
Abstract
INTRODUCTION:
Lower motor neurons are the only neurons of the central nervous system (CNS) with the ability to regenerate without any intervention after an axotomy.
AIM:
This present study was conducted to analyze clinical and electrophysiological parameters in four groups of upper limb peripheral neuropathies, before and after treatment, comparing the results obtained after three cures of complex rehabilitation therapy.
MATERIALS AND METHODS:
We selected a number of 107 patients (66 women and 41 men) aged between 29 and 77 years (mean age = 49.6). Clinical (muscular strength, sensitivity) and electrophysiological parameters (accommodation coefficient α, nerve conduction velocity) were analyzed. All patients received 3 comprehensive treatment cures, each cure of 14 days and a rest period of 3 months between the cures.
RESULTS:
From the total of 107 patients included in the study, 52 were diagnosed with brachial plexus palsy, 27 with radial nerve palsy, 18 with median nerve palsy and 10 with ulnar nerve palsy. We did not observe a statistically significant difference between the mean age of males (47.2) and females (51.2) (p = 0.07), but peripheral neuropathies were more common in young males. At the end of the rehabilitation treatment all patients achieved better outcomes in muscle strength, sensitivity, adjustment coefficient α and nerve conduction velocity (p < 0.001).
CONCLUSION
The intervention of a physical therapy program in patients with peripheral neuropathies provided significantly better outcomes in clinical and electrophysiological parameters. Our rehabilitation protocol can be considered an alternative in order to stimulate and accelerate the nerve regeneration process.
Introduction
Lower motor neuron lesions affecting the upper limb is considered to be a multidisciplinary pathology, with severe neurological manifestations, as well as economic, professional, social and familial implications.
The lower motor neurons (LMNs) are the only neurons of the central nervous system (CNS) with the ability to regenerate without any intervention after an axotomy; this ability results from the environment surrounding these neurons and from the intrinsic regrowth property of motor neurons [22]. Their regenerative ability is impressive and involves all fibers of the peripheral nervous system. The sectioning a peripheral nerve triggers a series of histological and pathophysiological mechanisms (Wallerian degeneration of the distal segment, changes in the proximal segment, regeneration of nerve fibers) [7].
After a peripheral nerve lesion, from the proximal end budding fragments of new neurofilaments start to grow. The growth process takes place in the empty axonal cylinders from the distal tube. Therefore, axonal growth determines an activation of the Schwann cells, which play an important role in axonal regeneration [6]. Schwann cells proliferation is followed by the appearance of “Bungner bands” formed through the multiplication and disposition in parallel columns, bands that will create the needed network for the migration of nutrient and for growth. They cover the axons with a pluristratified layer that will eventually transform into a myelin sheath [5, 10].
Numerous studies have analyzed the mechanisms that determine the budding process. Many of these studies agree with the theory of sympathetic fibers sprouting after peripheral nerve lesions and with the intervention of neurotropic factors in the axonal regeneration process [1, 8].
Neurotrophic factors (neurotrophins) are specific proteins that induce neuronal survival, neuronal growth, synaptic plasticity and neurotransmission. The neurotrophins refer to the following factors: nervegrowth factor (NGF), the brain derived neurotropic factor (BDNF), the neurotrophin-3 (NT-3), and the neurotrophin-4/5 (NT-4/5). Many studies suggested that these neurotrophic factors have roles in specific axonal guidance during the growth and regeneration process of peripheral nerves [18].
In order to increase functional recovery following peripheral nerve injuries, a comprehensive planned program of medical and rehabilitation therapy must be initiated. As regards physical rehabilitation, a variety of methods are used in the treatment of upper limb peripheral neuropathies.
The present study was conducted to analyze clinical and electrophysiological parameters in four groups of upper limb peripheral neuropathies, before and after treatment, comparing the results obtained after three cures of complex rehabilitation therapy.
Hence, we designed a rehabilitation protocol in order to demonstrate that a comprehensive rehabilitation has an effect on the nerve recovery.
Materials and methods
This study took place between January 2011 and April 2016 at the Department of Balneophysiotherapy and Rehabilitation Medicine from the Emergency County Hospital in Timisoara.
The patients selected for the study need to fulfill the following criteria: (1) traumatic upper limb peripheral nerve lesions; (2) time until surgery less than 2 months (in patients that underwent surgical treatment); (3) no other associated diseases (metabolic, peripheral nervous system, chronic intoxications). A number of 107 patients (66 women and 41 men) with traumatic upper limb peripheral nerve injuries were selected. All patients gave their informed consent regarding their participation, agreeing to both evaluation and treatment. Clinical (muscular strength, superficial and profound sensitivity) and electrophysiological parameters (accommodation coefficient α, motor nerve conduction velocity) were analyzed.
Manual muscle testing (MMT) was used to determinate the muscular strength on a scale known as “0–5 scale” (by the National Foundation for Infant Paralysis). Moreover, we used the electro-diagnosis for the affected muscles and we determined the adjustment coefficient α. This coefficient reflects the degree of denervated muscle that will undergo electrostimulation. The α accommodation coefficient is defined as the ratio between the intensity of the triangular current with a duration of 1000 ms and the intensity of the rectangular current with the same duration, for values that produce a minimal contraction [9, 13]. In order to determine this coefficient we used the Siemens Universal – Neuroton 826, and as a work technique – the bipolar determination technique of the I/t curve (normal values of the α accommodation coefficient: normal innervation α= 2,5 – 6; partially denervated α= 1-2,5; completely denervated α< 1).
The nerve conduction velocity was performed with the aid of Keypoint – EMG/EP SySTEM manufactured by Alpine Biomed Corp. USA. The normal value for the nervous motor conduction velocity for the upper limb is 75 m/s.
All patients received 3 complex treatment cures, each cure of 14 days and a rest period of 3 months between the cures. Each patient received assessments before and at the end of each cure of rehabilitation treatment.
The patients underwent a complex treatment scheme, administered daily, at the same time and in the same order for the procedures: ultrasound treatment, thermotherapy (fango), electrostimulation of the partially or totally denervated muscles, kinetotherapy and massage. In the present study we chose to use our own protocol that includes the following procedures: Direct-coupled ultrasound therapy, in partly mobile field, with an intensity of 0,5 W/cm2 for 5 minutes, on the affected nerve. In this manner the profound micro-massage function of the ultrasound included the nervous fibers of the affected peripheral nerve; Thermotherapy (fango) in the areas innervated by the affected nervous roots, with a temperature of 40–42°C, for 15 minutes/session daily, with a stimulatory, excitatory and revulsive purpose; Electrostimulation, with exponential momentum, of the muscles that were partially or totally denervated, preceded by electrodiagnosis for the determination of the α adjustment coefficient; Electrostimulation of the muscles innervated by the affected peripheral nerve was performed daily, for 8 minutes/session, and the duration of the therapy was increased with 1 minute/session; Daily kinetotherapy sessions were adapted to the diagnosis of each patient. Intially, the patients underwent only 1 session/day, after that, they received 2 sessions/day; Manual stimulatory massage of the whole affected limb and especially massage of the cervical plexus emergence (antalgic and stimulation effect of the affected muscles). The sessions of manual massage took place daily, for 15 minutes, at the end of the daily therapeutic routine.
For all the patients included in the study we collected demographical data (age, sex, diagnosis, localization of the lesion), as well as specific parameters measured at the beginning and the end of each phase.
Descriptive statistics was used to describe the basic features of the data in this study. As descriptive statistics methods we used the average, the standard deviation, the median and the interquartilar distance (quartile 1 and 3) for numerical values, respectively proportions for qualitative variables. Student’s t test for paired or unpaired data was used to compare different data; ANOVA and Wilcoxon tests were used for numerical values, as well as the chi2 and Fischer tests. All tests were bilateral and the statistical significance p value was 0.05. For data visualization we used histograms and box plots.
Results
From a total of 107 patients included in the study, 52 were diagnosed with brachial plexus palsy, 27 with radial nerve palsy, 18 with median nerve palsy and 10 with ulnar nerve palsy. The mean age of the group was 49.6, varying between 29 and 77 years.
After centralizing the demographical data, we did not observe a statistically significant difference between the mean age of males (47.2) and females (51.2) (p = 0.07). However, men presented peripheral neuropathies at a younger age than women (Table 1).
Patient distribution depending on age and diagnosis (average values, median values, and quartiles Q1–Q3)
Patient distribution depending on age and diagnosis (average values, median values, and quartiles Q1–Q3)
Values are described as mean±standard deviation, median and interquartilar distance (quartile 1 and 3); *p≤0.05.
On the other hand we can state that there is a statistically significant difference between the four groups of upper limb peripheral neuropathies, as follows (Table 1): Patients with radial nerve palsy (average: 44.5 years of age) were younger than the rest of the patients in the study group (p = 0.01); Patients with median nerve palsy (average: 59.5 years of age) were older than the rest of the patients in the study group (p = 0.01); Patients with brachial plexus palsy and ulnar nerve palsy had similar ages (average: 50.2 and 50.0 years of age) (p = 0.01).
In all patients significant difference in muscular strength was observed at the end of the three treatment phases (p < 0.001) (Table 2).
Comparative analysis of muscle strength at the beginning and at the end of the three treatment phases (p < 0.001)
Values are described as mean±standard deviation, median and interquartilar distance (quartile 1 and 3); *p≤0.05.
We noticed that muscle strength generally improved with one stage during all three treatment phases (p < 0.001). Individual increase in muscle strength during each treatment phase was between 0 and 2 points, and global improvement for the three phases was between 2 and 3 points. Although the final effects of each phase are minor, the combined effect corresponds with a 3 point or higher improvement for more than half of the patients included in the study.
The maximal effect for one phase was obtained for phase 2, the difference between this and the other two treatment phases being statistically significant (p < 0.005, block-ANOVA test) (Fig. 1).
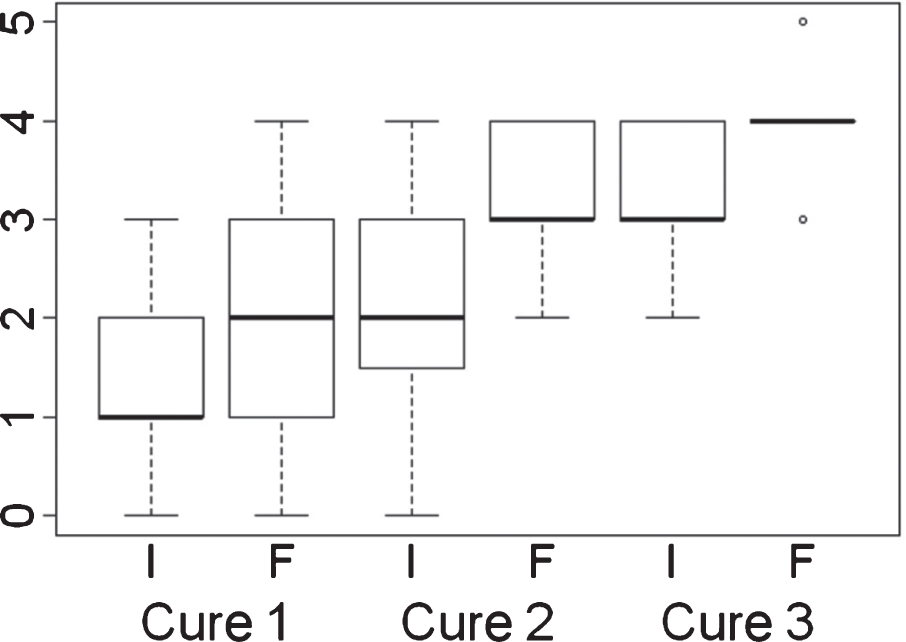
Comparative analysis of muscle strength at the beginning and at the end of the three treatment phases (p < 0.001).
Moreover, we found that all patients presented sensory symptoms in the affected upper limb. However, at the end of the whole treatment we observed a significant improvement in sensitivity in the affected upper limb (p < 0.001). The best results were noted at the end of phase 3 (Table 3) (Fig. 2).
Sensitivity evaluation for the affected upper limb – initial and final (p < 0.001)
Values are described as mean±standard deviation, median and interquartilar distance (quartile 1 and 3); *p≤0.05.

Sensitivity evaluation for the affected upper limb – initial and final (p < 0.001).
The α adjustment coefficient quantitatively assesses the degree of denervated muscle after a peripheral nerve injury. After the treatment, most patients presented a 0.5–0.7 increase in the adjustment coefficient values. During phase 1, the increase was 0.05–0.2, during phase 2 it was 0.1–0.3, and 0.2–0.3 during phase 3. This improvement was statistically significant (p < 0.001) (Table 4) (Fig. 3).
Evaluation of the adjustment coefficient – initial and final
Values are described as mean±standard deviation, median and interquartilar distance (quartile 1 and 3); *p≤0.05.

Evaluation of the adjustment coefficient – initial and final (p < 0.001).
Motor nerve conduction velocity (MNCV) for the affected peripheral nerves varied during the first phase between 23 and 50 m/s. This parameter was higher at the beginning of phase 2 and phase 3. At the end of the 3 treatment cures most of the patients presented a significant increase in nerve conduction velocity. Overall, during all treatment phases, nerve conduction velocity increased between 12–19 m/s. This improvement was statistically significant (p < 0.001) (Table 5) (Fig. 4).
Progression of motor nerve conduction velocity – initial and final (p < 0.001)
Values are described as mean±standard deviation, median and interquartilar distance (quartile 1 and 3); *p≤0.05.
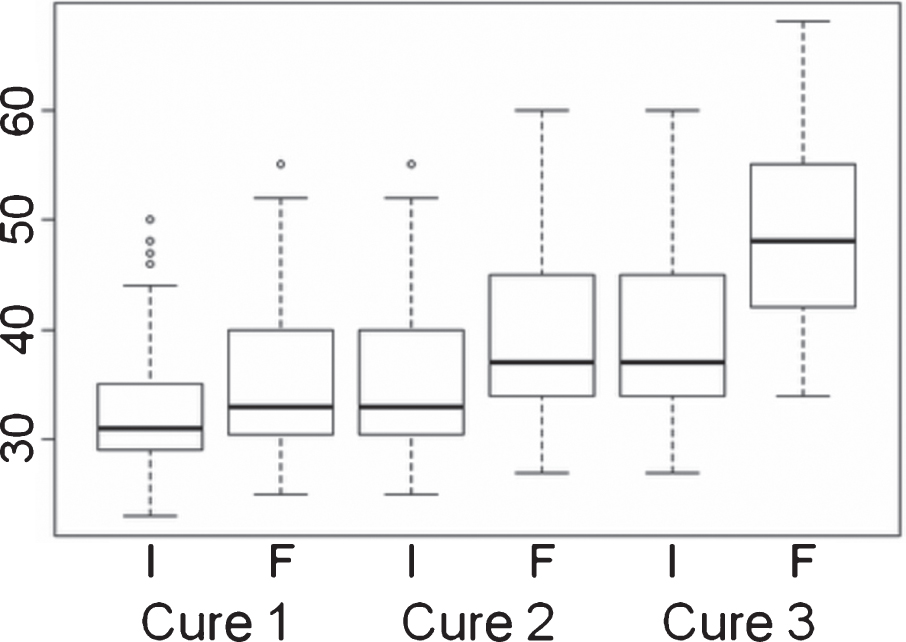
Progression of motor nerve conduction velocity – initial and final (p < 0.001).
The reactions of nervous tissues to trauma comprise of a sequential activation of degeneration and regeneration processes at the axon level.
Nerve growth factors (NGF) play an important role in the regeneration process by directly stimulating axonal regeneration. Understanding the way in which neurotrophic factors contribute to neuroprotection and regeneration after peripheral nerve injuries is challenging and represents the beginning of a new non-pharmacological therapeutic approach in neuropathies [1, 21].
It is notable that the regeneration rate is variable, depending on the nerve injury. The median nerve regenerates at a rate of 2–4.5 m/day, the cubital nerve at a rate of 1.5 mm, and the radial at a rate of 4-5 mm/day. On the other hand, the regeneration rate varies depending on the type of peripheral nerve lesion, being higher in the axonotmesis than in neurotmesis imjuries [15, 21].
The ability to manage the peripheral nerve regenerative processes at a cellular or genetic level is a future challenge for rehabilitation medicine. Therefore, the clinical and electrophysiological evaluation of peripheral motor neuron lesions of the upper limb is mandatory in order to set the localization and degree of nerve damage, as well as the proper therapeutic strategy.
This paper presents a rehabilitation protocol in which four groups of upper limb peripheral nerve injury patients participated. Taking into account the type of nervous lesion and the not so long time from the traumatic event (2 months), the aim of this protocol is to stimulate and accelerate the nerve regeneration process.
In order to achieve our goal we selected a number of 107 patients (66 female, 41 male), aged between 29 and 77 years (mean age = 49.6). From the total number of patients included in the study, 52 were diagnosed with brachial plexus palsy, 27 with radial nerve palsy, 18 with median nerve palsy and 10 with ulnar nerve palsy.
This study did not find a statistically significant difference between the mean age of males (47.2) and females (51.2) (p = 0.07), but peripheral neuropathies were more common in young males. Thus, our results coincide to other previous studies which showed that peripheral neuropathies are more frequent in young males [2, 20]. The difference between the genders can be explained by the fact that men get more often involved in physical work and are more exposed to accidents.
At the end of the rehabilitation treatment, both clinical and electrophysiological parameters improved. Although the effects of each treatment individually did not show spectacular results, the global effect led to the improvement of all parameters. Therefore, after analyzing the results we observed that the aforementioned parameters registered a statistically significant improvement during phase 3, regardless of the diagnosis.
In recent years, many studies evaluated the efficacy of rehabilitation techniques on clinical and electrophysiological parameters in upper limb peripheral neuropathies. Physical therapy modalities include pain modulators like hot and cold packs, ultrasound, low-power laser, TENS, transcutaneous electrostimulation and mobilization techniques. These have proven to be efficient in reducing pain, increasing muscle strength, sensitivity and peripheral nerve conduction velocity [4, 19].
In our study we proposed a protocol with the following procedures: ultrasound treatment, thermotherapy, electrostimulation of the partially or totally denervated muscles, kinetotherapy and massage. The results recorded at the end of the rehabilitation program confirm previous reports, above mentioned. All patients achieved better outcomes in muscle strength, sensitivity, adjustment coefficient α and nerve conduction velocity in the affected limb (p < 0.001) [4, 19].
Another finding of this study is that rehabilitation technique should be initiated as soon as possible after the trauma in order to avoid eventual pathologic regeneration (Wallerian degeneration) and the establishment of muscular hypotrophies or atrophies that would hinder rehabilitation of the limb. Thus, several authors demonstrated the importance of early rehabilitation therapy for good outcomes [3, 17].
The favorable results obtained allow us to state that our protocol could be proposed as an alternative in the rehabilitation therapy of upper limb peripheral nerve injuries.
Conclusions
The clinical and electrophysiological assessment of traumatic peripheral motor neuron lesions is mandatory to establish the location and the level of nervous damage, as well as a proper therapeutic strategy.
This protocol could have two effects in patients with peripheral nerve injuries: Nerve stimulation by producing supramaximal impulses leading to a motor response; Regeneration stimulation of the limb by promoting the tissue regrowth processes, by activating the metabolism and timulating cytogenesis.
The intervention of an early physical therapy program in patients with peripheral neuropathies provided significantly better outcomes in muscle strength, sensitivity, adjustment coefficient α and nerve conduction velocity of the affected limb.
Conflict of interest
All authors declare that they have no conflict of interest.