
Abstract
BACKGROUND:
Robot-assisted gait training (RAGT) allows an intensive gait training in patients with cerebral palsy (CP). There are few evidences on the effectiveness of RAGT in adults with CP.
OBJECTIVE:
To assess the effect of RAGT on gross motor function in adolescent and adult patients with bilateral spastic CP and to compare the effect of RAGT with conventional kinesiotherapy.
METHODS:
Forty-seven patients (mean age 21.2±5.33 years) with bilateral spastic CP were divided into two groups. Twenty-one patients underwent 20 therapeutic units of RAGT and 26 patients underwent 20 therapeutic units of conventional therapy/training (CON). The following parameters were evaluated before (V1) and after the therapy (V2): dimension A (lying and rolling), B (sitting), C (crawling and kneeling), D (standing), E (walking, running and jumping) of the Gross Motor Function Measure (GMFM-88). In patients in the experimental RAGT group, these parameters were also evaluated 3–4 months later (V3).
RESULTS:
Comparing the mean improvements in endpoints in both groups (RAGT vs. CON) after 20 TUs, we observed the statistically significant difference (p < 0.001) and large effect size in all GMFM dimensions and total GMFM improvement in favour of the RAGT group. In RAGT patients, the improvement persisted even 3–4 months after RAGT (p < 0.001).
CONCLUSION:
We demonstrated that the intensive RAGT regimen is more effective than conventional therapy in terms of improvements in gross motor functions in adolescent and adult patients with bilateral spastic CP.
Abbreviations
Cerebral palsy Gross Motor Function Measure International Classification of Functioning, Disability and Health World Health Organization Gross Motor Function Classification System Minimal clinically important difference Robot-assisted gait training Activities of daily living Control group/conventional therapy Therapeutic unit Bilateral spastic cerebral palsy
Introduction
Cerebral palsy (CP) describes a group of permanent disorders of the development of movement and posture, causing activity limitation, that are attributed to non-progressive disturbances that occurred in the developing foetal or infant brain (Rosenbaum, 2007). CP is the most frequent cause of motor, sensory and cognitive disability in childhood. The current prevalence of CP in industrialised countries ranges from 1.5 to 2.5 per 1,000 live births, with one new case every 500 live births (Surman, 2009; Oskoui, 2013). The therapy of patients with CP is a continuous lifelong process. A multidisciplinary therapeutic approach in the care of patients with CP is crucial (Heine, 2009). Early initiation of the rehabilitation is very important; its basic element is a therapeutic physical education. Therapy is not intended to cure or achieve a normal state. The real goal is to improve the functionality and skills and maintain health in terms of locomotor, cognitive development, social integration, and independence. Increased emphasis is now being placed on an active approach in the therapy, including intensive, repetitive, and task-specific training to enhance neuroplasticity (Das, Ganesh, 2019). In the last decade, there has been a noticeable increase in the use of robot-assisted rehabilitation, particularly in patients after stroke, cerebrospinal trauma and, last but not least, in children with cerebral palsy. The neurophysiological background of RAGT is based on the spinal automatism (central pattern generators), plasticity of the central nervous system, and motor learning (Barbeau, 2013, Wiart, 2016). Despite inconsistent conclusions, several authors demonstrated the effectiveness of the robot-assisted locomotor therapy on gait improvement in adult patients after stroke and cerebral and spinal trauma (Mehrholz, 2017; Mekki, 2018; Shackleton, 2019). In addition to the improvement of locomotor functions, positive effects of training on postural adaptation, cardiovascular function, muscle metabolism, intestinal motility, tissue trophicity, and overall improvement in quality of life are apparent (Riener, 2006; Shackleton, 2019). Published studies have shown the beneficial effect of RAGT in patients with other neurological diseases, e.g. Parkinson’s disease (Furnani, 2017), multiple sclerosis (Russo, 2018; Straudi, 2013).
Since 2005, RAGT has also been used in paediatric patients with impaired motor functions of various aetiology, most commonly in children with CP. Recent systematic reviews and meta-analyses evaluating the effectiveness of RAGT in children and adolescents with CP have documented the effectiveness of robot-assisted training primarily in standing ability, balance control in gait, walking speed and distance, walking endurance, and improving gross motor functions (Carvalho et al., 2017; Bayon, 2016; Lefmann, 2017; Wallard, 2017; Booth, 2019).
To date, few studies have studied the effect of RAGT on motor functions in adolescent and adult patients with CP. The results of studies evaluating the effect of gait training in adolescent and adult patients with CP have shown its positive effect on motor functions and gait parameters (Patritti, 2010; Chrysagis, 2012; On-Yoo Kim et al., 2015). There is currently no formalised pathway for the transition from paediatric to adult healthcare in patients with CP (Orlin, 2014) and, furthermore, there is no consensus on which physiotherapeutic interventions most effectively help to improve or maintain functional mobility in patients with CP. The effort is rather to maintain than improve gross motor functions in adolescent and adult patients with CP, especially in the more severely affected patients (Schroeder, 2014).
Most published studies have focused on effects of resistance training and strengthening in these patients. Insufficient awareness of interventions for adults with CP can lead to the reduced quality of provided healthcare and, subsequently, to the lower quality of life (Lawrence, 2016). A systematic review published in 2010 revealed that only a few studies on physiotherapeutic interventions in adult patients with CP have been conducted, and even fewer have been conducted with good methodological quality (Jeglinsky, 2010). In their systematic review, Lawrence et al. (2016) evaluated the available evidence for PT interventions to address functional mobility limitations such as ambulation, stair negotiation and dynamic postural stability in ambulatory adults with CP aged older than 18 years. The review showed that the evidence of the effect of exercise on functional mobility for ambulatory adults with CP is lacking. Rhythmic auditory stimulation and interactive serious gaming were found to be statistically significant in benefiting adults with CP.
RAGT is a promising tool that allows prolonged, controlled, intensive, task-specific training that is goal-directed and cognitively engaging with the high repetition of steps. These aspects promote a reproducible and kinematically consistent, symmetric, physiological-like movement of limbs (gait pattern) able to enhance motor learning and neuroplasticity.
The objective of the presented randomized clinical trial was to evaluate the effect of RAGT on motor functions in adolescent and adult patients with bilateral spastic CP, compared to the conventional kinesiotherapy, and to assess the persistence of RAGT effect on their motor functions during 3–4 months.
Materials and methods
Experimental design
The study was conducted as a prospective, bicentric, comparative, randomized clinical trial in two out-patient rehabilitation healthcare facilities in Slovakia from September 2009 to August 2018. Of 101 patients examined, 47 adolescent and adult patients with bilateral spastic CP were enrolled into the study (Fig. 1, Table 1). The randomization to both groups was stratified based on the study site and type of therapy. The first group (RAGT) consisted of 21 patients of the rehabilitation centre which offers the possibility of robot-assisted gait training; these patients underwent 20 therapeutic units (TUs) of RAGT. 26 patients in the second group (CON) underwent 20 TUs of conventional kinesiotherapy in another rehabilitation centre in which a RAGT device was not available. Figure 1 shows the patient flow through the recruitment, assessment, intervention and follow-up.
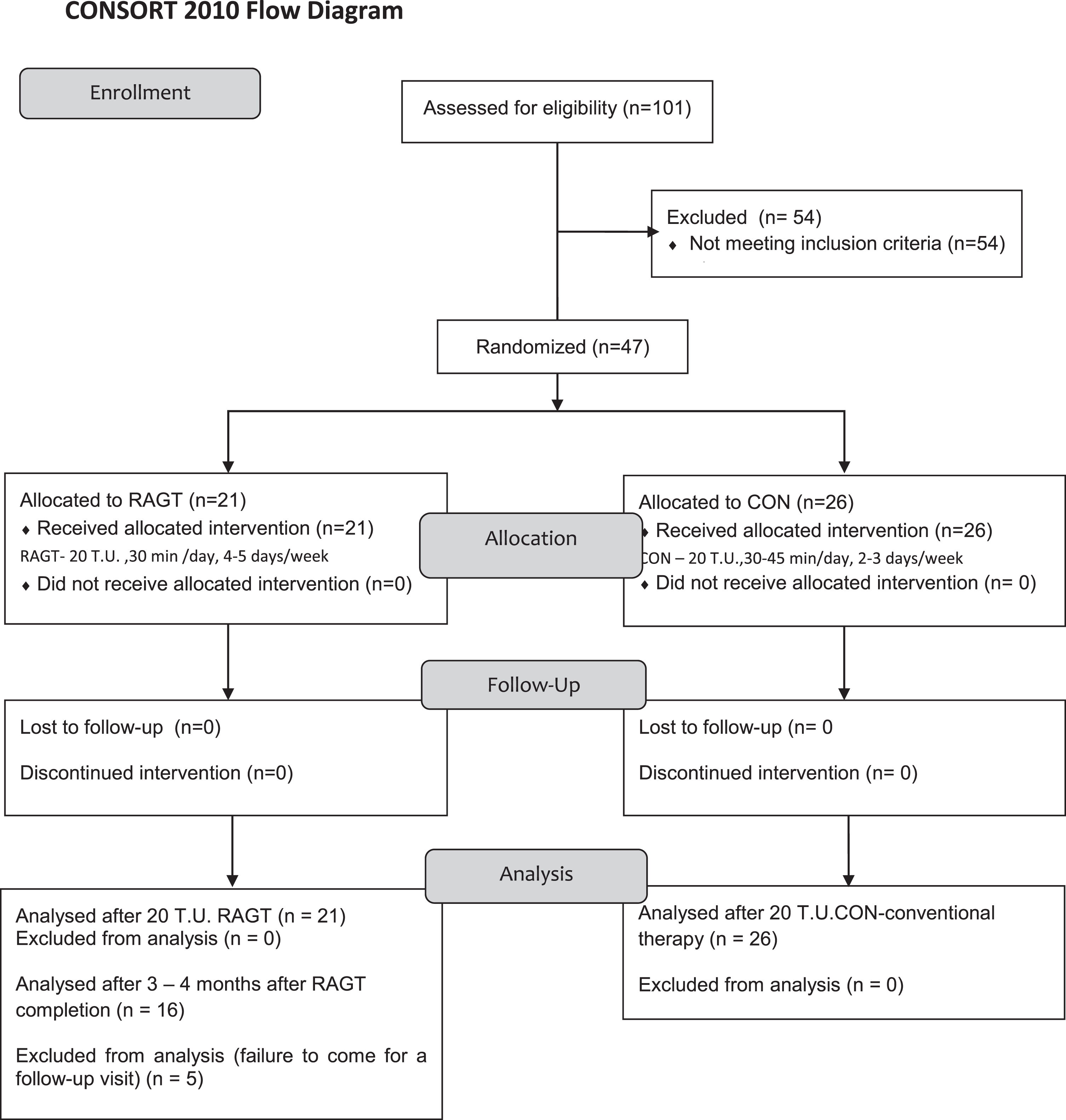
Flowchart of participants’ enrollment and randomization.
Demographical and clinical features of the two groups of patients
There were no significant differences between the two groups in terms of age, gender and severity of motor impairment, although the control group was older (mean 23.4 years vs. 18.3 years) and included more severely affected patients (mean GMFCS level was 3.14 (±0.85) and 3.25 (±0.71) in the RAGT and CON group, respectively).
All patients, parents or legal representatives of patients were informed about the course and conditions related to the applied therapy, as well as about the use of test results for research purpose, and they gave the informed consent before inclusion. This study was conducted in accordance with the principles of the Declaration of Helsinki and Good Clinical Practice (GCP) and was approved by the local ethics committee.
Therapy device
The robot-assisted gait training was performed using the Lokomat® system (Hocoma Inc., Volket-swil, Switzerland). Lokomat® consists of a treadmill, special proprietary suspension system, and electronically controlled lower limb orthoses. The electromechanical body weight supports the system monitors and adjusts the body weight support in real time at the requested level. Moveable parts are controlled by three computers and a special software. Computer-controlled controls at each hip and knee joint are synchronised with the speed of the treadmill. The force sensors on these joints are connected in order to record the interaction between the patient and the Lokomat® system. Since the parameters of each training (distance, speed, number of steps, rate of body weight support and guidance force) are well defined and continuously monitored, gait training can easily be compared inter-individually as well as between individual therapeutic units. This offers opportunities not only for research but also for specific therapeutic plans and patient management.
The pelvic fixation using orthoses and adjustable pelvic support is an important element of the therapy. A dorsal flexion of the talocrural joint is achieved using a passive foot lifter. On monitors dedicated to the patient and therapist, we can visually monitor in real time and consequently influence the course of the exercise. To increase the participation during RAGT training, a special virtual reality-based environment (VR) has been developed. The software is also equipped with Guidance Force function by which the therapist can adjust the rate of guidance of the patient’s lower limbs by the Lokomat system. The value of 100% represents a strict guidance (position control with fixed joints of the Lokomat system). The value of 0% represents an idle speed (freely moveable joints of the Lokomat system). The unrestricted gait can be achieved with the guidance force value lower than ca. 20%. The robot-assisted gait training has been considered to be a safe therapeutic option in the paediatric neurorehabilitation (Meyer –Heim, 2007; Borggraefe, 2010b; Aurich-Schuler, 2015).
Therapeutic interventions
We started with 100% body weight support and then reduced it as much as possible up to the point when the knee maintained the extension posture during stance phase and was then gradually decreased according to the individual’s response to the intervention and to his/her functional capacity. The guidance force was individually adjusted according to the clinical judgement and the patient’s abilities in order to maximise the intensity of the training and to maintain the motivation during each session. The therapist provided verbal enhancement to step actively and to raise patients’ awareness to correct gait patterns and posture during the therapeutic unit. Active patient participation was additionally achieved by changing the walking speed, body weight support or guidance force of the exoskeleton. Patients were trained in the virtual reality-based environment.
Prior to the robot-assisted locomotor therapy, patients from the experimental group 1 (RAGT) underwent a conventional rehabilitation (most commonly Vojta’s method of reflex locomotion, neurodevelopmental treatment NDT –Bobath concept, ergotherapy, physical therapy –magnet therapy, bio laser phototherapy, and some patients underwent complementary methods of therapeutic rehabilitation –synergetic reflex therapy, ball training, circular training, TheraSuit, hydrotherapy, acupuncture, etc.) in various combinations and at different frequencies depending on the type and options of the healthcare facility they have been attending.
Both RAGT and CON were delivered by trained physical therapists specialised in the management of patients with cerebral palsy. Assessments in both groups were performed independently by a different group of physical therapists.
Evaluations
All evaluations were performed within 24 hours prior to the therapy and within 24 hours after the last therapeutic unit. In the experimental group 1 (RAGT), patients were also tested 3–4 months after the RAGT completion. Prior to therapy, patients were routinely examined by a rehabilitation doctor in the out-patient setting. All patients were classified at the admittance according to the Gross Motor Function Classification System (GMFCS). The GMFCS is a 5-level classification system that describes the gross motor functions in children and youth (young adults) on the basis of their self-initiated movement, with a particular emphasis on sitting, walking and wheeled mobility (Palisano, 1997). Distinctions between levels are based on functional abilities, the need for assistive technology, including hand-held mobility devices or wheeled mobility, and to a much lesser extent, quality of movement.
Subsequently, patients were tested using the Gross Motor Function Measure (GMFM). GMFM is a standardised examination procedure for children older than 5 months. It evaluates the changes in the gross motor functions over time in patients with CP. There are two versions of the GMFM; the 88-item version (GMFM-88) and the abbreviated 66-item version (GMFM-66). To evaluate patients’ motor functions in this study, we used the more detailed 88-item version which evaluates patient’s motor functions in the following five dimensions:
Walking time (min), walking distance during one therapeutic unit and total walking distance (m), and average walking speed (km/h) during each training was evaluated by the Lokomat® system.
Statistical analysis
To process the obtained data, we used descriptive statistics, non-parametric statistics and effect size. We processed data using MS Office Excel and SPSS 21.0 for Windows. Data are presented as means plus minus standard deviations or medians and interquartile ranges (IQR). The two groups were compared at the baseline using χ2 test/Fisher’s exact test for categorical variables and independent sample t-test (2-tailed, significance level p < 0.05) for continuous variables. The normality of our data sets was tested using Kolmogorov-Smirnov normality test. Since the normal data distribution was not maintained across all data sets, the non-parametric Wilcoxon test for paired values was used to compare the input and output GMFM values in each group. To evaluate inter-group differences of the percentage improvement in GMFM (RAGT vs. CON), we used the Mann-Whitney test of two independent data sets. The results are considered statistically significant with p < 0.05 and highly statistically significant with p < 0.001. To determine the substantive significance of the differences, we used the calculation of the Cohen’s effect size (d) using the pooled standard deviation. According to the concept of Cohen (1977) and Sawilowski (2009), the coefficient d = 0.01 –0.2 was interpreted as a very small effect size, d = 0.2 –0.5 as a small effect size, and d = 0.5 –0.8 as a medium-sized effect causing the difference. The values d = 0.8 –1.2 represent a large effect size and d > 1.2 a very large effect size. The calculation of mean improvements and the Cohen’s coefficient d were completed by calculating 95% confidence interval (CI 95%).
Results
Forty-seven patients (27 males and 20 females) with bilateral spastic CP aged 15.1 –35.1 years (mean age 21.2 (SD±5.33)) underwent 20 TUs according to the scheduled protocol. The severity of disability was determined using GMFCS (Gross Motor Function Classification Scale) (Palisano, 1997). Patients with GMFCS level I, II (n = 8) were evaluated as mildly affected. Patients with GMFCS level III, IV were evaluated as more severely affected (n = 39). Baseline data of all the recruited patients are summarized in Table 1.
Evaluation of improvement in motor functions in the experimental RAGT group
Twenty-one patients with bilateral spastic CP underwent 20 therapeutic units of the robot-assisted locomotor therapy using the Lokomat® system during four to six weeks, three to five times a week. The intervention was well tolerated with no adverse events, except for minor issues such as small leg abrasions.
The following values are presented as mean±SD (min–max). The mean duration of one therapeutic unit (TU) was 28.81 min per patient (SD±3.09, ranging from 20.59 to 35.91) and the mean distance that patients walked during one therapeutic unit was 713.54 m (SD±122.32, ranging from 475 to 889). The mean total distance per patient during the therapy consisting of 20 TUs was 14,797 m (SD±2,563.75, ranging from 9,027 to 18, 605) and the mean total time per patient was 607.53 min (SD±86.03, ranging from 452.54 to 820.46). The average speed was 1.59 km/h (SD±0.17, ranging from 1.2 to 1.8).
After 20 therapeutic units in the RAGT group, the evaluated input parameters have improved as follows (Table 2, Fig. 2).
RAGT group (n = 21) –improvement in motor functions assessed by the GMFM-88 after 20 therapeutic units of robot–assisted gait training (RAGT)
RAGT group (n = 21) –improvement in motor functions assessed by the GMFM-88 after 20 therapeutic units of robot–assisted gait training (RAGT)
Values are presented as mean±SD. V1 –visit 1 (baseline), V2 –visit 2 (post- intervention), GMFM –Gross Motor Function Measure. d –Cohen’s effect size, rate of substantive significance of differences. d = 0.2 –0.5 (small difference), d = 0.50 –0.80 (medium-sized difference), d = 0.80 –1.2 (large difference). p –statistical significance level, significant at p < 0.05. Z –value of the test criterion (statistical calculation) was obtained using the Wilcoxon test. A statistically significant improvement in motor functions represented the small Cohen’s effect size (d) in dimensions B, C, D, E, GMFM total score, and the medium-sized Cohen’s d effect size in GMFM dimension A.
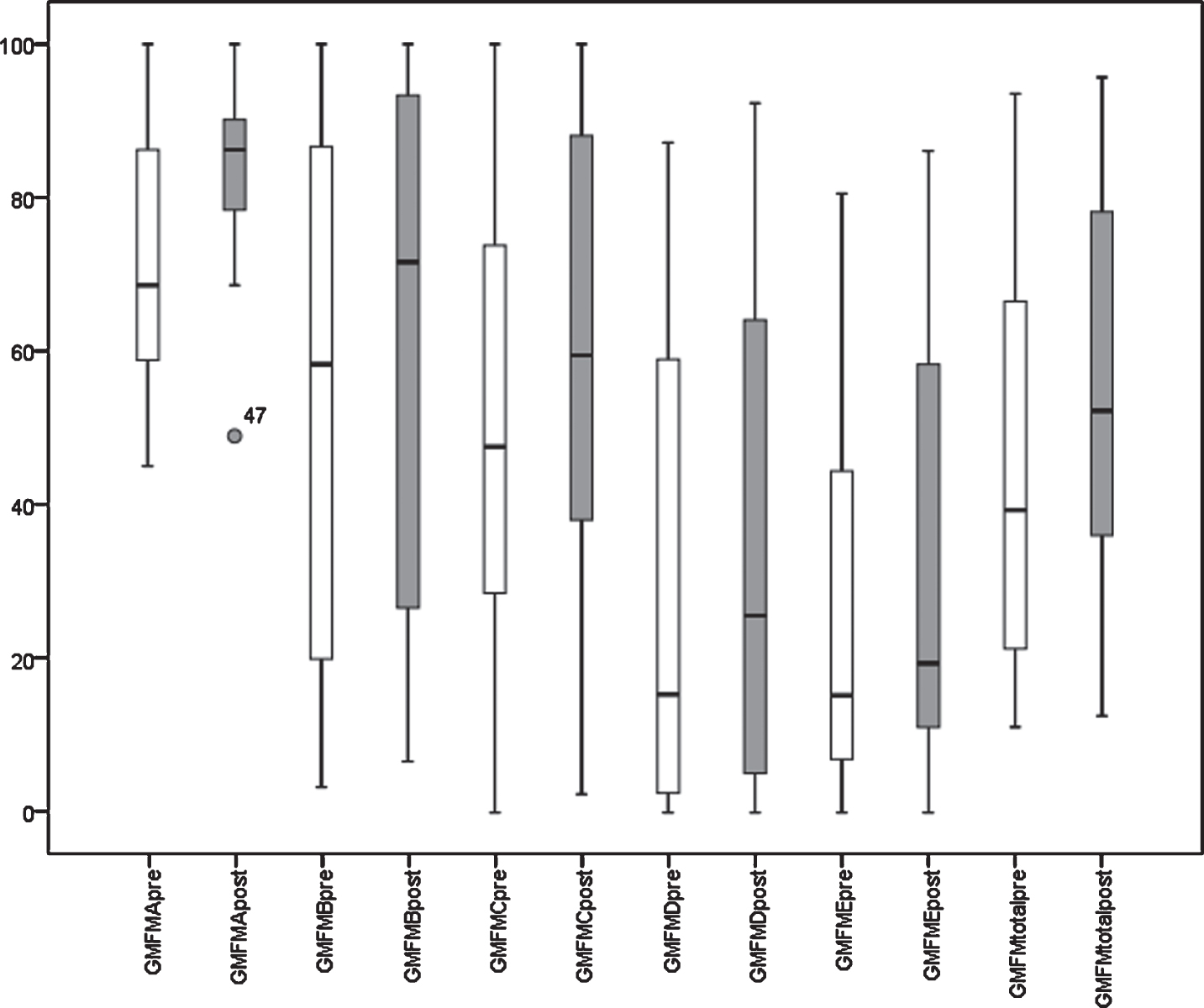
RAGT group (n = 21) –improvement (p < 0.001) in motor functions assessed by the GMFM-88 after 20 therapeutic units of robot-assisted gait training (RAGT). The box plot shows the minimum, maximum, first and third quartile-interquartile ranges (IQR median [5th; 95th percentiles]); the median is indicated between quartiles inside the box and the outliers are marked with a circle. GMFM –Gross Motor Function Measure.
Twenty-six patients from group 2 (control group, CON) underwent 20 therapeutic units of individual kinesiotherapy 2–3x a week under the supervision of a physical therapist. One therapeutic unit lasted for 30–45 minutes.
The following values are presented as mean±SD (min–max). After 20 therapeutic units of the conventional kinesiotherapy in CON group, we observed the following changes in endpoints:
A statistically non-significant change in the evaluation of motor functions in patients after 20 TUs of the conventional kinesiotherapy represented a very small effect size in the evaluated GMFM parameters (Table 3, Fig. 3).
CON group (n = 26) –change in motor functions assessed by the GMFM-88 after 20 therapeutic units of the conventional kinesiotherapy (CON)
CON group (n = 26) –change in motor functions assessed by the GMFM-88 after 20 therapeutic units of the conventional kinesiotherapy (CON)
Values are presented as mean±SD. V1 - visit 1 (baseline), V2 - visit 2 (post- intervention), GMFM - Gross Motor Function Measure. d –Cohen’s effect size, rate of substantive significance of differences. d = 0.2 –0.5 (small difference), d = 0.50 –0.80 (medium-sized difference), d = 0.80 –1.2 (large difference). p –statistical significance level, significant at p < 0.05. Z –value of the test criterion (statistical calculation) was obtained using the Wilcoxon test.
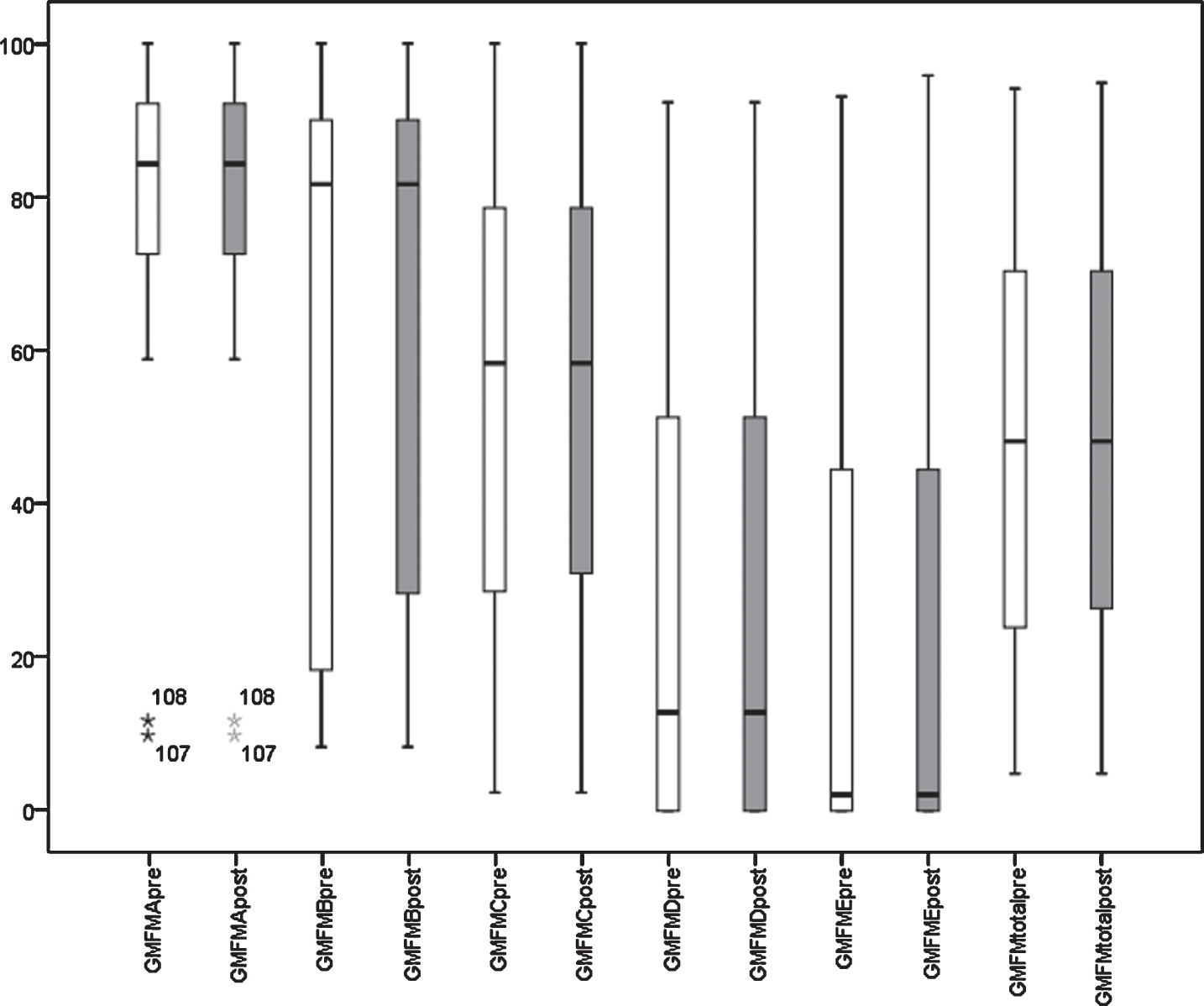
CON group (n = 26) –change in motor functions assessed by the GMFM-88 after 20 therapeutic units of the conventional kinesiotherapy (CON). The box plot shows the minimum, maximum, first and third quartile-interquartile ranges (IQR median [5th; 95th percentiles]); the median is indicated between quartiles inside the box and the outliers are marked with a circle. GMFM –Gross Motor Function Measure.
Comparing the mean improvements (%) of endpoints after 20 TUs in both groups (RAGT vs. CON), we documented a statistically significant difference (at a level of statistical significance p = 0.000) in all dimensions A–E as well as in overall GMFM improvement in favour of the RAGT group (Table 4).
Comparison of the change in motor functions in dimensions A-E and overall improvement in GMFM-88 score between the RAGT and CON groups after 20 therapeutic units
Comparison of the change in motor functions in dimensions A-E and overall improvement in GMFM-88 score between the RAGT and CON groups after 20 therapeutic units
Values are presented as mean±SD. GMFM –Gross Motor Function Measure. d = 0.2 –0.5 (small difference), d = 0.50 –0.80 (medium-sized difference), d = 0.80 –1.2 (large difference), d > 1.2 (very large difference). p –statistical significance level, significant at p < 0.05. Z –value of the test criterion (statistical calculation) was obtained using the Mann-Whitney U test. CI 95% –confidence interval.
By calculating the Cohen’s effect size (d), we found that the statistical significance is accompanied by a substantive significance in all dimensions, and it represented a very large effect size in dimensions A, B, C, E and GMFM total score and a large effect size in GMFM dimension D (Table 4).
Twenty-one patients underwent the robot-assisted gait training (RAGT group). Five patients from the experimental RAGT group did not come to a scheduled follow-up visit 3–4 months after RAGT completion. Therefore, we evaluated the maintenance of the therapeutic effect in 16 patients (RAGT subgroup 1). After RAGT completion these patients have continued with the conventional kinesiotherapy, 1–3x a week. They received their regular home-based therapy program (physical therapy or neuro-developmental therapies once or twice per week) as had been established for each patient individually prior to the study period.
Based on the comparison of mean GMFM values before and 3–4 months after RAGT therapy, we can conclude that in the experimental group 1 (RAGT subgroup 1, n = 16) there was no worsening after the completion of therapy with the Lokomat system. A statistically significant improvement persisted (Table 5). By calculating the Cohen’s effect size (d, V1 –V3), we demonstrated that the statistical significance is accompanied by a substantive significance in the dimension A (Z = –3.229, p = 0.001, d = 0.96) which represents the large effect size (Table 5). In dimensions B, C, D, E and GMFM total score, the effect size was small.
Data of the outcome measures immediately before (V1-baseline) and after intervention RAGT (V2), and after the follow-up period (V3) of 3–4 months
Data of the outcome measures immediately before (V1-baseline) and after intervention RAGT (V2), and after the follow-up period (V3) of 3–4 months
Values are means (±SD), Mean Difference (95% CI). V1 –visit 1, examination before RAGT therapy, V2 –visit 2, examination after 20 TUs of RAGT, V3 –visit 3, examination performed 3–4 months after the completion of RAGT therapy. d –Cohen’s effect size, rate of substantive significance of differences. †d = 0.2 –0.5 (small difference), ††d = 0.50 –0.80 (medium-sized difference), †††d = 0.80 –1.2 (large difference). p –statistical significance level, significant at p < 0.05. Z –value of the statistical calculation was obtained using the Wilcoxon test. CI 95% –confidence interval.
Effect of age on gross motor functions in patients with CP
Age should be taken into account as a relevant variable when determining therapeutic goals in patients with CP. Hanna et al. (2008, 2009) and Rosenbaum (2002) processed reference curves of the motor development in individuals with CP based on the longitudinal observation in various age categories and different degrees of disability. They evaluated motor functions using the GMFM-66 test. According to these curves, there is an improvement of gross motor functions in individuals with CP GMFCS level I up to adolescent age, and GMFCS level II up to the age of 9–12 years. The gross motor functions are then constant and usually deteriorate at different ages depending on the severity of the disability. Hanna et al. (2009) stated that the motor functions deteriorate very early in GMFCS levels III –V: at the age of 7 years and 11 months and 6 years and 11 months in GMFCS level III and GMFCS level IV –V, respectively.
In a prospective, controlled cohort study focusing on the effect of robot-enhanced repetitive treadmill therapy on the gross motor function, activity and participation in patients with bilateral spastic cerebral palsy (BS-CP), Schroeder et al. (2014a, b) observed a negative correlation between GMFM-66 score improvement and age. Schroeder et al. (2014) observed more than a two-fold improvement of gross motor functions in GMFM score in younger patients compared to older patients. The group of older children was of adolescent age, so a natural motor development was not expected. Nevertheless, the improvement in their GMFM-66 score still represented a large effect size in minimal clinically important difference (MCID) change (Schroeder, 2014). This supports the hypothesis that RAGT provides benefits even after reaching the maximum predicted motor development in patients with CP (Borggraefe et al., 2010, c).
In our previous work, we have also discussed the influence of age on improving motor functions (Klobucká, 2014). After 20 TUs of RAGT, we documented a statistically significant improvement in motor functions evaluated using GMFM-88 in children, adolescent and young adult patients with CP (GMFCS I –IV). In the group of less severely affected patients (GMFCS I, II), we observed a trend towards higher improvement in younger patients (up to 11 years old). However, in the group of more severely affected patients (GMFCS III, IV), a trend towards higher improvement was observed in patients older than 11 years (Klobucká, 2014).
Adult patients with CP often experience the functional deterioration and loss of physical activity which can lead to the limitation of locomotor functions (Beckung, 2007; Roebroeck, 2009). However, the intensive training can help to prevent the age-related process of de-condition (Damiano, 2006). It can be assumed that the activity-induced neuronal plasticity plays a role in the functional recovery also in adult patients with CP (Winchester, 2005).
Although CP is a lifelong condition, the majority of research has been focused on children and little attention is paid to patients with CP who are 18 + years old (Peterson, 2013).
The objective of this study was to assess the effect of RAGT on motor functions in adolescents and adults with bilateral spastic CP compared to the conventional kinesiotherapy. Patients older than 15 years were enrolled into this study. This criterion was chosen with regard to the biomechanical effect of growth acceleration in puberty, taking into account the expected maximum motor functions in children with CP.
Comparison of RAGT vs. conventional therapy effect on motor functions in patients with CP
After 20 TUs of RAGT using the Lokomat® system in this study we observed more significant improvement in endpoints –GMFM A, B, C, D, E and GMFM total score –in the experimental group vs. the group of patients receiving conventional training in all the mentioned dimensions (p < 0.001). We confirmed this improvement in agreement with other authors in our previous study, where we also confirmed an increase in walking speed and endurance after RAGT (Klobucka, 2013, Meyer-Heim et al. 2007, 2009; Borggraefe et al., 2010a; Patritti et al., 2009).
In several published studies in children and adolescents with CP, the gait training on a treadmill was compared with the conventional physical therapy/kinesiotherapy (Johnson, 2011; Chrysagis, 2012; Schroeder et al. 2014). Unfortunately, these studies show inconsistent/inconclusive findings and results during their interpretation. Schroeder et al. (2014) as well as Chrysagis et al. (2012) found treadmill therapy to be superior in improvements of GMFM dimensions D and E compared to the same amount of conventional therapy (3 trainings per week for 12 weeks). Johnson et al. (2011) showed that only the “supported speed treadmill training exercise program” (SSTTEP) group maintained achieved improvement in spatiotemporal gait parameters and improvement in gross motor functions over the next 12 weeks. Compared to the strength training, there were no statistically significant differences between groups. In their randomized controlled trial Smania et al. (2011) showed a positive and superior effect of the robot-assisted gait training in spatiotemporal gait parameters compared to the conventional physical therapy. However, Druzbicky et al. (2013) did not confirm such superiority in their RCT. In their systematic review and meta-analysis, Booth et al. (2018) showed that the gait training results in a greater positive effect than the standard physical therapy. There is strong evidence that functional gait training results in clinically important benefits for children and young adults with CP, with a therapeutic goal of improved walking speed. Furthermore, there is weak yet relatively consistent evidence that the gait training can also have positive effects on walking endurance and gait-related gross motor function.
In our controlled, prospective trial evaluating the effect of RAGT vs. conventional physical therapy, we observed a significant improvement in motor functions, evaluated using all five GMFM-88 dimensions in adolescent and adult patients with CP. By comparing the mean improvements in the evaluated parameters of gross motor functions (GMFM-88) after 20 therapeutic units in two treatment groups, we observed a significantly greater improvement in the experimental RAGT group compared to the control CON group consisting of patients who underwent the conventional training.
The difference in outcomes achieved in the two groups of our study (RAGT vs. CON) may be caused, to some extent, by different intensity of therapy. Patients from group 1 (RAGT) received the therapy 3–5x a week and patients from group 2 (CON) 2–3x a week, i. e. usual frequency in the clinical practice.
The question of optimal intensity of the therapy in patients with CP is still open and it is different in various studies. If the therapeutic goal is to improve gross motor functions, increasing the frequency of physical therapy/kinesiotherapy may be beneficial. Most patients with CP undergo rehabilitation 1–2x a week, but the frequency of therapy varies from less than 2x a month to more than 3x a week (Palisano, 2012). Given the time and effort that patients with CP and their families invest in motor skills training and prevention of secondary complications, it is important to know whether more frequent rehabilitation really represents a success factor in achieving improved motor functions (Novak, 2012). In most studies, the intensive rehabilitation regimen (with a frequency of 3–11x per week) with a therapeutic unit duration of 30 –60 min leads to a significant improvement in the endpoints (Størvold, 2018; Park, 2018).
In addition, the severity of disability (GMFCS level) can be another determining factor. Schroeder et al. (2014) confirmed a negative correlation of improvement in motor functions (GMFM 66 total score) with increasing GMFCS level. In our presented study, the mean GMFCS was 3.14 (±0.85) and 3.25 (±0.71) in group 1 (RAGT) and group 2 (CON), respectively, with a higher mean age in group 2 (CON); however, the inter-group differences were not statistically significant. Another explanation for the differences in improvement may be the fact that the patients in our study underwent RAGT for the first time, which may be a decisive factor for a statistically significant improvement compared to the CON group in this age category. Schroeder et al. (2014) pointed to the “ceiling-effect” for the improvement in motor functions in particular patients when performing repeated series of the robot-assisted gait training. They found a significant negative correlation between GMFM 66 score improvement and the number of robot-assisted treadmill training blocks in their examined population.
Evaluation of persistence of achieved therapeutic effect
Published studies focusing on the persistence of achieved improvement after the robot-assisted gait training in patients with CP suggest that the achieved therapeutic effect can be maintained for 2–6 months (Borggraefe, 2010c; Meyer –Heim, 2007; Patritti, 2011; Montinaro, 2011; Schroeder, 2014).
In our study, 16 patients from the experimental RAGT group (n = 21) came to the follow-up visit after 3–4 months. Immediately after the completion of RAGT, patients from the experimental group continued with the conventional kinesiotherapy at the frequency of 1–3x a week until the next planned follow-up visit. In these 16 patients (RAGT subgroup), we evaluated the persistence of RAGT effect using GMFM. We observed the statistically significant persistence of achieved improvement in endpoints GMFM A, B, C, D, E and GMFM total score, compared to the values before RAGT.
Improvements in outcomes measured in the study presented by us and their persistence were consistent with unpublished references from patients, parents and caregivers, who mostly experienced greater stamina, endurance, improvement in the ability to climb stairs, and overall mobility improvement in the observed population of CP patients after the therapy with the Lokomat® system when performing daily activities in various positions (sitting, standing, lying). They also recorded improvements in transfers, either with the help of crutches, walkers, assistance by another person, or by other means. These references are also supported by the results of the study performed by Schroeder et al. (2014), who reported improvements in occupation and performance after RAGT using an individualised outcome measure with the Canadian Occupational Performance Measure (COPM).
The minimal clinically important difference (MCID) and effect size
The use of MCID becomes an important part of rehabilitation research since the statistical significance does not yet mean clinical significance and clinical significance does not necessarily mean statistically significant change. The MCID is the smallest change that an instrument can detect, making it possible to interpret whether this observed change results in improvement or worsening of the individual’s symptoms. It is debatable how much the change in GMFM-88 score is clinically significant.
Wang and Yang (2006) divided the improvement in motor functions in patients with CP into three categories: “no improvement”, “moderate improvement” (achieved partial progress in motor functions), “high improvement” (achieved or almost achieved expected improvement in motor functions). In their study related to the sensitivity of GMFM-88, Wang and Yang (2006) stated that an improvement of ≥1.29% in GMFM-88 can be considered clinically detectable, and a score increase by ≥3.99% is considered as a major improvement.
Oeffinger et al. (2008) calculated MCID for GMFM-66 score in the longitudinal prospective study including 381 walking children with CP aged 4–18 years (the mean age 11 years). For this population, GMFM-66 improvements by ≥1.3 points, GMFM-D score improvements by ≥1.8 points, and GMFM-E score improvements by ≥2.6 points represent a large effect size of clinically important differences.
By calculating Cohen’s effect size when comparing therapeutic interventions between two groups, in the study group of adolescent and adult patients with CP we observed the improvement in favour of the experimental RAGT group (the mean improvement±SD in total GMFM 9.32±9.33), which represents a very large effect size (d = 2.147, 95% CI 1.426 to 2.867) representing a clinically significant difference in the improvement of gross motor functions assessed by the GMFM. This finding is also supported in a review by Moreau et al. (2016) specifically investigating gait speed, reporting that gait training resulted in a large effect size of 0.92 (95% CI 0.19 –1.66), significantly greater than that of strength training (effect size 0.06, 95% CI 0.12 –0.25). Moreover, Carvalho (2017) and Booth (2018) demonstrated similar results. In these studies, endpoints included mainly dimension D, E, walking speed and endurance.
Limitations
It should be noted that our study is limited by several factors. During the study we tried to perform tests by the same physical therapists but, for organisational reasons, this was not possible in all cases. The patient group was heterogeneous in terms of severity of disability. On the other hand, this reflects the standard population of the neurorehabilitation clinic. In assessing the persistence of achieved improvement in motor functions after RAGT, it was not possible to examine all patients who had received RAGT (five patients did not come to the follow-up visit for various reasons).
Conclusion
The study results indicate that the intensive regimen of the robot-assisted gait training can clinically significantly improve gross motor functions in adolescent and young adult patients with CP. There was a statistically and clinically significant improvement in patients in the experimental group compared to the conventional therapy. Furthermore, such improvement has also persisted after 3–4 months.
Intensity, duration, and frequency of RAGT are still the subject of ongoing clinical research. This should not only focus on which therapeutic intervention could be superior to the other, but rather on how one type of therapy could be beneficial for a specific pathology using pre-defined therapeutic objectives, and taking into account the severity of disability according to GMFCS and the age of the patient (Schroeder, 2014). Studies should include information on specific parameters of the therapy (e.g. active patient’s contribution to walking, total walking distance, total therapy duration, walking speed during the training, and weight bearing) allowing specific data, values and knowledge to be obtained about the optimum dose of support using robotic technologies. As a result, this information can help to select and determine the timing of the intervention in the clinical practice (Aurich, 2015).
Conflict of interest
The authors declare no potential conflicts of interest with respect to the authorship and/or publication of this article.
Funding
The authors received no financial support for the research and/or authorship of this article.
Footnotes
Acknowledgments
The authors would like to express their appreciation to all the subjects and their families for their co-operation and participation in this study. We thank the physiotherapy teams of both centres for their assistance and cooperation.
We are grateful to Alojz Halas - director of the Rehabilitation Centre Harmony, for support and willingness to help in performing this study.