in urine (59,000 copies/mL) and in the blood (5,000 copies/mL) on day 41. CMV qPCR testing of his stored, dried umbilical cord was negative, while the CMV qPCR in the breast milk was positive (900 copies/ml).
This together with the fact that only seronegative blood products were transfused, led to a diagnosis of breast milk-acquired postnatal CMV infection. Ganciclovir was administered intravenously from day 52 to 73. CMV PCR testing performed at day 71 showed that the amount of CMV DNA in the blood and urine had decreased but not disappeared (Table 1), and therefore CMV treatment was switched to valganciclovir on day 74. On day 111, Twin B’s respiratory condition worsened, and he was re-intubated. He was diagnosed with acute exacerbation of BPD (Fig. 2) and pulmonary hypertension and treated with steroids and antibiotics drugs. Nitric oxide inhalation therapy was given from day 139, without any improvement. On day 146, a methicillin-resistant staphylococcus aureus (MRSA) strain was isolated from the patient’s tracheal secretions and blood, and the patient was treated for MRSA sepsis and pneumonia with antibiotics and γ-globulin (Fig. 1). Unfortunately, his condition did not improve, and he died on day 182 due to multiple organ failure. Twin A was discharged from the hospital in good health on day 100.
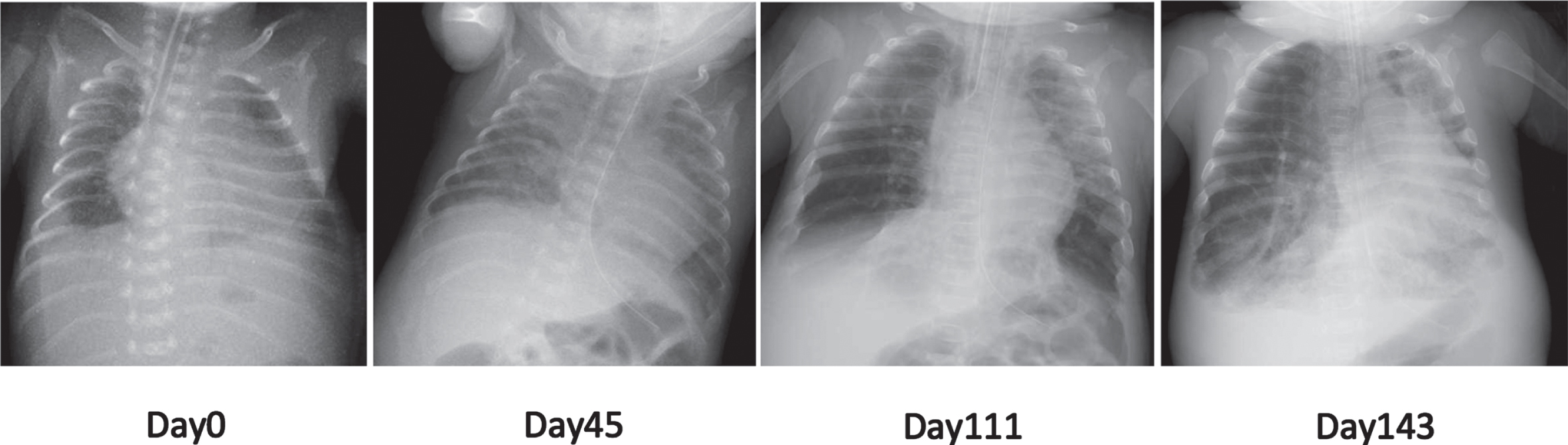
Chest radiograph. Granular shadow with mild respiratory distress syndrome (day0), bilateral hazy appearance (day45), emphysema and atelectasis (day111), exacerbation emphysema and fibrous appearance (day143).
Here we report on a case of a preterm infant diagnosed with breast milk-acquired postnatal CMV infection and who developed BPD during his NICU admission period.
Although reported infection rates from breast milk vary, Kurath et al. reported that the rates of transmission, symptom development, and infection severity from breast milk in VLBW infants were about 20%, 3.7%, and 0.7%, respectively [6]. The incidence of symptoms in preterm infants with pCMV infection from breast milk is higher compared to full term neonates, and the more preterm the birth, the higher the infection rate [3].
Raw breast milk has several advantages over formula, including anti-inflammatory and anti-infective properties [1] and is therefore the optimal nutrition for infants. It is however, also the primary cause of acquired CMV infection [6]. Methods to reduce CMV transmission risk from breast milk include freezing and pasteurizing. Freezing reduces the amount of CMV without losing the nutritional properties of breast milk while pasteurization reduces the risk of CMV infection in breast milk significantly but affects its nutritional and immunological properties [1].
French neonatal society contraindicates raw breast milk feeds in preterm infants born to CMV-positive mothers before a corrected age of 32 weeks or below a weight of 1,500 g, and recommends feeding with pasteurized maternal milk in order to reduce the CMV transmission risk [7]. The American Academy of Pediatrics (AAP), for example, recommends that all preterm infants receive nutritional support through fresh or frozen breast milk and does not contraindicate fresh breast milk for preterm infants [8]. There is therefore no worldwide consensus on the administration of raw breast milk to preterm infants.
CMV excretion in the breast milk of CMV positive mothers begins in small amounts and gradually increases with mammary gland activity. The onset of excretion into breast milk is variable but peaks at around 4 to 8 weeks postpartum. It is usually excreted in breast milk by day 10 post-partum, but has been reported in colostrum from day 3 post-partum [9, 10] leading to the potential for symptomatic CMV infection and disease development in preterm infants via raw milk [10].
According to some previous studies, the median age of onset of CMV infection after breastfeeding is 50 days after birth [3, 11]. Considering that the incubation period of CMV infection is 4 to 12 weeks (average 8 weeks) [12], it is possible that many breastfed infants are infected by the CMV in breast milk early in life and develop the disease after an incubation period rather than through cumulative viral exposure. Recent reports recommend that pasteurized mother’s own milk or pasteurized another mother’s milk (Human milk bank) rather than the raw mother’s colostrum, be used after 3 days of age in preterm infants due to the risk of infection from colostrum [7, 10] and that the early use of raw breast milk for preterm infants should be done with careful consideration.
Acute CMV pneumonia often requires prolonged ventilator support and increased oxygen administration, which are known to be associated with the development of BPD. Suzumura et al. described a VLBW infant who developed interstitial pneumonia secondary to a CMV infection at two months of age with a progressive deterioration in respiratory function, hyperinflation with chest radiograph showing reticular shadows similar to that of cystic lung disease in preterm infants [13].
There are several plausible mechanisms by which pCMV infection might increase the risk of BPD. Damage to lung tissue may occur as a direct result of viral infection or indirectly through the immune response to the virus. CMV infection in neonates often causes chronic viral replication and may play an indirect role in BPD by increasing exposure to other causative factors. On the other hand the development of BPD may also be related to the direct effects of CMV infection on the lungs, as CMV can cause a diffuse necrotizing pneumonia with fibrosis that confirms the development of BPD [2].
In particular, the inflammatory cytokine IL-6 is known to stimulate the expression of CMV immediate early type proteins and trigger inflammatory processes [14]. Therefore, active CMV infection may promote the development of BPD, and CMV replication processes may be stimulated by inflammation in the BPD lung. CMV infection is linked to increased morbidity and mortality in patients treated with immunosuppressive drugs and steroids, for example organ transplant recipients. Based on autopsy findings of secondary interstitial pneumonia, Andrade et al. reported that CMV pneumonia is a common cause of severe lung disease in immunosuppressed children [15]. Patients treated with immunosuppressive drugs are at higher risk of CMV infection, while inflammation itself predisposes to CMV infection as CMV favors replication in cells of granulation tissue [16]. It is possible that steroid therapy as well as active inflammation and repair processes may have predisposed Twin B to both the development and the severity of his CMV infection. In our case, we suspect that the persistence of CMV-DNA in Twin B’s serum and urine even post treatment with anti-CMV drugs indicated an ongoing acquired CMV infection that contributed to his lung tissue damage. The incidence and severity of CMV pneumonia in immunosuppressed children are higher than in healthy children, and it is possible that immunosuppression secondary to steroid use in this patient caused a prolonged CMV infection and exacerbation of pre-existing BPD. However, it remains unclear whether CMV caused direct damage to the lungs or if the systemic CMV infection led to an inflammatory response in the alveoli, which in turn exacerbated his underlying BPD.
Although there are a few case reports regarding the treatment of pCMV, no clinical trial data exists. Ganciclovir is usually used to treat cCMV, but recently oral valganciclovir has been shown to be as effective as ganciclovir in the treatment of cCMV [17]. Monitoring of blood CMV-DNA viral load during treatment is useful for assessing the efficacy of antiviral agents, and complete suppression of the virus is usually associated with disease cure. Kadambari et al. recommend that the pCMV treatment regimen consist of 2 weeks of anti-viral treatment, followed by a further 2 weeks of treatment post symptom resolution and an undetectable CMV-DNA viral load. Treatment for longer than 8 weeks is however rare [18].
Twin B was treated with ganciclovir for 3 weeks starting from 52 days of age. Ganciclovir administration is typically effective in treating CMV infections in preterm infants. In our case, treatment was changed from ganciclovir to valganciclovir for an additional 8 weeks, but CMV-DNA in blood and urine remained detectable.
Takahashi et al. [19] reported that intravenous immunoglobulin containing high titers of anti-CMV antibodies was effective in the treatment of pCMV infection and can reduce the need for prolonged valganciclovir use.
Conclusion
pCMV is a significant cause of mortality and morbidity in preterm VLBW infants and may lead to the exacerbation of BPD. A common route of infection is via CMV positive breast milk and therefore the early use of raw breast milk in preterm infants should be carefully considered. A treatment protocol for pCMV infected infants need to be established to provide standardized care based on the latest evidence.
Footnotes
Statement of ethics
IRB approval was not required for this study.
Written informed consent was obtained from the patient’s parents to publish this report.
Disclosure statement
This study was not supported by any grants.
Conflict of interest
The authors declare no conflict of interest.