
Abstract
BACKGROUND:
The Neurobehavioral Symptom Inventory (NSI-22) is a validated self-report measure designed to assess neurobehavioral symptoms (NBS) after mild TBI (MTBI). Psychological and behavioral factors have been shown to be predictors of persistent NBS reporting in veterans; however, there is still a gap in knowledge about these associations in a civilian population presenting for treatment.
OBJECTIVE:
This study seeks to identify the predictors of increased NBS reporting on the NSI-22 in a treatment-seeking population with MTBI.
METHODS:
Analysis of 80 treatment seeking participants admitted to an interdisciplinary outpatient rehabilitation program with a diagnosis of MTBI. NSI-22 was used to measure NBS reporting. Predictor variables identified by univariate analysis were entered into a multivariable regression model, which was adjusted for demographic variables.
RESULTS:
Higher NSI-22 scores correlated with increased level of depressive complaints (PHQ-9), higher disability (M2PI), lower satisfaction with life (SWLS), prior MTBI, fewer years of education, absence of motor vehicle collision (MVC), and unemployment at time of assessment. When those variables were used in a multivariable linear regression model, PHQ-9, M2PI, years of education, and absence of MVC remained statistically significant.
CONCLUSION:
Psychological factors and level of societal participation predicted increased NBS as compared with injury severity and time since injury.
Keywords
Introduction
Mild traumatic brain injury (MTBI), generally defined as a traumatically induced injury disrupting brain function with a loss of consciousness 30 minutes or less, posttraumatic amnesia less than 24 hours, and an initial Glasgow Coma Scale of 13–15 (American Congress of Rehabilitation Medicine, 1993), constitutes greater than 90% of overall TBI cases across all levels of severity (Leibson et al., 2011). While the majority of individuals recover within a few weeks after MTBI, an estimated 5% –43% of individuals experience persistent neurobehavioral symptoms (NBS) that restrict participation in a variety of personal and societal roles (Voormolen et al., 2018). In a substantial proportion of individuals, NBS after MTBI continue over a year after injury (Dikmen, Machamer, & Temkin, 2017; Hiploylee et al., 2017). These NBS, which include headaches, fatigue, dizziness, balance impairment, affective changes, and cognitive difficulties, often become characterized as post-concussive syndrome (PCS) when continuing beyond three months (Hiploylee et al., 2017; Polinder et al., 2018; Voormolen et al., 2018). Persistent NBS after MTBI are associated with lower quality of life, increased disability, and high health care service utilization, (Lange, Iverson, & Rose, 2011; Leibson et al., 2012), with up to 20% of individuals encounter significant difficulties returning to work years after MTBI (Cancelliere et al., 2014).
Symptom persistence after MTBI is associated with various premorbid psychological, behavioral, and personality factors. However, the extent to which these factors influence NBS in comparison to the physiological impact of the TBI remains unclear (Iverson, 2019). Symptoms of PCS are not specific to those who experience a MTBI and have been reported in healthy individuals with no history of MTBI (Iverson & Lange, 2003; Machulda, Bergquist, Ito, & Chew, 1998; Voormolen et al., 2019), and in individuals experiencing sequelae of major depression (Lange et al., 2011; Merz, Zane, Emmert, Lace, & Grant, 2019), chronic pain (Smith-Seemiller, Fow, Kant, & Franzen, 2003), PTSD (Belanger et al., 2016), and anxiety (Ponsford et al., 2012). Though multiple risk factors have been identified for developing PCS (Iverson et al., 2017; King, 2014; Zemek, Farion, Sampson, & McGahern, 2013), the diagnosis of PCS itself is controversial, with no validated diagnostic criteria for PCS and an absence of the diagnosis in the DSM-5 (Wortzel &Arciniegas, 2014).
The Neurobehavioral Symptom Inventory (NSI-22) is a self-reported questionnaire that was designed to better characterize persistent symptoms after MTBI (Cicerone & Kalmar, 1995). This scale is widely used in TBI evaluations within the Veterans Health Administration and the Department of Defense. PTSD and sleep impairment have been found to be associated with increased symptom reporting on NSI-22 in a sample of veterans (Andrews, Fonda, Levin, McGlinchey, & Milberg, 2018). Further studies in combat veterans has shown increased scores on NSI-22 to be correlated with PTSD (Belanger et al., 2016), depression, and generalized anxiety (King et al., 2012).
While psychological and behavioral measures are strong predictors of the variance reported on the NSI-22 in veterans, there is a gap in knowledge about these associations in a community-based, civilian population presenting for treatment. The primary aim of this study was to identify the predictors of increased NBS reporting on the NSI-22 in a treatment-seeking population with MTBI on admission to a multidisciplinary outpatient rehabilitation program. The study sought to determine the extent to which measures of depression, participation, and life satisfaction would predict the variation in NSI-22 scores as compared to measures of injury severity. We hypothesized that psychological and behavioral factors would have a greater influence on NBS as compared with injury severity, prior MTBI, mechanism of injury, and time since the injury.
Methods
This study was approved by the Mayo Clinic Institutional Review Board, and medical records were reviewed only for those individuals who gave authorization for their records to be utilized for research purposes. This was a retrospective data analysis of a community-based, treatment-seeking cohort with MTBI in a quaternary medical center between 2014 and 2018. All participants received interdisciplinary outpatient rehabilitation, with the specific therapy plan determined by clinical need. Admission to the outpatient rehabilitation program required the need for at least one ongoing therapy modality (Physical Therapy, Occupational Therapy, and Speech Language Pathology) following evaluation by a physician or certified registered nurse practitioner, and included ongoing interdisciplinary team rounds. Further neuropsychological, social services, as well as vocational rehabilitation evaluations were determined by the interdisciplinary team based on individual need.
Severity of TBI was classified using the Mayo Classification System (MCS) described in Fig. 1 (Malec et al., 2007). The classification system uses all data available in the medical record to identify evidence that fulfills the case definition of TBI: that an external mechanical force is associated with brain dysfunction. This system has been shown to be a more sensitive and specific classification of TBI severity compared to single indicators (e.g., loss of consciousness, initial Glasgow Coma Score, Post Traumatic Amnesia) (Leibson et al., 2011; Malec et al., 2007). In the MCS, each case of TBI is characterized into the following three categories: Definite (consistent with Moderate-Severe TBI), Probable (consistent with Mild), or Possible (consistent with Concussive) TBI. Important for this analysis, this classification system distinguishes severity within the MTBI spectrum (Possible vs. Probable) as seen in Fig. 1, which can allow for greater granularity to be made of the association between the severity of MTBI and reporting of NBS.
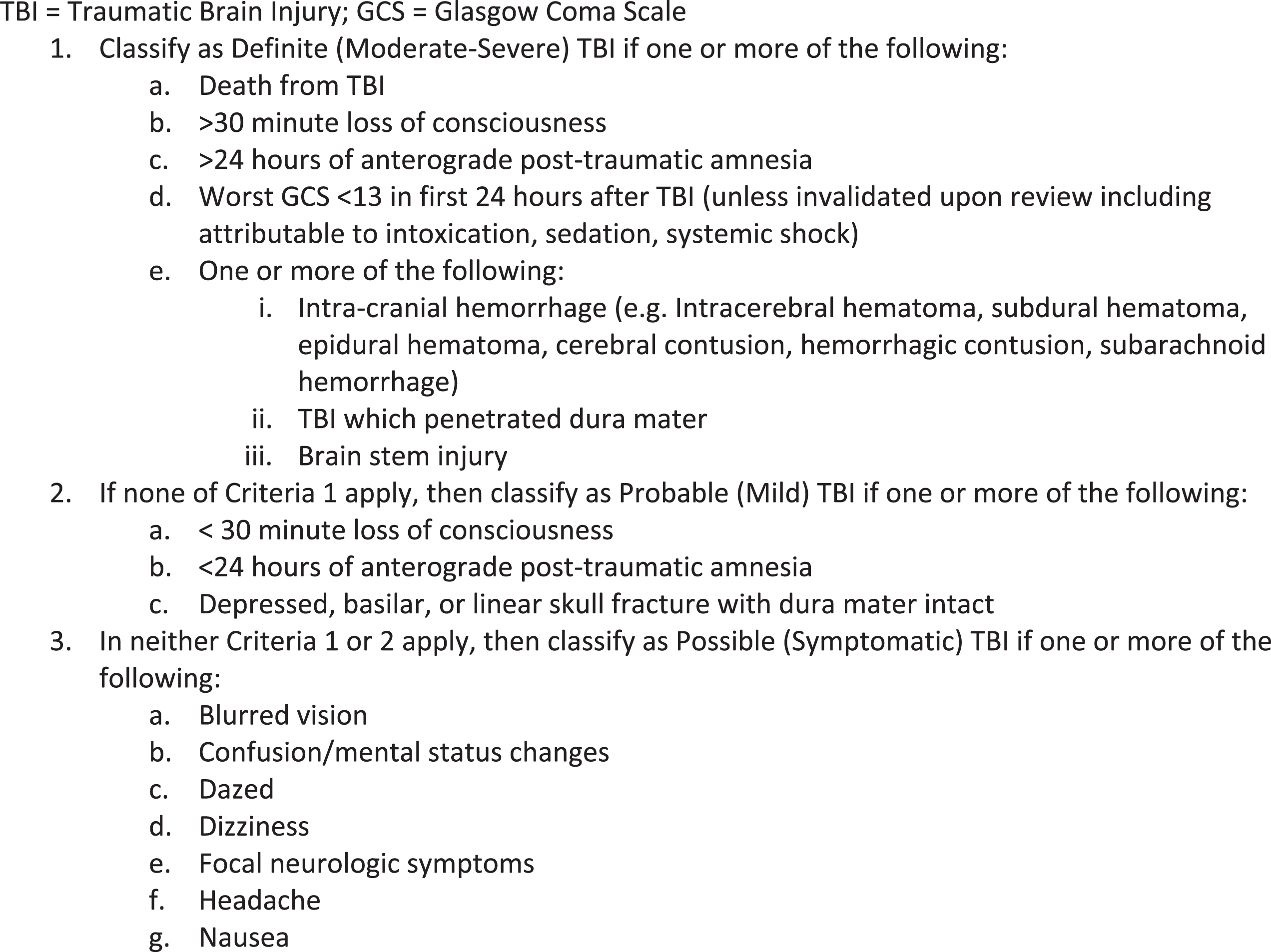
Mayo Traumatic Brain Injury Classification System. TBI = Traumatic brain injury; GCS = Glasgow Coma Scale.
Inclusion criteria included a diagnosis of Possible or Probable TBI, admission into the comprehensive outpatient rehabilitation program, and completion of all measures of interest on treatment admission, including demographic factors, years of education, current employment, as well as outcome measures regarding symptom severity (NSI-22), depression (PHQ-9), satisfaction with life (SWLS), and participation (M2PI). Exclusion criteria included a current or prior history of Definite TBI, or a diagnosis of acquired non-traumatic brain injury such as brain infarction (ischemic or hemorrhagic stroke), brain neoplasm, seizure disorder, anoxic brain injury, encephalopathy, or degenerative cognitive impairment.
Table 1 shows the predictor variables chosen for analysis in this study. Medical record review confirmed TBI severity, injury date, and demographic variables including age, gender (King, 2014), race, education and marital status at time of injury for this sample. Medical record review further assessed for a prior history of MTBI (Iverson et al., 2017), as well as a pre-injury history of chronic pain (Smith-Seemiller et al., 2003), ADHD (Zemek et al., 2013), PTSD (Belanger et al., 2016), mood disorder (Kumar et al., 2014), substance abuse (Bjork & Grant, 2009), sleep disorder (Andrews et al., 2018), and migraine headaches (Hiploylee et al., 2017). All conditions were required to be documented as conditions existing prior to the most recent MTBI. The mechanism of injury was also reviewed, documenting cases of MTBI caused by motor vehicle collision (MVC) vs. other mechanisms of injury. Studies have found associations between MVC and increased incidence of chronic pain conditions, prolonged symptoms, and psychological sequelae (Hartvigsen, Boyle, Cassidy, & Carroll, 2014; McLean, Clauw, Abelson, & Liberzon, 2005).
Demographic, program admission, and premorbid predictor variables
Abbreviations: TBI = Traumatic brain injury; MTBI = Mild traumatic brain injury; PHQ–9 = Patient Health Questionnaire; SWLS = Satisfaction with Life Scale; M2PI=Mayo-Portland Participation Index; PTSD = Post Traumatic Stress Disorder; ADHD = Attention-Deficit/Hyperactivity Disorder.
Neurobehavioral Symptom Inventory (NSI-22)
The primary outcome of interest was NSI–22 total score on admission. The NSI-22 has shown to be a valid assessment measure in characterizing symptom complaints after MTBI (Dretsch et al., 2016; Wilde et al., 2010). This scale consists of 22 questions scored on a Likert scale from 0 (no symptoms) to a score of 4 (severe symptoms). Score ratings are based on persistence of symptoms, the effect of symptoms on participation in societal roles, and the need for assistance. In the initial cluster analysis of the NSI-22, symptomatic complaints were subdivided into four non-overlapping clusters based on different symptom profiles: cognitive, affective, somatic, and sensory (Cicerone & Kalmar, 1995). Further studies have found a four-cluster profile - somatosensory, affective, cognitive, and vestibular subsets - to have the best overall psychometric fit (Meterko et al., 2012; Vanderploeg et al., 2015). Normative data have been developed within a cohort of National Guard members (Soble et al., 2014). However, these data have not yet been established in a civilian, treatment-seeking population. Based on prior subset cluster analysis, this study used the four symptom subset – somatosensory, affective, cognitive, and vestibular – and assessed for associations between each of these subsets as well the NSI-22total score.
The Validity-10 scale was developed as a measure to test for exaggerated NBS on the NSI-22 (Vanderploeg et al., 2014). This scale, which is embedded in the NSI-22 with a cut-off score above 22, has been validated for use in veterans (King et al., 2012; Lippa et al., 2016). Validity-10 scores have not been validated outside of the veteran population and have unknown utility in other clinical settings (Sullivan, Lange, & Edmed, 2016). Given that this was a community-based, treatment-seeking population, Validity-10 scores above the cutoff score were not used as exclusion criteria.
Patient Health Questionnaire (PHQ-9)
The PHQ-9 is a nine item, self-reported measure of the frequency and severity of depressive symptoms, that has been found to have adequate validity and reliability (Kroenke, Spitzer, & Williams, 2001). Increasing scores correspond with increasing severity of depression, with scores greater than 10 indicating moderate depression, and scores greater than 20 indicating severe depression. The PHQ-9 has further been shown to have sufficient utility as a screening tool for major depression in the TBI population, both within inpatient and outpatient clinical settings (Donders & Pendery, 2017; Fann et al., 2005). Cut-off scores of 10 or greater have been used to identify cases of major depressive disorder with good sensitivity and specificity (Kroenke et al., 2001; Terry, Brassil, Iverson, Panenka, & Silverberg, 2019).
Mayo-Portland Participation Index (M2PI)
The M2PI is an outcome measure focusing on participation in societal roles and community re-integration in post-acute rehabilitation programs (Malec, 2004). This is an 8-item self-reported assessment that measures initiation, social contact with friends and work associates, participation in leisure activities, independence in self-care, independent living and homemaking, independence in transportation, paid employment, and independence in managing finances. Each item is rated on a 5- point Likert Scale from 0 to 4, with higher scores indicating less participation and overall increased functional limitation.
Satisfaction with Life Scale (SWLS)
The SWLS is a widely used measure of perceived global life satisfaction that has been shown to have adequate psychometric properties (Amtmann et al., 2017; Diener, Emmons, Larsen, & Griffin, 1985). It is self-administered and includes five statements about life satisfaction on a 7-point Likert scale, where a score of 20 represents a neutral point, and with scores above that representing increasing life satisfaction. It has been used as an outcome measure in a number of studies in the TBI population (Corrigan, Kolakowsky-Hayner, Wright, Bellon, & Carufel, 2013; Davis et al., 2012).
Data analysis
Continuous variables are summarized as mean (SD) unless otherwise specified. Discrete variables are presented as frequency (percent). Linear regression models (both univariable and multivariable) were used to estimate associations between the NSI scores and proposed predictor variables. Predictor variables used in a univariate analysis can be seen in Table 1. NSI endpoints included both NSI-22 total scores as well as somatosensory, affective, cognitive, and vestibular subsets of the NSI-22 (Vanderploeg et al., 2015). Predictor variables identified to be statistically significant by univariate analysis for any of the NSI endpoints (total score or the 4 subsets) were entered into the multivariate regression models. Modeling results are presented as forest plots. For multivariate models, only variables significant at the 0.10 level are displayed. The estimated effects of continuous predictors are standardized to their inner quartile range so that effect magnitudes can be compared across both continuous and discrete variables.
Results
The study sample initially included 506 individuals with various acquired brain injuries and severities of TBI. There were 122 individuals identified with Possible or Probable TBI in the sample, with a total of 80 individuals meeting the inclusion and exclusion criteria. Table 2 shows demographic and clinical characteristics of the sample (n = 80) on admission to the rehabilitation program. The average age was 43 years old, with 55% of the sample having a diagnosis of Possible, as compared with Probable TBI. The majority (99%) of the sample were white, about 50% were married, and only 28% were males. Average years of education was approximately 15, and 41% were employed on admission. The median time between injury until admission to the rehabilitation program was 163 days. Eighty-three percent were found to have a prior history of a mood disorder, 35% with a prior MTBI, 38% with a history of chronic pain, 38% with history of migraine headache, and 44% with history of sleep disorder. Mean NSI-22 total scores was 34.1, and mean PHQ-9 scores was 11. Forty-six subjects (58%) reported at least a score of 10 on the PHQ-9, indicative of at least moderate depression (data not shown) (Kroenke et al., 2001; Terry et al., 2019).
Sample demographic and clinical characteristics (N = 80)†
Sample demographic and clinical characteristics (N = 80)†
†Unless otherwise indicated, numeric summaries are N (%) for discrete variables and mean (SD) for continuous variables. Abbreviations: TBI = Traumatic brain injury; MTBI = Mild traumatic brain injury; PHQ–9 = Patient Health Questionnaire; SWLS = Satisfaction with Life Scale; M2PI = Mayo-Portland Participation Index; PTSD = Post Traumatic Stress Disorder; ADHD = Attention-Deficit/Hyperactivity Disorder; NSI-22 = Neurobehavioral Symptom Inventory.
Figure 2 reports the results of the univariate analysis. Higher NSI-22 total scores were significantly correlated with higher depressive complaints (PHQ-9), higher level of disability (M2PI), lower satisfaction with life (SWLS), history of prior MTBI, fewer years of education, and unemployment at time of assessment. If a motor vehicle collision was the mechanism of injury, participants had significantly lower NSI-22 total scores. On analysis of NSI-22 clusters (data not shown), NSI-22 cognitive scores were significantly associated with PHQ-9, M2PI, SWLS, prior MTBI, and unemployment at time of assessment; NSI-22 vestibular scores were associated with PHQ-9, M2PI, SWLS, and unemployment at time of assessment; NSI somatosensory scores were associated with PHQ-9, M2PI, SWLS, as well as with prior MTBI, history of chronic pain, unemployment at time of assessment, and MVC as mechanism of injury; NSI-22 affective scores were associated with PHQ-9, M2PI, SWLS, fewer years of education and unemployment at time of assessment. Overall, both NSI-22 total and NSI subset scores were all associated with elevated PHQ-9 and M2PI, decreased SWLS, as well as unemployment at time of assessment.
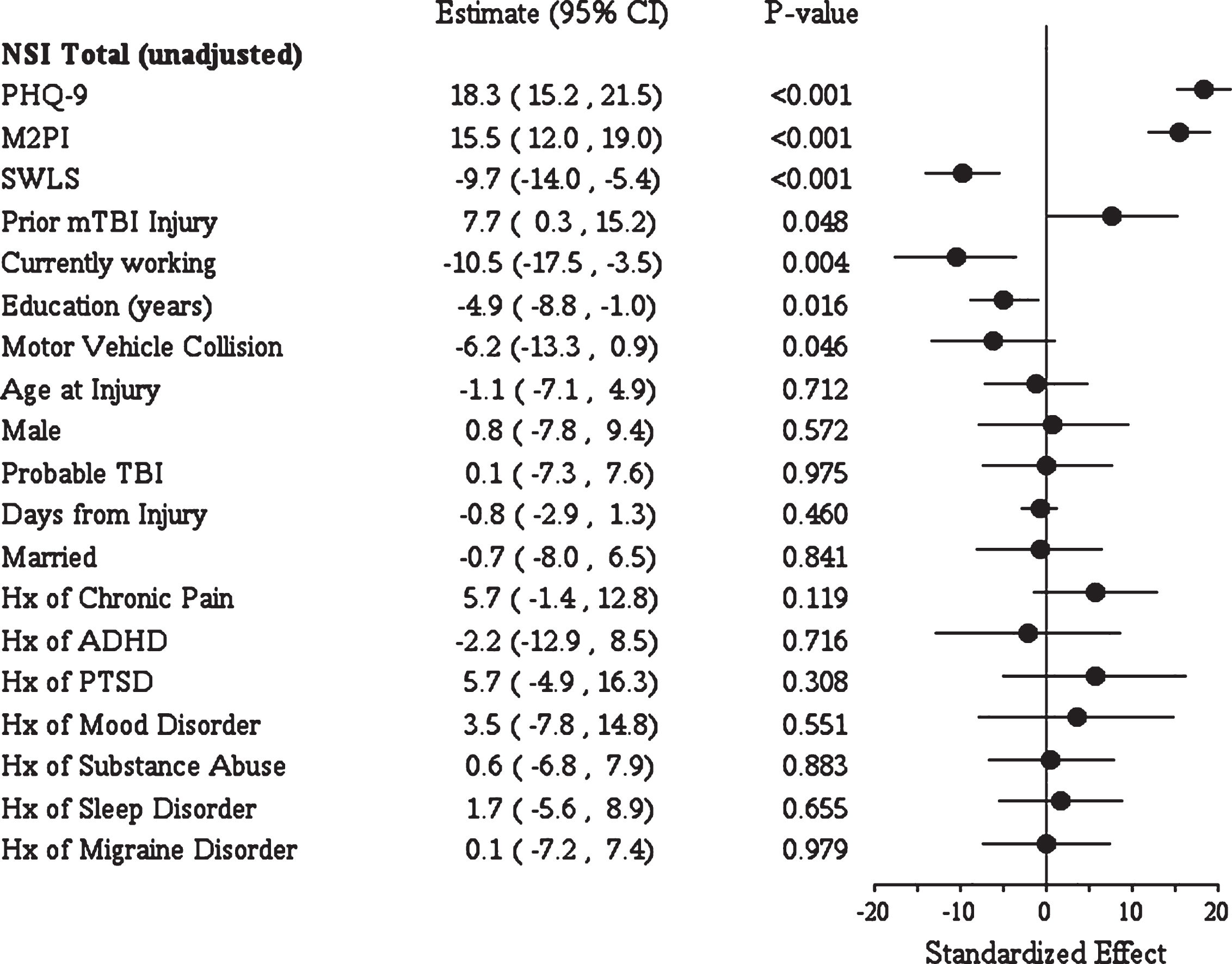
Forest plot depicting univariate analysis of NSI-22 total scores. The following continuous variables were scaled so that the displayed effect represents the expected change in NSI when the predictor changes from its 25th to 75th percentile: PHQ-9 (IQR 8), M2PI (IQR 8.5), SWLS (IQR 9), education (IQR 3), age at injury (IQR 23), days from injury (IQR 342.5).
Statistically significant predictor variables identified by univariate analysis were PHQ-9, M2PI, SWLS, prior TBI, unemployment, education, and MVC, which were then entered into the multivariate regression models. Results of this analysis on NSI-22 total score are shown in Fig. 3. The PHQ-9, M2PI, years of education, and absence of MVC as mechanism of injury remained statistically significant. Table 3 shows the parameter estimates from the linear regression model on NSI-22 total multivariate analysis. Each 1-point increase in PHQ-9 was associated with an expected increase of 1.5 points in the NSI total score (95% CI 1.1, 2.0; p < 0.0001). Each 1-point increase on the M2PI total score was further associated with an expected increase of 0.9 points on the NSI-22 total score (95% CI 0.4, 1.4; p < 0.0005). The absence of MVC as etiology for the injury was associated with an average increase of only 2.6 points total (95% CI 0.6, 4.7) on the NSI-22 total score. Figure 3 reports results of the multivariate analysis of NSI subsets. NSI-22 cognitive scores remained statistically significantly associated with PHQ-9, M2PI, and MVC; NSI-22 vestibular scores remained statistically significantly associated with M2PI; NSI-22 somatosensory scores remained statistically significantly associated with PHQ-9, M2PI, education, and MVC; NSI-22 affective scores remained statistically significantly associated with PHQ-9.
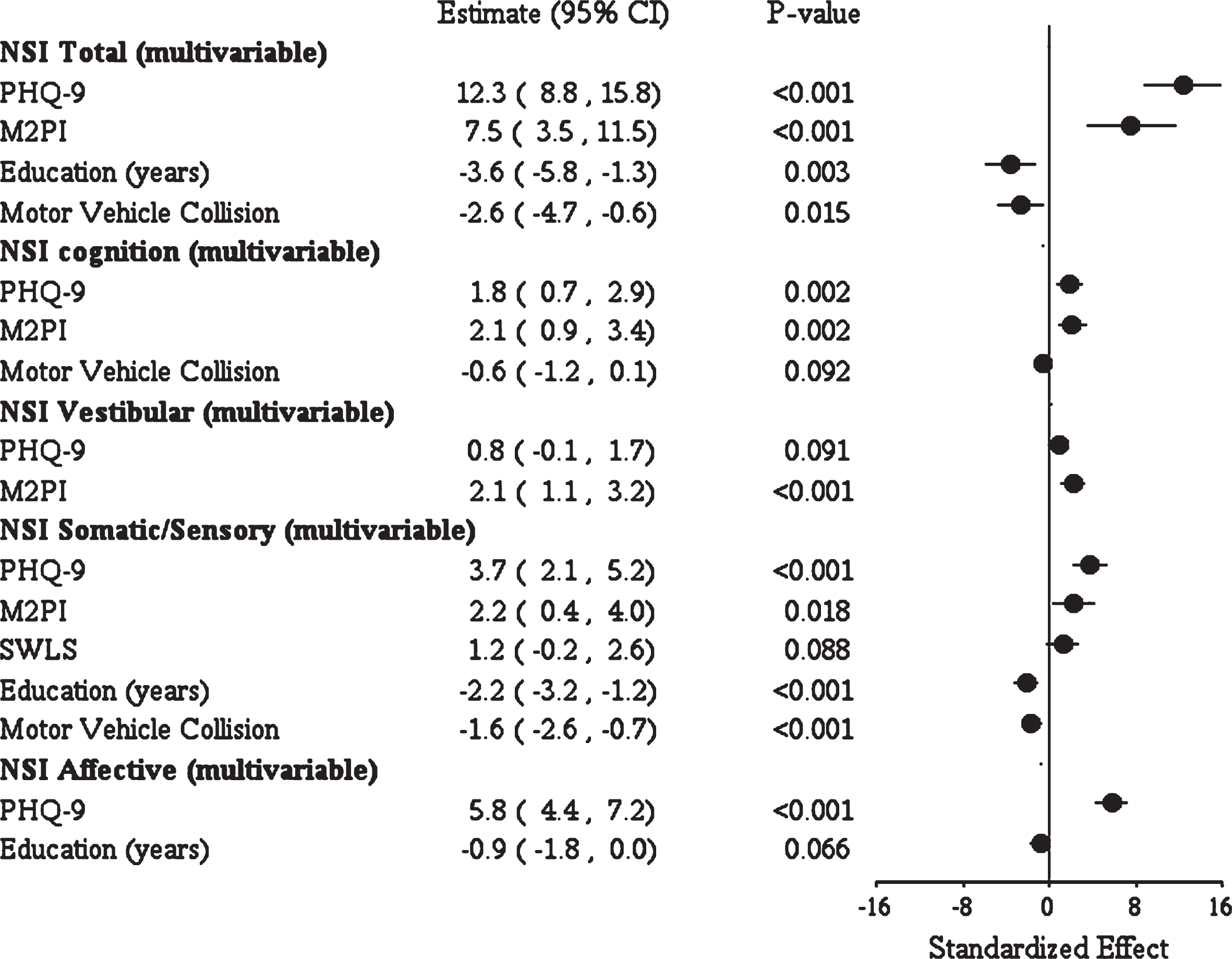
Forest plot depicting multivariable analysis of NSI-22 total and all NSI subsets. The following continuous variables were scaled so that the displayed effect represents the expected change in NSI when the predictor changes from its 25th to 75th percentile: PHQ-9 (IQR 8), M2PI (IQR 8.5), SWLS (IQR 9), education (IQR 3), age at injury (IQR 23), days from injury (IQR 342.5).
Parameter estimates from linear regression model on NSI-22 total multivariable analysis
Abbreviations: PHQ–9 = Patient Health Questionnaire; M2PI = Mayo-Portland Participation Index; MTBI = Mild traumatic brain injury; SWLS = Satisfaction with Life Scale. aFor continuous variables, slope estimate represents the expected change in NSI-22 total score in response to a one unit increase in the independent variable. For example, each 1 point increase in PHQ-9 results in a 1.5 point expected change on NSI-22 total score. For binary variables, the slope estimate represents expected change when condition is present. For example, the absence of MVC represents a total change of 2.65 points on NSI-22 total score. bFor continuous variables, scaled estimate represents expected change in response from the 25th percentile to the 75th percentile of the independent variable. For example, there is an expected change of 12.3 points on the NSI-22 total score when PHQ-9 changes from the 25th to 75th percentile.
In this sample of a community-based, treatment-seeking population with MTBI, psychological and participation factors, more education, and an absence of MVC collision as mechanism of injury, were significantly associated with increased NBS reporting, while injury severity, time since injury, and prior MTBI did not have a statistically significant influence. These findings in a civilian sample are overall consistent with those reported in military populations. Andrews et al. (2018) found that behavioral and psychological factors accounted for 42.5% of the variance in NSI-22 in a sample of veterans, with MTBI showing negligible predictive value. A diagnosis of PTSD was the largest predictor of increased neurobehavioral symptom reporting on NSI-22, with baseline sleep impairment predicting increased symptoms as well. Lange et al. (2014) found that depression and PTSD symptoms accounted for the 41.5% of the variance of NBS reported on the NSI-22 in a U.S. military service member sample, and further associations have been found with NSI-22 reporting and Generalized Anxiety Disorder and Depression in veterans (King et al., 2012).
The strongest predictor of increased NBS in our sample was increased reporting of depressive symptoms on the PHQ-9. There was a strong effect magnitude of NSI-22 total scores with PHQ-9, and the associations remained significant with all NSI-22 subsets, except with the NSI vestibular subset. On multivariate analysis, each 1-point increase in PHQ-9 was associated with an expected increase of 1.5 points in the NSI-22 total score. Furthermore, 58% of the sample reported scores greater than 10 on the PHQ-9 with an average score of 11, indicative of moderately severe depression. While the presence of a prior history of mood disorder did not correlate with increased symptoms in this study, this was likely due to the high prevalence of a history of depression across the entire sample (83%).
These findings of increased depressive symptom reporting associated with increased NBS after MTBI are consistent with prior studies (Kumar et al., 2014; Lange et al., 2011; Powell et al., 2019), demonstrating that NBS reporting is mediated by emotional distress in those with MTBI. Within the spectrum of TBI severity, depressive disorder remains one of the most common conditions after TBI (Kreitzer et al., 2019), and anxiety and depression are both common after MTBI (Delmonico, Theodore, Sandel, Armstrong, & Camicia, 2017; Merz et al., 2019). While the rate of mood disorders is generally very high after TBI, those with MTBI can report depressive symptoms that are equal or even greater to those with more severe injuries (Singh, Mason, Lecky, & Dawson, 2018), with severity of depression associated with increased symptom reporting after MTBI (Terry et al., 2019). In a prior study of a similar cohort of individuals across all severities of TBI, those with MTBI had significantly increased report of depressive symptoms as compared to those with moderate to severe TBI (Powell et al., 2019).
An important consideration is that many of the diagnostic features of depression (difficulty concentrating, fatigue, sleep difficulties) are similar to the symptoms included within the NSI-22 and other definitions of PCS (Lange et al., 2011). Therefore a degree of overlap can be expected. While many studies have shown the association between PCS and other medical conditions, other studies have analyzed the unique variance of PCS. In a study of veterans of conflicts in Afghanistan and Iraq, structural equation modeling was used to show strong relationship between MTBI and development of PCS that was independent of concomitant PTSD or depression (Morissette et al., 2011). In an online questionnaire analyzing the prevalence of PCS symptoms in those with MTBI as compared to a healthy population, the presence of headaches distinguished between MTBI and healthy control groups (Dean, O’Neill, & Sterr, 2012). Headaches and dizziness are clinical features of PCS that overall overlap least among associated psychiatric disorders (Staab & Powell, 2019). In a sample of MTBI individuals in an outpatient specialty clinic, individuals with MTBI and depression reported increased NBS as compared to individuals with MTBI without depression, suggesting that, while there is overlap within the criteria, the presence of depression with MTBI is associated with a particularly high symptom burden (Lange et al., 2011). In our sample, PHQ-9 scores had the highest standardized effect within the NSI affective subset. However PHQ-9 scores remained significantly associated with all NSI-22 subsets. The reason for such high associations between depression and MTBI is likely multifactorial, related not only to shared diagnostic criteria and the high prevalence of depression (Lange et al., 2011), but to other behavioral, personality and psychosocial factors as well (Powell et al., 2019).
Other predictive variables unassociated with the injury, including decreased societal participation and lower years of education at time of program admission, were significantly associated with increased NBS reporting. In a study of military veterans, M2PI correlated significantly with mental health conditions, further showing the potential interplay between scores of NSI-22, PHQ-9, and M2PI (O’Rourke et al., 2019). Multivariable analysis showed that lower years of education were significantly associated with increased NBS reporting as well. A study on athletes with sports related concussion showed that lower years of education resulted in increased neuropsychological symptoms after MTBI (Dougan, Horswill, & Geffen, 2014), however level of education in a similar population cohort as this study has not been found to be a predictor of increased NBS otherwise. A higher level of education has been associated with increased cognitive reserve and hence a decreased vulnerability to cognitive deficits post TBI (Kesler, Adams, Blasey, & Bigler, 2003), and it has been postulated that this, in turn, can offer a protective benefit to development of mood disorders and to increased NBS (Scholten et al., 2016). Lower levels of education have been found to contribute to increased risk of unemployment after MTBI (Cancelliere et al., 2014), which in turn can lead to worsening societal participation and subsequent increased symptom reporting.
In this community-based, treatment-seeking sample, measures of injury severity (Possible vs. Probable TBI), prior MTBI, and time since injury did not have a significant effect on NBS reporting after multivariable analysis. Mechanism of injury was a statistically significant predictor, however the absence of a MVC was associated with an average increase of only 2.6 points on NSI-22 total score. Instead, external factors apart from the physiological impact of the injury –psychological factors as well as decreased societal participation including unemployment – predicted increased NBS reporting as compared to injury-related factors. As a whole, these findings support the literature suggesting that it is unlikely that the physiological components of the injury or the severity of MTBI are the predominant factors contributing to persistent NBS after MTBI, although the injury may be associated with increased symptoms indirectly (Andrews et al., 2018; Lange et al., 2014; Nordhaug et al., 2015). Iverson (2019) identified a model reflecting interrelated persistent NBS, suggesting that various life stressors interact with personality and premorbid mental health factors that result in persistent NBS after MTBI, including pre-injury emotional trauma and baseline personality factors (Ruff, Camenzuli, & Mueller, 1996). Overall, cumulative stressors interacting with premorbid behavioral and mental health problems are the main factors that result in persistent NBS (Iverson, 2005). This is further reflected in the proportion of patients with pre-existing comorbidities that have been shown to prolong and worsen symptoms after MTBI, as shown in Table 2, as well as a high proportion of patients unemployed (59%).
Based on the strength of association of the NSI-22 with PHQ-9 and M2PI, this study supports a multifactorial, interdisciplinary treatment approach to PCS, with a particular focus of targeting psychological and behavioral difficulties and with goals of improving a person’s participation in societal roles. While the effects of interdisciplinary treatment were not studied in this analysis, multidisciplinary treatment including vocational rehabilitation, psychological services, and therapeutic services have been shown to improve depressive symptoms in this sample of individuals (Powell et al., 2019). Psychotherapeutic treatment is likely to have benefit for this subset of individuals. In particular, the role of cognitive behavioral therapy has evidence showing improved outcomes in individuals with MTBI (Al Sayegh, Sandford, & Carson, 2010; Bryant, Moulds, Guthrie, & Nixon, 2003). At this time, no large randomized controlled trials have shown efficacy for pharmacological treatment for individuals with MTBI for overall NBS improvement above placebo, and pharmacological treatment for targeting depressive symptoms after MTBI remains controversial. A study assessing relationship between pharmacological treatment at the time of injury in persons with MTBI found that those receiving pharmacological treatment for depression had significantly fewer clinician visits for persistent symptoms post injury as compared to those who did not receive pharmacological treatment (Kruse, Li, Prideaux, & Brown, 2018). Meta-analysis of pharmacological treatment after TBI of all severity showed no significant improvement in depression after TBI as compared to placebo (Kreitzer et al., 2019). However some have argued that individuals with MTBI are appropriate for trials of antidepressants to improve psychological elements associated with increased NBS (Silverberg & Panenka, 2019). The role of vocational rehabilitation within this treatment program must also be emphasized, given the findings of the study. Improvements in return to work in individuals with persistent symptoms after MTBI have been demonstrated in interdisciplinary clinics (Dornonville de la Cour, Rasmussen, Foged, Jensen, & Schow, 2019).
This study has several limitations. Data was collected prospectively, however the study was retrospective and thus has a higher risk of confounding factors and bias. Data may not have been inclusively compiled during documentation of the initial patient visit in recording all past histories of ADHD, mood disorder, PTSD, sleep disorder, migraine headaches, or substance abuse –thus, some conditions may be underrepresented. In this case, given the high proportion of associated conditions in our sample study, the results do provide meaningful information. The population in the study was primarily from Olmsted County, MN, and surrounding regions, as individuals admitted to the program required an ongoing therapy need and thus consistent follow up. This population is primarily white and of northern European descent with slightly higher median education levels (Melton, 1996). Thus, this patient population may not be generalizable to treatment-seeking populations in other regions of the United States. In particular, racial and ethnic minorities, as well as those from underserved communities (American Indians, Alaskan Natives) were not represented in this sample, and this patient population is even more likely to report depressive symptoms after TBI (Perrin et al., 2014). However, prior studies using the Rochester Epidemiology Project (REP), a comprehensive medical records linkage infrastructure encompassing all persons in Olmsted County, MN, (i.e. in our community), found that the population of our region can be generalizable to a substantial part of the United States (Melton, 1996). This study did not exclude individuals with Validity-10 scores above the cut-off range, and thus may not have accounted for symptom exaggeration; however, this was ultimately a treatment-seeking and not a forensic sample, and Validity-10 scores have not been validated in a community population at this time.
Conclusion
Within a treatment-seeking community sample with persistent symptoms after MTBI, increased endorsement of depressive symptoms and greater self-reported level of disability strongly predicted increased neurobehavioral symptoms. Significant associations were found between a lower education level and unemployment with increased NBS, and the absence of MVC was weakly associated with higher NSI-22 total scores on multivariate analysis. Measures of injury severity did not have any statistically significant effect on NBS reporting. Strongest associations overall were found between reported NSI-22 and increased reported depressive symptoms on PHQ-9. These results further support the need for comprehensive assessment and interdisciplinary treatment that assist with the management of physical, cognitive, behavioral, and emotional symptoms that impact quality of life in persons with MTBI presenting for treatment.
Conflict of interest
The authors have no disclosures.
Funding
The authors received no financial support for the research, authorship, and/or publication of thisarticle.