
Abstract
BACKGROUND:
New and innovative approaches are needed to overcome the barriers to engaging people in physical and leisure activity after stroke. Outdoor cycling, including the use of adapted or electric bicycles, may be one approach. However, perceptions of stroke survivors on this topic have not yet been explored.
PURPOSE:
To explore a sample of stroke survivors’ perspectives, who expressed an interest in cycling, about cycling and the use of electric bicycles.
METHODS:
A convenience sample of stroke survivors were identified through focus groups at a ‘Cycling after Stroke’ event, local stroke support groups, and structured interviews at a national conference for stroke survivors. Quantitative data were analysed descriptively, and qualitative data analysed thematically.
RESULTS:
Data were collected from 21 stroke survivors, seven of whom were current cyclists. All participants were independently mobile with, or without, the use of a walking aid. Themes oriented around the value of cycling (e.g. getting out of the house, doing something for yourself, and feeling part of a community); concerns and challenges (safety and negotiating adaptations); and how they could be overcome (starting slowly and identifying sources of assistance).
CONCLUSION:
Outdoor cycling may be a worthwhile approach to increasing physical and leisure activity after stroke. However, barriers still exist and need to be addressed to provide inclusive opportunities for adapted and electric cycling for stroke survivors. Due to the small sample size and bias population, further research is needed to explore stroke survivors’ perspectives on cycling to provide solutions to overcome the barriers identified.
Introduction
Despite a wealth of evidence supporting the role of physical activity in post-stroke recovery [1] and the prevention of recurrent strokes [2], low levels of physical activity persist amongst stroke survivors [3]. Six months after a stroke, over half of stroke survivors also report that their lives are lacking some aspect of social, recreational, or purposeful activity [4, 5]. Returning to outdoor activities has been identified as a particular concern for people after stroke [6], with nearly half of stroke survivors experiencing outdoor mobility restrictions [7]. Barriers to activity after a stroke include concerns around balance and fear of falling [8], and a lack of services, transport and support [9–11]. Novel and innovative approaches are needed that can support stroke survivors in achieving recommended levels of physical activity (i.e. 150 minutes or more of moderate intensity physical activity per week [12]).
Cycling may be a feasible and acceptable way of increasing outdoor leisure opportunities for some stroke survivors. Some of the advantages of cycling are that of being seated whilst exercising [13], and the option of being in either an upright or semi-recumbent position [14] depending on the requirement of the user. Cycling is also a functional, repetitive activity [15] and encourages use of the affected side [14]. There is a growing body of evidence demonstrating the increased beneficial effects on wellbeing and self-esteem when exercising in natural environments opposed to synthetic or clinical environments [16, 18]. Yet, the current evidence base for cycling after stroke is limited to stationary cycling in the early phases of rehabilitation [15, 21]. Additionally, there are recent developments in cycling, including the development of motor-assisted bicycles that have yet to be explored in the context of stroke. Electric bicycles (e-bikes) for example, have a battery-operated electric motor that can be utilised to assist the cyclist during cycling. Sales of e-bikes are increasing in the UK [22] with the reported benefits including a reduction in muscle fatigue, exertion, and physiological stress [23]. However, the use of these bikes and the perceptions of stroke survivors towards cycling on e-bikes has not yet been explored within in Ireland, the UK or worldwide to the authors’ knowledge.
The aim of our study was to explore perspectives of a sample of stroke survivors’ who expressed an interest in cycling, about cycling and the use of electric bicycles.
Methods
This was a sequential exploratory mixed-method design [24] consisting of two phases - focus groups (phase 1) and structured interviews (phase 2) (see Fig. 1).
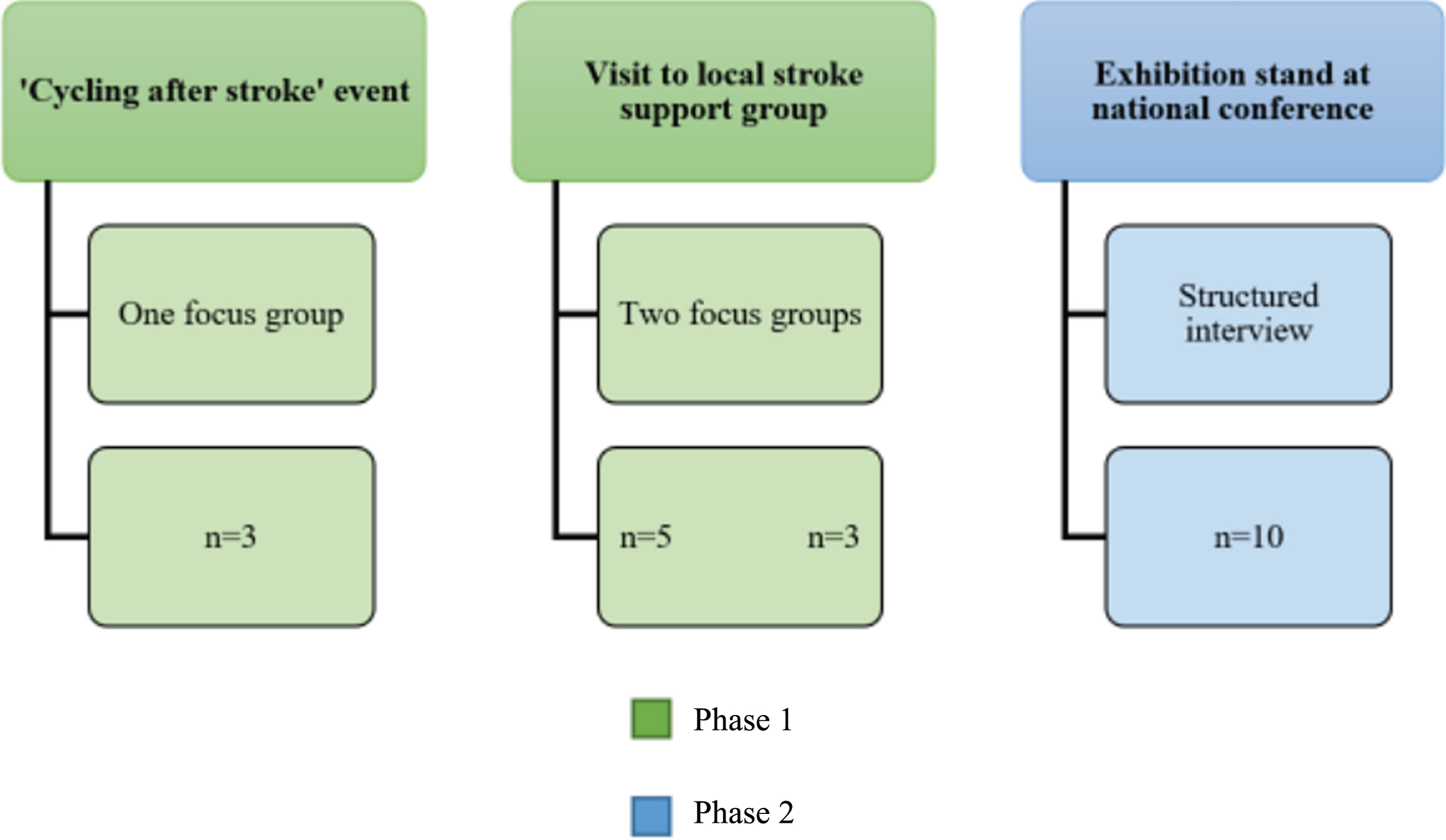
Overview of data collection.
For phase one, we identified a sample of stroke survivors with a range of post-stroke cycling experiences using a convenience sampling strategy. A flyer advertising the ‘Cycling after Stroke’ event was circulated to existing contacts who work with people with stroke. A local stroke support group expressed interest in the event but were unable to attend on the day so a follow-up visit to the group was organised. Participants were recruited for the focus groups through (1) a one-off ‘Cycling after Stroke’ event held at a university sports arena in July 2016; (2) a visit to a local stroke support group.
For phase two, participants were recruited for structured interviews at an exhibition stand at a national conference for people after stroke. Stroke survivors at the conference were asked if they were interested in taking part in a structured interview. To be eligible to participate in the study the person had to have had a stroke. Carers were allowed to be present. The researchers explained that by participating in the structured interview the participant was giving their voluntary consent to be part of the research project.
Data collection
During phase one, we held one focus group at the ‘Cycling after stroke’ event and two focus groups at the local stroke support group. Focus groups were selected to allow for interactive discussion [25] between participants who were likely to have a range of experiences of outdoor cycling after their stroke. A short topic guide consisting of open questions was used to structure discussions (Appendix I) which were audio recorded.
In the second phase, we collected data using structured interviews with consenting attendees at a UK Stroke Assembly, which is a national conference with a target audience of anyone who is affected by stroke. Focus group data, together with findings from the literature, were used to inform the development of the structured interview guide (Appendix I). In the exhibition area of the conference, both the research team and an electric bike company known to the team each had a stand. Due to the proximity of the electric bike stand to the research team’s stand, and to minimize any bias, it was made clear to all potential participants on initial introduction that the researchers were conducting independent research relating to cycling and the use of electric bicycles after stroke. A member of the research team (JJ, OG) read each question of the structured interview aloud and recorded on paper the answers given and any extra verbal information provided by the participants.
Data analysis
Audio-recordings of the focus groups were transcribed and imported into NVivo11 for thematic analysis. The approach to analysis was deductive in nature, with a view to identifying and reporting patterns in the data set that reflected participants’ perspectives on the feasibility of participating in outdoor cycling and the potential utility of electric bicycles. Following the guidance by Braun and Clarke [26], transcripts were read a number of times for understanding. Two members of the research team (MF, AK) then independently analysed the transcripts to produce an initial set of codes. These codes were reviewed in conjunction with (NM) and collated into preliminary themes. The extent to which preliminary themes reflected the data set was checked, prior to producing a refined set of themes. To reduce the burden of participation, member checking was not carried out.
The quantitative data collected in the structured interviews were analysed descriptively (JJ, NG, OG) and compared with the themes from the focus groups.
Ethical approval and reporting
All participants had the opportunity to read an information sheet and then provided written informed consent to allow audio recording of focus groups prior to data collection. For the structured interviews, the researchers explained that the participant was giving their voluntary consent to be part of the research project as stated at the beginning of the structured interview sheet (Appendix I). This study conformed to the Declaration of Helsinki and received approval from the University of Central Lancashire Research Ethics Committee, number STEMH 474 (focus groups) and number STEMH 647 (structured interviews).
Results
Characteristics of the sample
In total 21 stroke survivors took part, 14 males and 7 females. Eleven stroke survivors participated in phase one (three focus groups), and ten stroke survivors completed a structured interview for phase two (Fig. 1). Of the eleven participants in the focus group, two were actively cycling, one using a custom recumbent three-wheeled bicycle and the other using a standard road bicycle. The remaining nine focus group participants were not currently cycling but had recently had the opportunity to trial-adapted bicycles.
Of the ten participants in the structured interview, seven were male, three were female and 50% were over the age of 60 years. The average number of years since having their stroke was 9, ranging from 3 to 30 years. Five of the ten participants in the structured interviews were currently cycling, one using a balance bike, one using a tandem, one using an electric bicycle, and two using a standard bicycle. All participants were independently mobile with, or without, the use of a walking aid.
Value of cycling
When asked about reasons for taking up cycling, or returning to cycling after their stroke, three themes were evident in the focus group discussions: (i) improved mood through being outdoors, (ii) doing something for yourself and (iii) being part of a community. These findings also emerged in the structured interviews; five participants identified that doing something for yourself and being part of a community as important. Health and fitness was the main reason for cycling, and three of the five reported social reasons for cycling.
During the focus groups, participants discussed how finding themselves stuck in the house after a stroke contributed to problems of low mood. Taking part in an outdoor activity, in the form of cycling, provided a valuable opportunity to counter this and enhance their wellbeing.
I wanted to get out of the house, you feel cooped up in the house after a while, you want to be outside you want to breathe the fresh air and be away from being cooped up. That being cooped up adds to feeling a little bit more down as time goes on doesn’t it
Focus group participants stressed the importance of having the opportunity to do something for themselves after their stroke. A number of participants provided detailed reflections on their time in rehabilitation, where they felt their opportunity to assess risk, and make decisions for themselves, was often revoked. One participant provided the following example to illustrate their experience:
... one weekend I thought ‘I know! I’ll get out the wheelchair and see if I can get up the stairs’ ... so I went up on my bum one step at a time and I got to the top I felt really great, like I achieved something. When I got back to rehab and I happen to mention to a physio passing or an OT, I don’t know who to blame [laughter], a week or two later when they had a case conference and I was sitting here listening to them that I had done this awful thing and gone upstairs and I felt naughty as if I shouldn’t have done it ... and I think the whole pressure of ‘be careful’ and ‘don’t do that’ I think needs to change with rehab, you know ‘try this’, ‘do this’, ‘push yourself a little’; okay you fall over you’re not going to break well not too badly anyway
Experiencing a sense of achievement after participating in cycling activities was evident across all of the focus group discussions. Participants emphasised the importance of ‘giving it a go’ by themselves and highlighted that the resulting tiredness was experienced positively.
You know I wanted to do it independently I didn’t want to go on one with the two seats, one of the helpers wanted to go one with me but I said no, it won’t prove I have done it, I have got to prove I can do it
I was so fatigued after the stroke that it was nice to have the cycling to create a different tiredness, a tiredness that I remembered from pre-stroke was because I was physically having a go, it was nice to feel that tired instead of fatigued from the stroke
The final aspect discussed by participants was how cycling afforded them the opportunity to feel part of a wider community.
You know, since I’ve had this trike, one of the things that sort of amazed me when I’m cycling along and proper cyclists come past they wave ... you are part of that group ... and you’re not labelled you know, we’re all in this together!
... but the joy of it, the joy, like fitting helmets you know [laughter] took me ages to fit a helmet, and she’s [coordinator] going “Don’t take that bike, don’t take that bike, I’ve got to check the tyres!” You know, so there was a lot of camaraderie with it which was the enjoyable bit.
Concerns around cycling
Participants reported a number of concerns that were most often oriented around safety and practical issues during both phases. Although some focus group participants were able to try two wheeled bicycles, the majority opted for a three-wheeled bicycle to accommodate concerns around balance. Five of the ten structured interview participants reported fear of falling as a discouraging factor, with three of the non-cyclists reporting additional concerns relating both to keeping hold of handlebars and keeping feet on the pedals. Participants in the focus groups, who had the opportunity to trial bicycles, also expressed some concerns over adaptations that intended to overcome stroke related impairments but could inadvertently increase anxiety or risk of falls for participants.
... because I thought maybe these bikes would be, depending if you’ve had a stroke, you can put a strap on the pedals, put a strap around the left hand side, put a strap around the right hand side depending on which foot is difficult, that’s the best route for you. But then I thought afterwards, you can’t stop because if that foots on the pedal you have to stop that way, getting your feet out you’ll be collapsed and hit on the floor.
Most participants said during the focus groups that they would be unlikely to cycle on their own or on the roads due to safety concerns. Traffic was the primary reason for avoiding cycling on roads and one participant joked:
On the cars coming too close I was told there is research, proper research, that showed that cars go closer to cyclists in Lycra than they do to people not dressed in Lycra [laughter] ... so the secret is to look as unprofessional as possible!
These findings were echoed in the structured interview data where four of the ten participants reported other road users as a discouragement from cycling.
Overcoming challenges
Focus group participants reported that (i) starting slowly, and (ii) having help could assist in overcoming some of the identified concerns. For example, one participant discussed the option of starting on an indoor training device to get used to being on a bike, with another participant outlining that the local authority cycling sessions provided an opportunity to test out cycling before potentially progressing to purchasing a bicycle of your own:
If you practice on these [bicycles in group sessions] I suppose and you’re good with them you could think, ah, maybe I could buy my own bike now that I’m used to it, so it’s a good way of testing if you could do it isn’t it and then you can buy your own if you progress
Participants in the focus groups also spoke about the need for practical support for transporting and getting on and off the bicycles. However, only two of the ten participants in the structured interviews identified this as an issue. Perspectives on the potential value of motor assistance were generally positive as many participants felt that they were unable to do as much as they would have liked on the bicycles. Additionally, participants identified disadvantages such as weakness in particular positions, being unable to stand on the pedals to generate additional force, and other non-stroke related problems that affected their ability to pedal that could be helped by using a motor assisted bicycle.
I persevered, I had it the same as him, I did two laps and the first lap was fairly easier than the second one. It was just ... it was impossible and I would have loved to carry on but that was that.
Because I have something wrong with my groin, I had a fractured pelvis you see and it’s my left groin a bit. So then it [my leg] was so high I couldn’t get my leg back down with the pedal to get that going so electrical would have made it easier in that instance
In the structured interviews, eight of the ten participants expressed that they would be interested in using an electric bicycle but identified the price as the most discouraging factor. The one participant who already owned an electric bicycle found it to be useful and practical.
Discussion
We identified three themes in this study that captured the stroke survivors’ perspectives of outdoor cycling. The themes related to the value of cycling, the concerns and challenges of cycling, and then how these concerns may be overcome. Values of cycling that were highlighted included getting out of the house and enjoying the fresh air. Participants also highlighted the potential social element provided when cycling in a group setting, and through feeling part of the wider cycling community. The benefits of group exercise that provide an opportunity for social engagement, especially with people who are experiencing similar health conditions, has been highlighted in the literature [8, 27]. Additionally, greater engagement in valued activities has been shown to be positively associated with improvements in emotional well-being after stroke [28]. None of the participants in this study reported an interest in cycling for practical purposes, which is reflective of the common UK population [29].
Participants did however identify numerous concerns, the primary one being safety whilst cycling. Safety is often considered the most important factor influencing cycling participation in the general population, particularly for women, children and the elderly [29]. Although some participants felt confident to cycle on the road, the majority of participants identified that they would be prefer cycling in spaces where no traffic would be present. Safety also included concerns around balance, falling, and being able to keep upper and lower limbs safely in position when cycling. A correct bespoke setup is said to be essential for optimising performance [30]. However, for many participants this involves the use of large and weighty adapted bicycles with implications for manoeuvring the bicycles, and for transportation.
Having assistance from others was identified as a crucial element to overcome some of the identified challenges. Participants, in this small sample sized study, had generally positive perspectives on the use of motor assistance. Power assisted, or electric bicycles, are becoming increasing popular in some parts of the world [31]. More recently, there are examples of how electric bicycles have been adapted to accommodate impairments resulting from other neurological conditions (e.g. cerebral palsy [32]) which may provide some insight into the optimisation of motor assisted bicycles for a stroke population. Some of the perceived benefits of electric bicycles in the general population include an improved sense of health and wellbeing and being able to cover greater distances in a shorter period of time with less effort [22]. However, various barriers are still present, most notably the high cost, which was identified by the sample of stroke survivors in this study.
All participants in this study self-selected to take part at the events ‘Cycling After Stroke’, local stroke support groups and a national stroke conference. Therefore, bias was introduced to the convenient sample of participants recruited, due to the individuals attending the events being actively engaged in their rehabilitation and interested in cycling already. As such, the results may represent an overly positive view. All participants were also independently mobile with, or without, the use of a walking aid. There are likely to be additional limitations for more severely impaired stroke survivors that are therefore not represented in this study. Study participants had a mix of experiences of cycling, and the perspectives of the majority was based on a one-off recent experience of trialling adapted bicycles. Additionally, perspectives on the utility of electric bicycles are based on speculation, rather than experience, for the majority of participants.
Conclusion
Outdoor cycling may be a worthwhile approach to increasing physical activity after stroke, but further work is needed to develop solutions to existing barriers to participation. The likely benefits of this approach may include increased opportunities to get out of the house, participation in ‘green exercise’ and increased social contact with other stroke survivors and the wider cycling community. This study has highlighted that barriers still exist for people after stroke who are interested in cycling, and would need to be addressed to provide inclusive opportunities for adapted and electric cycling for stroke survivors. However, due to the small sample size and bias population used, the findings of this study cannot be generalised. Therefore, more research is needed to explore stroke survivors’ perspectives on cycling to provide solutions to overcome the current barriers identified.
Conflict of interest
The authors report no conflicts of interest.
Footnotes
Appendix I: Data collection tools
Acknowledgments
We would like to acknowledge the participants who gave up their time to contribute to this study. This article presents independent research (focus groups) funded by the National Institute for Health Research Collaboration for Leadership in Applied Health Research and Care North West Coast (NIHR CLAHRC NWC). In addition, the European Regional Development Fund (ERDF) as part of the European Structural and Investment Funds Growth Programme 2014-2020 funded the structured interviews through the UCLan Innovation Clinic. The views expressed are those of the author(s) and not necessarily those of the NHS, the NIHR, the ERDF programme or the Department of Health. We would also like to thank Ian Gibbs at I-Cycle Electric (Huntley’s Country Stores, Samlesbury, PR5 0UN) for providing the electric bikes and technical support throughout the research study.