
Abstract
BACKGROUND:
Gastrointestinal dysfunctions are common in Parkinson’s disease. Their management is still challenging and new treatment options are needed.
OBJECTIVE:
To test whether transcutaneous vagal nerve stimulation can improve gastrointestinal dysfunction in patients with Parkinson’s disease.
METHODS:
We performed a randomized double-blind pilot study enrolling patients suffering from Parkinson’s disease with gastroenteric complaints. Patients were randomized to use either a sham-device or to stimulate the vagal nerve with an electric device over the course of four weeks with four stimulations per day. Ten patients (aged 69.6±4.6 years) were randomized for the intervention group, and nine patients (aged 67.2±6.3 years) used a sham-device. Clinical outcome was evaluated using the Gastrointestinal Symptom Rating Scale whereas gastrointestinal motility was measured with the 13C-octanoic acid breath test.
RESULTS:
In the treatment group, vagal nerve stimulation improved the Gastrointestinal Symptom Rating Scale comparing before and after stimulation (before, 8.7±6.09; after 5.67±3.08; p-value 0.48). This improvement was not observed in the sham group (before, 7.44±4.85; after, 5.67±3.08; p-value 0.16). In the 13C-octanoic acid breath test no significant changes were detectable.
CONCLUSIONS:
Vagal nerve stimulation is well tolerated with no side effects and may be a promising non-invasive therapy option to improve gastroenteric symptoms in Parkinson’s disease.
Abbreviations
Gastrointestinal Symptom Rating Scale
Enteric nervous system
Minimal Mental Status Examination
Parkinson’s disease
Unified Parkinson’s Disease Ranking Scale
Transcutaneous vagus nerve stimulation
Introduction
In the stomach, the myenteric plexus is directly connected to the vagal nerve, providing a direct neural link between the brain and stomach. The vagus nerve is integral to the control of gastric emptying, and the stomach is richly supplied by efferent and afferent vagal fibres (Marrinan et al., 2014) The aim of our study was to test whether tVNS is tolerated in patients with PD and gastrointestinal dysfunction.
Methods
We evaluated a randomized sham-controlled group of 19 patients with Parkinson’s disease and delayed gastric emptying in a double-blind pilot study in accordance with ethical standards on human experimentation and with the Helsinki Declaration of 1975, as revised in 1983. The study design was approved by the local ethics committee (No. 152/15).
To establish clinical baseline characteristics of the study population, we determined their UPDRSIII scores and Hoehn and Yahr stages. Ten patients (aged 69.6±4.6 years; 6 male/4 female; disease duration 4.8±4.7 years) were randomized for transcutaneous vagal nerve stimulation with the GammaCore® (electroCore LLC; Basking Ridge, NJ, USA) electric device for four weeks with four stimulations per day, and nine patients (7 female/2 male; aged 67.2±6.3 years; disease duration 3.±3,7 years) used a sham device. Symptoms were rated with the Gastrointestinal Symptom Rating Scale (GSRS) (Kulich et al., 2003); and gastrointestinal motility was measured with the 13C-octanoic acid breath test (Perri et al., 2005).
Results
The clinical characteristics of both groups showed no significant differences. PD patients allocated to the treatment group were, on average, 2.4 years older and suffered with PD 1.3 years longer than those allocated to the control group. The Hoehn and Yahr stages, UPDRSIII scores, levodopa dose and number of patients treated with dopamine agonists were almost identical between the two groups. A total of 112 vagal nerve stimulations were intended for the entire study period for each patient. The number of stimulations completed was similar in both groups (sham group, 100.33±16.14; treatment group, 94.10±14.44).
In the 13C-octanoic acid breath test no significant changes in either group were detectable (Table 1). In the treatment group, tVNS improved the sum GSRS score comparing before and after stimulation (before, 8.7±6.09; after 5.67±3.08; p-value 0.48; difference 3.0±4.14), and this improvement was not observed in the sham group (before, 7.44±4.85; after, 5.67±3.08; p-value 0.16; difference, 1.7±3.4; Fig. 1). The between-group comparison of the post-treatment scores of the sham and treatment groups did not reach the level of significance. Not all individuals applied the full number of stimulations, but the number of stimulations was not correlated with the outcome values.
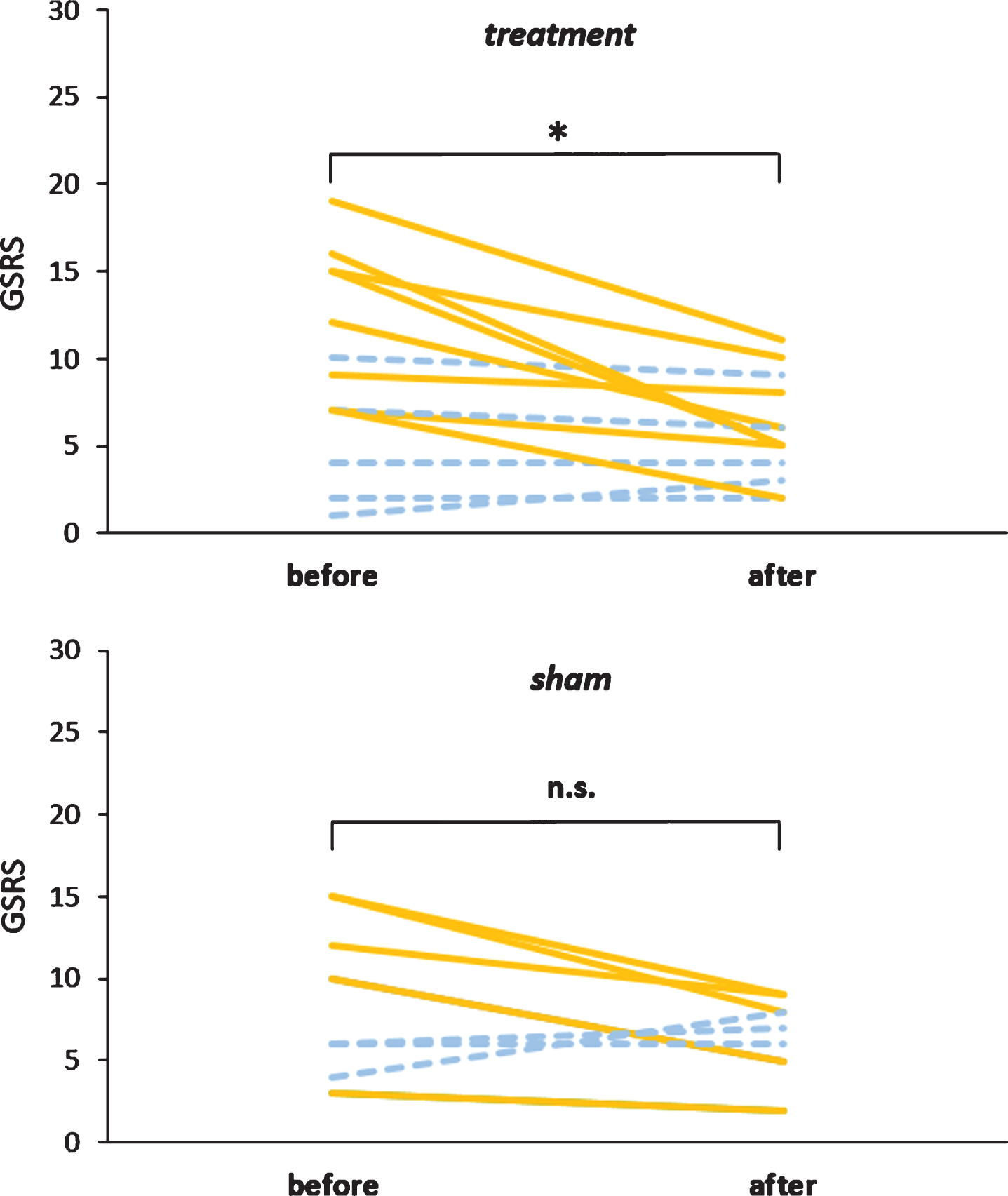
GSRS scores before and after treatment. GSRS scores were improved after tVNS treatment (p = 0.45), but many patients did not report a change after the treatment (dashed line). In the sham-treated group tVNS treatment resulted in an improvement of the GSRS in several patients without reaching the level of significance (p = 0.25), but also deterioration was reported (dashed lines).
Results of the 13C-breath test before and after treatment
Values are the median±SD. GEC, gastric emptying coefficient; higher values indicate clinically improved status. T lag [min] represents the “lag phase” until gastric emptying starts; thus, lower values indicate improvement. T½ [min.] gives the “half-emptying time”, and lower values indicate improved clinical conditions.
Only one patient who was allocated to the sham group reported an adverse event with skin alterations that remitted completely after usage of a skin cream.
Here, we demonstrated that transcutaneous vagal nerve stimulation is well tolerated and accepted in Parkinson’s disease patients with gastroenteric complaints. There was no change in the 13C-labeled breath test, whereas the self-rating score (GSRS) was improved in the treatment group. Although this was slightly significant it should be noted that our study is underpowered and we cannot claim to demonstrate positive effects of the intervention.
Recently, Hong et al. demonstrated that tVNS applied at the tragus of the ear can upregulate ghrelin levels in the blood and elevate the muscle action potential amplitude in the stomach of humans after open laparotomy (Hong et al., 2018). However, these effects were immediate three hours after tVNS. We speculate that tVNS affects the motility of the stomach in PD patients but only lasts for several hours. This would explain why the 13C-breath test, which was performed 24 h after the last stimulation, was not changed by the application of tVNS in our study.
It should be noted that vagal nerve stimulation also exerts effects within the brain via the solitary nucleus (NTS) and its projections (Schachter & Saper 1998). In a PD model of rats, vagal nerve stimulation increased locomotion, resulting in the increased expression of TH-positive neurons in the striatum and substantia nigra and decreased alpha-synuclein expression in the substantia nigra after only 10 days of stimulation (Farrand et al., 2017). The exciting findings of Farrand et al. suggest that tVNS may have potential as a disease-modifying treatment and should be further investigated in PD. Our findings are in line with the recent trend in PD management of using non-pharmacological treatments like tVNS as well as canonical pharmacological therapies. In summary, tVNS is well tolerated in PD patients with no relevant side effects and may be a promising non-invasive therapy option to improve gastroenteric symptoms in PD, but further studies with larger cohorts are warranted.
Conflict of interest
This research did not receive any specific grant from funding agencies in the public, commercial, or not-for-profit sectors. The authors have no conflict of interest to declare.
Footnotes
Acknowledgments
Special thanks to Regina Landeck for supervising the 13C-octanoic acid breath test.