
Abstract
BACKGROUND:
Most neonates have neonatal jaundice, with 5–15% requiring phototherapy. Although phototherapy is beneficial, it can potentially extend hospital stays and cause harm. This study’s purpose was to analyze the effects of fenofibrate and phototherapy on total serum bilirubin (TSB) levels at 24 and 48 hours (primary outcome) after intervention. Furthermore, the phototherapy duration and adverse events were also of interest (secondary outcome).
METHODS:
The study protocol was registered in the PROSPERO database. Articles were searched on EMBASE, PubMed, Cochrane Library, and Google Scholar. Study selection was done following PRISMA and risk of bias studies were conducted. The Review Manager 5.4 was used for the meta-analysis.
RESULTS:
Nine studies, including 610 newborns, were identified and included in the meta-analysis. This meta-analysis discovered a significant change in TSB levels at 24 hours after intervention (mean difference (MD) –0.96 (95% CI –1.09, –0.83), p < 0.00001) with low heterogeneity and at 48 hours after intervention (MD –1.75 (95% CI –2.26, –1.24), p < 0.00001) with high heterogeneity. Significant shortening of phototherapy duration was observed in the interventional group (MD –15.28 (95% CI –20.65, –9.90), p < 0.00001) with high heterogeneities. One of the nine studies reported a non-significant occurrence of abdominal distension and diarrhea in the fenofibrate group.
CONCLUSION:
Fenofibrate might be applied as an adjuvant in unconjugated neonatal hyperbilirubinemia to reduce the average total serum bilirubin and shorten the length of phototherapy.
Introduction
Neonatal jaundice is a significant health concern globally [1, 2]. If left untreated, it can result in neonatal mortality or grave morbidities such as temporal and occipital lobe seizures and kernicterus, commonly known as bilirubin encephalopathy. Kernicterus causes lifelong brain injury along with feeding difficulties, aberrant crying, tone abnormalities, and kernicteric facies [3, 4]. Neonatal jaundice is a concern of parents and physicians because of the associated risk of financial burden and prolonged hospitalization [5].
Numerous non-pharmacological and pharmacological approaches exist in hyperbilirubinemia therapy. Phototherapy has become the most often used non-pharmacological approach for preventing and treating unconjugated neonatal hyperbilirubinemia. This is due to its simplicity, low cost, non-invasiveness, and ease of use [6, 7]. The water-soluble form of bilirubin generated from phototherapy is relatively simple to eliminate and lowers the TSB levels. When the blue-green spectrum lights with wavelengths ranging from 425–475 nm react biochemically with the bilirubin accumulated on the skin of jaundiced neonates [8]. Despite being widely used to treat unconjugated neonatal hyperbilirubinemia, fever, loose stools, dehydration, and the possibility of retinal damage are all adverse effects of phototherapy [9]. Phototherapy may also disrupt breastfeeding and the maternal-neonatal bond [10].
Fibrates, such as clofibrate and fenofibrate, are phenoxyisobutyric acid derivatives primarily used as antihyperlipidemic agents and can also be used to manage hyperbilirubinemia. Fibrates contribute to the treatment of neonatal hyperbilirubinemia through various methods. The majority of its action is through the upregulation of enzymes associated with the metabolism and excretion of bilirubin. Fibrate-mediated activation of PPAR-alpha assists the conjugation and elimination of bilirubin by increasing the activity of UGT enzymes. Moreover, fibrates stimulate the expression of organic anion transporters which facilitate the excretion of conjugated bilirubin into the neonatal bile [11].
The fenofibrate mechanism of action is equivalent to that of clofibrate. However, fenofibrate has a more favorable safety profile compared to clofibrate in neonates [12]. There has yet to be an update on the use of clofibrate in neonatal jaundice, considering the latest disclosure of the Cochrane meta-analysis (2019). Due to safety concerns, it no longer appears in the market in some countries [13].
Therefore, we intended to conduct a systematic review and meta-analysis to analyze the impact of the combination of fenofibrate and phototherapy compared to phototherapy only on bilirubin levels (following the initiation of phototherapy), phototherapy duration, and aftermath of fenofibrate as a treatment for neonatal unconjugated hyperbilirubinemia.
Methods
Eligibility criteria
The PRISMA guidelines were utilized as the checklist for this study. The study protocol was also registered on PROSPERO (CRD42023467846). The inclusion criteria were made according to PICOS, they were as follows: the study population was neonates with unconjugated hyperbilirubinemia. The intervention group received fenofibrate with phototherapy and the control group received placebo with phototherapy or phototherapy alone. The primary outcome of the study was total serum bilirubin (TSB) at 24 and 48 hours after the intervention and the secondary outcomes were mean duration of phototherapy and adverse effects of fenofibrate. Only randomized controlled trials whose full-text publication is accessible would be included.
The exclusion criteria were (1) observational studies with control (cohort or case-control) or without control (cross-sectional studies or case series); (2) studies not in English; (3) studies of prophylactic phototherapy; (4) unpublished abstracts; and (5) non-primary research.
Search strategy
Literature was systematically searched in four databases (EMBASE, PubMed, Cochrane Library, and Google Scholar) using two approaches: single-database and cross-database. The data was updated up to September 18th, 2023. The following keywords were utilized in the search: “hyperbilirubinemia”, ‘’jaundice”, “fenofibrate”, and “phototherapy”. The use of operators (AND, OR) and adjustments for the specific search criteria of each database were done. A manual search was also conducted on each of the reference lists of the included studies. The search strategy and the respective databases can be found in the supplementary materials.
Study selection
Two researchers (AVW, ALZ) independently screened the study titles and abstracts. They also evaluated the selected articles for full-text review and assessed their eligibility. Any disagreements were resolved by consulting with the third member of the review team (RKL).
Data extraction
The study details included the first author, year of publication, study type, country, sample size, study population, fenofibrate dosage, and outcome. All data were retrieved and input independently into Microsoft Excel spreadsheets by two researchers (AVW, ALZ). Discrepancies were settled by discussion or, if necessary, consultation with the third member of the review team (RKL). When details were not accessible in published publications, we contacted authors for further information or clarifications.
Study risk of bias assessment
Two authors (AVW, ALZ) used RoB 2 and Review Manager 5.4 [14] to assess the risk of bias from all studies. The third reviewer (RKL) was involved in mediating any possible disagreements. The two authors also independently assessed other kinds of biases, such as selection bias, performance bias, and others (AVW, ALZ). The assessment results are classified into high, low, or undetermined.
Data synthesis
The Review Manager 5.4 (Cochrane Collaboration) software was used for meta-analysis. The Inverse Variance method with random-effects models measured the mean difference (MD) and the standard deviations (SD). Heterogenicity was measured with I2 and the results were divided into three groups: <25%, 26–50%, and >50%, consecutively defined as low, moderate, and high degrees of heterogenicity. Results were considered significant if the two-tailed p-value was ≤0.05. The meta-analytical pooling method from Wan et al. was used to transform the obtained median and interquartile range data to mean and SD [15].
Assessment of publication bias
Examination of publication bias using a funnel plot analysis typically requires a minimum of 10 studies. This is to ensure sufficient power to detect heterogeneity among studies. As such, a funnel plot will not be generated in this study. However, it is essential to acknowledge that the study may be susceptible to publication bias due to the limited number of available publications [14].
Results
Studies selection
A total of 225 articles were retrieved in the initial search from the databases. Among them, fifteen articles were removed as duplicates. Of the seventeen studies sought for retrieval, the full text of two articles were not retrieved. Six studies were then excluded out of the retrieved fifteen articles. Ultimately, nine records were included in this systematic review. A detailed PRISMA flow diagram for the study selection process is shown in Fig. 1.
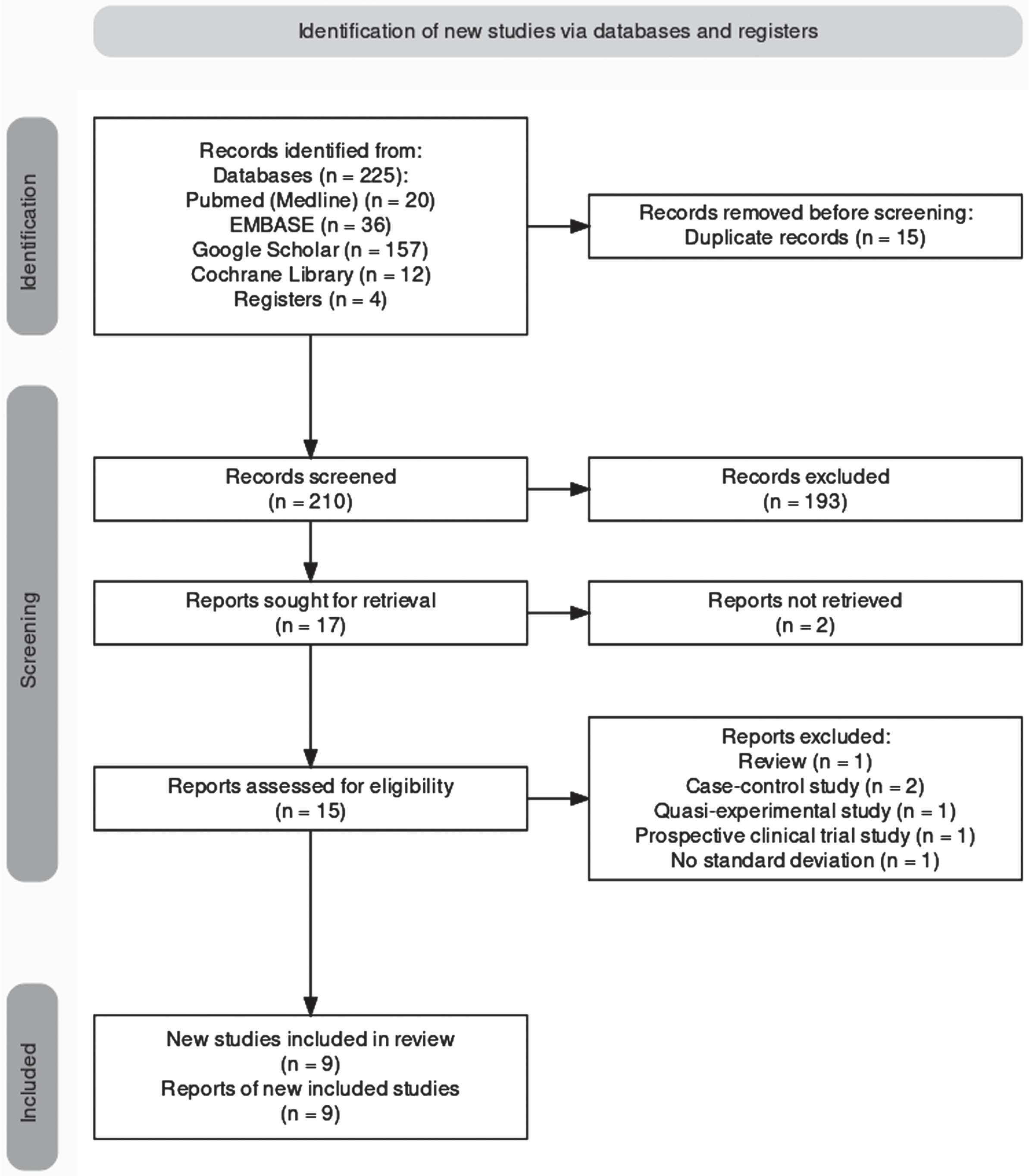
Diagram of PRISMA flow which demonstrated our process of the study selection.
Two studies were conducted in Iran [16, 17], three studies in Egypt [18–20], three studies in India [12, 22], and one study in Bangladesh [23]. The minimum and maximum number of participants was 40 [19, 22] and 180 [18]. All studies involved term neonates only, except for Chaudhary et al., who included both preterm and term neonates in their study. The control group received standard treatment (phototherapy) in the remaining studies. Except for Gohil et al., all the intervention groups received 10 mg/kg of fenofibrate. The extracted data and included studies’ characteristics are shown in Table 1.
Overview of study characteristics
Overview of study characteristics
*All studies used a single dose, 1: Bilirubin levels, 2: Duration of phototherapy, 3: Adverse effects of fenofibrate, 4: Number of exchange transfusions needed, 5: Number of intravenous immunoglobulins needed, RCT: Randomized controlled trials.
The visual representation of bias assessment is shown below as a risk of bias graph (Fig. 2) and table (Fig. 3). The assessment showed low to moderate results of bias. All studies used randomization, but details of the randomization method were unclear in three studies [19, 22]. Most of the studies also lacked details on allocation concealment [12, 21–23] and personnel blinding methods [6, 23]. Seven of the nine studies also had an unclear status of performance bias [6, 23]. Attempts were made to communicate with the respective authors of the studies mentioned above via email for further clarification, but no response was received.
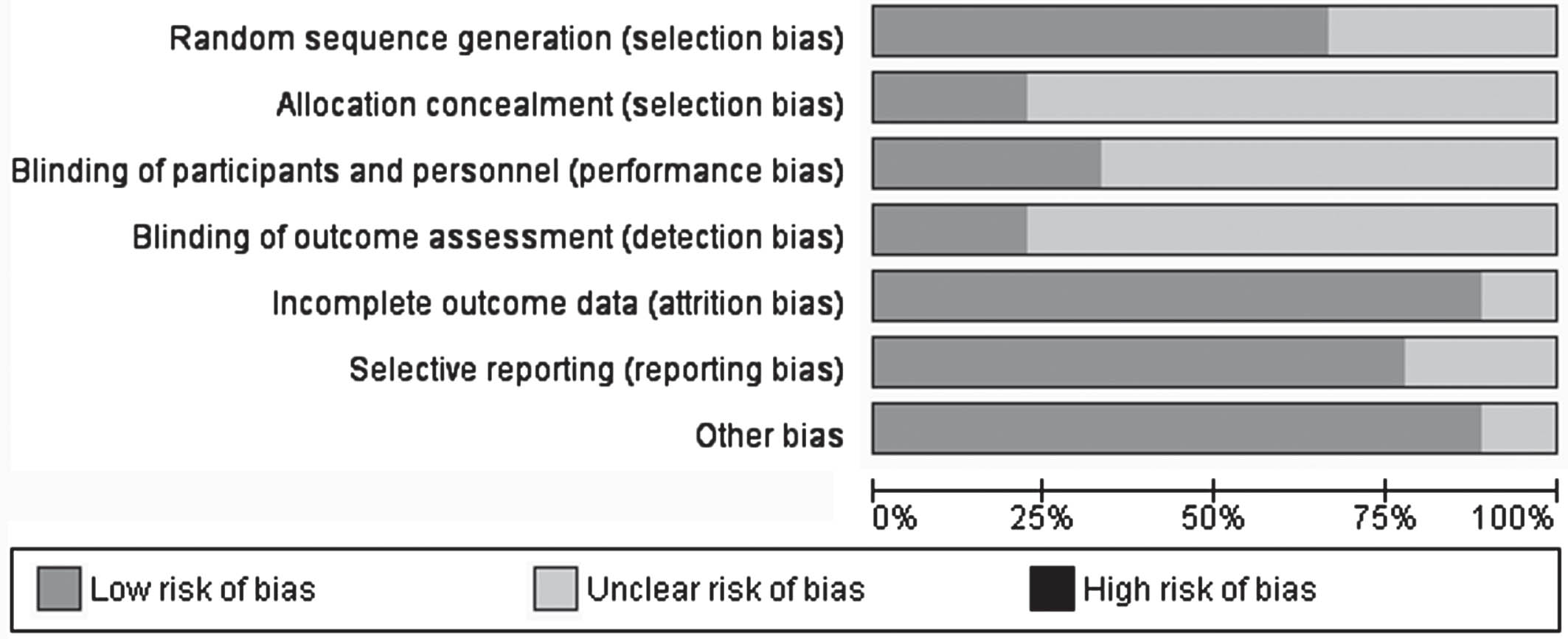
Graph for the risk of bias.
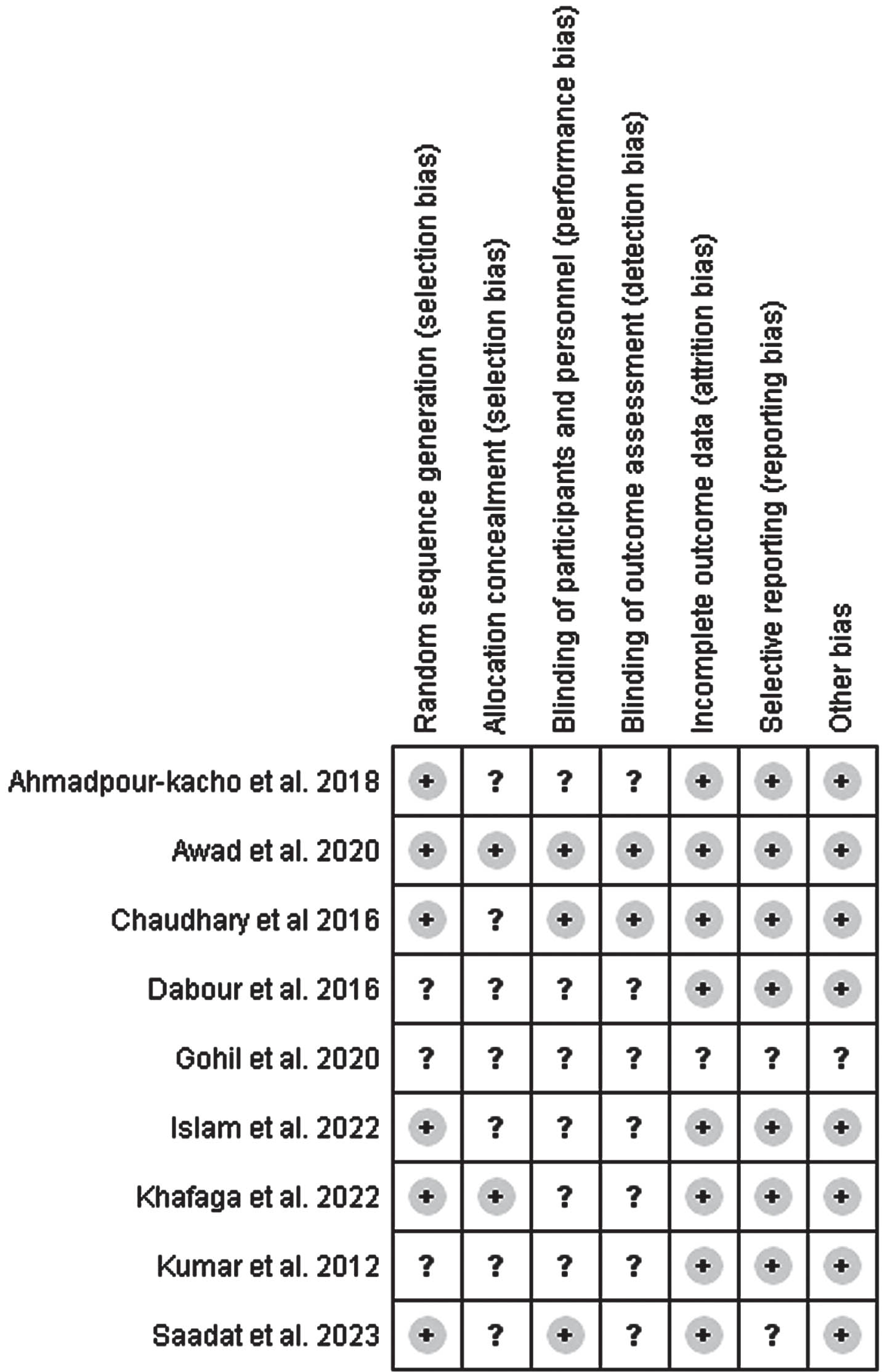
Summary of the risk of bias.
TSB (mg/dL) at 24 hours
All nine included studies (n = 610) reported TSB 24 hours after intervention. The pooled analysis showed that a significant decrease in TSB at 24 hours compared to control was associated with the fenofibrate and phototherapy combination group (MD –0.96 (95% CI –1.09, –0.83), p < 0.00001, random-effect model) (Fig. 4). Furthermore, the meta-analysis results for TSB at 24 hours exhibited a low degree heterogeneity (I2 = 0%).
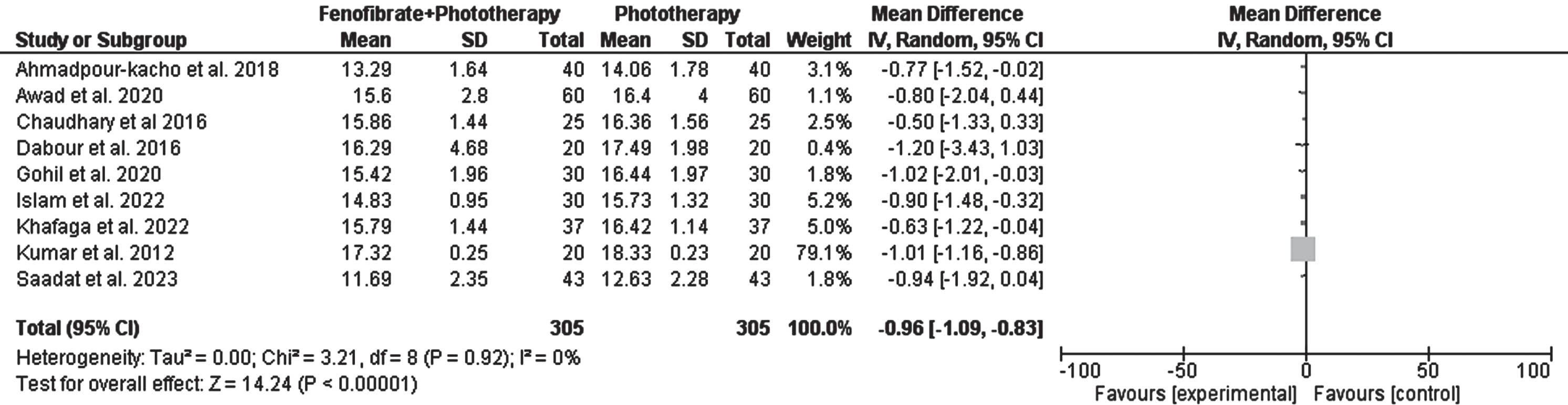
Forest plot for the effect of fenofibrate and phototherapy combination compared to control on Total Serum Bilirubin (TSB) after 24 hours.
All nine included studies (n = 610) reported the TSB 48 hours after intervention. The pooled analysis showed that a significant decrease in TSB at 48 hours compared to control was associated with the combination of fenofibrate and phototherapy combination group (MD –1.75 (95% CI –2.26, –1.24), p < 0.00001, random-effect model) (Fig. 5). Furthermore, the meta-analysis results for TSB at 48 hours exhibited a high degree heterogeneity (I2 = 82%). In sensitivity analysis, we removed two studies, Gohil et al. (used 100 mg/kg fenofibrate) and Chaudhary et al. (preterm and term populations), which still showed high heterogeneity.

Forest plot for the effect of fenofibrate and phototherapy combination compared to control on Total Serum Bilirubin (TSB) after 48 hours.
Duration of phototherapy (hours)
Only seven of the included studies (n = 530) reported the duration of phototherapy. The pooled analysis showed that a significant shortening of phototherapy duration compared to the control group was associated with the fenofibrate and phototherapy combination group (MD –15.28 (95% CI –20.65, –9.90), p < 0.00001, random-effect model) (Fig. 6). Furthermore, the meta-analysis results of phototherapy length exhibited a substantial degree heterogeneity (I2 = 82%). In sensitivity analysis, we removed two studies, Gohil et al. (used 100 mg/kg fenofibrate) and Chaudhary et al. (preterm and term populations), which still showed high heterogeneity.

Forest plot for the effect of fenofibrate compared to control on phototherapy duration.
The analysis of six studies concluded that no adverse effects were associated with fenofibrate treatment [6, 23]. However, one study reported abdominal distension and diarrhea in the fenofibrate group, but this was statistically insignificant [18].
Discussion
A 2022 Dutch study showed that around 72% of its participants (608 healthy neonates) were visibly jaundiced throughout their admission at the primary care birth centers. However, only 3.8% of neonates were indicated to receive phototherapy [24]. The prevalence of neonatal hyperbilirubinemia with bilirubin levels >6 mg/dL was 19% in an Italian study. Almost all the patients (99%) had a peak bilirubin level of less than 20 mg/dL (a level that is regarded as neurotoxic). Interestingly, the authors pointed out the sunny climate of the study location as a possible factor for the low incidence of hyperbilirubinemia [25].
This study included nine RCTs which involved 610 neonates. The analysis demonstrated that the combination of fenofibrate with phototherapy lowered total serum bilirubin levels at 24 and 48 hours after intervention. Data from seven RCTs involving 530 neonates showed adjuvant fenofibrate in phototherapy was effective and significantly lowered the duration of phototherapy by almost 15.5 hours compared to phototherapy alone.
The reduction in TSB at 24 and 48 hours after intervention and the 15.5-hour reduction in total phototherapy duration could be clinically relevant and helpful to patients. Moreover, these reductions could reduce the incidence of short and long-term adverse effects related to phototherapy [9, 10]. The shorter hospital stay may reduce expenditures associated with neonatal hyperbilirubinemia and allow for the distribution of healthcare resources. Studies have also discovered that neonates receiving phototherapy experience more breastfeeding difficulties [9, 26]. Spending less time in phototherapy and hospitalization may prevent such problems. However, the included original studies did not take these into account [27].
A previous meta-analysis of 4 RCTs showed that adjuvant fenofibrate in phototherapy had no significant effect on reducing serum bilirubin levels, which is inconsistent with our study. However, the prior meta-analysis did mention several study limitations, such as poor validity of the included studies and high data heterogeneity [28].
Fenofibrate belongs to the fibrates class of drugs, phenoxyisobutyric acid derivatives. Fenofibrate helps in neonatal hyperbilirubinemia through a variety of mechanisms, most of which include the activation of enzymes responsible for bilirubin metabolism and excretion. Through the activation of PPAR-α, fenofibrate promotes organic anion transporters, which in turn improves UGT enzyme production and facilitates bilirubin excretion into neonatal bile and subsequently [11].
Optimal fenofibrate dosing in neonatal jaundice remains to be determined. In this study, one study used a 100 mg/kg single dose while the rest used a 10 mg/kg single dose. We did not plan to do any subgroup analysis regarding the various dosages since the study conceptualization. We discovered that the research with the greater dose of fenofibrate [21] produced similar findings to those opting for a lower dose. As the majority of the trials in this meta-analysis reported no adverse effects, the fenofibrate dose with the best benefit-to-harm ratio remains unclear.
The statistical heterogeneity is a significant weakness of this meta-analysis, especially for “TSB at 48 hours” and “duration of phototherapy”. Although subgroup analyses (publication year and location) and the sensitivity analysis (removal of studies using fenofibrate at a dose of 100 mg/kg and studies with preterm and term neonate populations.) were conducted, the problem of heterogeneity remains. Possible reasons for variation included differences in baseline TSB upon admission, various causes of jaundice, phototherapy thresholds, different techniques of TSB testing, and genetic differences between populations. Another limitation of this study is that most of the included primary studies did not involve preterm neonates. Hence, the findings of this study cannot be applied to preterm neonates. We recommended that more clinical trials be conducted in preterm infants in future studies and that the source of heterogeneity be identified using meta-regression or other techniques.
Conclusion
In unconjugated neonatal hyperbilirubinemia, fenofibrate was found to work well when used in conjunction with phototherapy. Fenofibrate reduces the average bilirubin levels more quickly at 24 and 48 hours after the intervention. Fenofibrate administration was associated with a reduction of almost 15.5 hours in phototherapy duration. A significant outcome that would benefit patients. Large multicenter RCT trials, including pharmacological, cost-effectiveness, and safety analyses, are necessary before fenofibrate may be further considered as a feasible option in the traditional care of newborn hyperbilirubinemia.
Footnotes
Acknowledgments
The authors would like to thank everyone who contributed with article collecting, selection, and reading, as well as the paper’s writing and reviewing.
Conflicts of interest
The authors stated no conflict of interest.
Ethics approval
This article does not need to apply ethics.
Funding
This article got no financial, writing, or publishing help.