
Abstract
INTRODUCTION:
Gait engages motor and cognitive neural pathways. However, progressive deterioration of motor and cognitive function is characteristic in Parkinson’s disease (PD). We explored relationships between motor impairment, cognitive function, daily functioning, and gait in people with PD. We hypothesized there would be a stronger relationship between walking and cognitive function as gait task complexity increased.
METHODS:
Community-dwelling participants with PD were assessed on motor impairment [United Parkinson’s Disease Rating Scale Motor Subscale (UPDRSm)], cognitive function [Repeatable Battery for the Assessment of Neuropsychological Status (RBANS)], daily function [Schwab & England (S&E) ADL scale] and mobility [Timed Up and Go (TUG)] under single and dual task conditions. Analyses included Spearmans’ rank correlations coefficient to determine relational strengths between outcomes and separate forward stepwise multiple linear regressions to predict dual task gait performance.
RESULTS:
Forty-five participants [age Mean (M) = 68.93±7.78 years; 32 male/13 female; UPDRSm, M = 25.24±11.93] completed this study. RBANS was poorly related to TUGmotor and TUGcognitive. UPDRSm (rho = 0.524; p < 0.001) and S&E (rho = –0.589; p < 0.001) were moderately related to TUGmotor ; S&E (rho = –0.581; p < 0.001) to TUGcognitive. S&E (R2 = 0.234; F (1,43) = 13.14) and RBANS Language subscale (R2 = 0.071; F (1,42) = 4.31) were predictive of TUGmotor performance; S&E of TUGalone (R2 = 0.150; F (1,43) = 7.56) and TUGcognitive performance (R2 = 0.375; F (1,43) = 25.81).
CONCLUSIONS:
Daily function appears more closely related to dual task mobility than separate assessments of motor and cognitive function in this population.
Introduction
Typical human gait requires motor skill and cognitive function to successfully negotiate the environment [1, 2]. The ability to execute rhythmic motor activation, initiate and terminate movement, maintain dynamic stability, and successfully adapt to the demands of a changing environment [3] result in an effective and energy efficient gait pattern under normal conditions [4]. The addition of a simultaneously performed secondary task (e.g. dual tasking), necessitates divided attention and intact executive function. Thus, successful navigation of dual task gait requires proficient interplay between motor and cognitive capabilities [5]. By contrast, a hallmark of Parkinson’s disease (PD) progression is the emergence of gait dysfunction exacerbated under dual task conditions [6]. Difficulty with divided attention and executive function in people with PD [7] results in motor-cognitive interplay deficits during gait such as decreased cadence, decreased stability, increased step variability [5], difficulty with turns [8] and increased risk of falls [9].
Characterized by motor and non-motor impairments, individuals with PD often display difficulty balancing the cognitive task and motor function during gait [10]. This difficulty may be partially explained by complex cortico-striatal interactions between specific cognitive domain (i.e. processing speed) associations with motor symptoms (postural stability) in PD [11, 12]. Consequently, people with PD are at an increased risk of fall [13] with estimates suggesting over half of falls in people with PD occur during dual task activities [14].
Established literature describes a reciprocal hierarchical relationship between motor and cognitive neural pathways [15–17] where pathology in either component produces gait impairment [18]. For example, motor control of gait may diminish earlier in PD resulting in greater dependence on the cognitive components to produce gait. Yet, the specific contributions between motor and cognitive components necessary during dual task gait in people with PD remain unclear. Moreover, as motor and cognitive components are typically evaluated separately, concurrent assessment through dual task gait may be a valuable to the clinician [5]. Therefore, the purpose of this study was to explore the relationships between motor impairment, cognitive function, and daily function during dual task mobility in people with PD. We hypothesized a stronger relationship between walking and cognitive functioning as the gait task complexity increases.
Methods
Participants
Individuals with PD were recruited to participate in this study by flyer and word-of-mouth from local community centers, hospitals, physician clinics, and PD support groups. Participants were ambulatory community dwelling individuals who were diagnosed with PD based on the UK Brain Bank criteria, between ages 40 to 85 years old, and had been on a stable medication regime for at least 30 days. Participants were excluded if non-ambulatory, uncontrolled medical problems were present (i.e. hypertension, diabetes), coexisting neurological condition other than PD, or if cognitive capacity was less than the tenth percentile compared to aged normative scores on the RBANS assessment.
Procedure
This study was approved by the local university Institutional Review Board. After providing informed consent, participants completed testing over a single session during medication “ON” time where the positive effect of the medication was evident based on individual medication schedules as reported by each participant. Testing consisted of completing the following outcome measure assessments in sequential order within a two hour timeframe: Unified Parkinsonism Disease Rating Scale –motor subscale (UPDRSm) [19], Schwab and England Activities of Daily Living Scale (S&E) [20], Repeatable Battery for the Assessment of Neuropsychological Status (RBANS) (a multi-domain cognitive function scale) [21], and a single [Timed Up and Go alone (TUGalone)] and dual task mobility paradigm (TUGmotor and TUGcognitive) [22]. This approach has been used by others to assess motor impairment, cognitive function, and daily function during dual task mobility in people with PD [23–25].
Outcome measures
Motor impairment
Motor impairment was assessed by the motor subscale of the original UPDRS (UPDRSm). Ranging from a score of 0 to 108, a lower score on the UPDRSm indicates less motor impairment. The UPDRSm has excellent concurrent validity (r = 0.96) with the original UPDRS [26] and high internal consistency [26]. The UPDRSm is also strongly related to the Hoehn and Yahr scale (r = 0.87) [27].
Cognitive function
The RBANS is comprised of 12 subtests combined into five index scores (attention, language, visuospatial/constructional abilities, immediate recall, and delayed recall) to examine global cognitive function [28]. Index scores are summed and converted into a single total scaled score. With a range from 40 to 160, higher scores on the RBANS reflect better cognitive function. A total scaled score of 100 is equal to the 50th percentile of the aged normative population. The RBANS total score has strong internal consistency in healthy elderly (r = 0.806) [29] and people with PD (r = 0.74) [30] and a modest relationship with whole brain volume (r = 0.27) [31]. Furthermore, the RBANS is able to distinguish between various dementias (i.e. Alzheimer’s disease and PD dementia), discriminate patterns of cognitive impairment [21], and reveal reliable change on several subtest scores in PD [32]. We elected to use RBANS because of its comprehensive nature to examine multiple areas of cognitive function.
Daily function
The S&E is a self-reported activity of daily living (ADL) function scale from 0 to 100. A higher percentage indicates greater independence and less activity limitations. Developed for people with PD and used by physicians and other rehabilitation specialists due to its brevity and simplistic nature, the S&E quantifies the impact PD has had on the person’s ability to cope with daily function [20]. The S&E has adequate inter-rater reliability (ICC = 0.60–0.65) and test-retest reliability in people with PD (ICC = 0.7) [20].
Single and dual task mobility
The TUG is a simple method of quantifying mobility and the effect of an additional cognitive demand in people with PD [22]. The TUG was used to assess motor-cognitive interplay under three conditions: TUGalone, TUGmotor and TUGcognitive [33]. The TUGalone is a single attention mobility task where the participant was required to stand up at walk 3 meters at a normal and safe pace, turn 180 degrees, walk back, and sit down. During the TUGmotor, the participant carried a full cup of water with one hand of their choice throughout the mobility task. During the TUGcognitive, the participant counted aloud backwards by three from a randomly selected number between 50 to 100 during the mobility task. The time required to complete each mobility task was recorded. Participants were allowed one practice trial of the TUGalone to familiarize them with the mobility task. All TUG tasks were performed under the direct supervision of one of the investigators in a randomized order. The TUG has excellent inter-rater (r = 0.99) and intra-rater (r = 0.98) reliability in people with PD [34]. The TUGcognitive has a positive predictive value of 71% for falls in comparison to 42% for the TUGalone for people with PD [35].
Data analysis
Statistical analysis was performed using SPSS (Version 24.0). Descriptive statistics were used to analyze participant characteristics and performance on single and dual task mobility tests (TUGalone, TUGmotor, TUGcognitive). Preliminary analyses were performed to assess assumptions of normality and linearity and included the Kolmogorov-Smirnov test. As our data distribution did not meet the assumptions for conducting a parametric analysis, we elected to use a non-parametric alternative for subsequent statistical analyses. Relational strengths between the UPDRSm, RBANS total scaled score and subscales, S&E and TUG conditions were determined by Spearmans’ rank correlations coefficient. This approach has been used elsewhere with functional measures such as the TUG [36, 37]. Three separate forward stepwise multiple linear regressions were used to analyze the predictability of motor impairment (UPDRSm), cognitive function (RBANS), and daily function (S&E) on single (TUGalone) and dual task mobility (TUGmotor, TUGcognitive). Age was included in the analysis as a potential confounding variable. Tests of multicollinearity and heteroscedasticity assumptions of regression were performed. Significance level was set at 0.05 for all analyses.
Results
Forty-five people with PD completed our study. Refer to Table 1 for participant characteristics and Fig. 1 for performance on RBANS and individual subscales. On average, our typical participant was a community dwelling 69 year old male with a diagnosis of PD for 9 years who reported taking twice as long to complete ADLs due to PD symptoms including mild-to-moderate motor symptoms and cognitive function performance in the 16th percentile. Nearly 75% (n = 34) of our participants reported rare falls or no falls within the last year. The remaining 25% of our participants (n = 11) indicated an average of one or more falls per day. As expected, average time required to complete the TUG tasks increased with task complexity (i.e. TUGcognitive more complex than TUGalone).
Participant characteristics (n = 45)
Participant characteristics (n = 45)
Note: PD = Parkinson’s disease; UPDRSm = Unified Parkinson’s Disease Rating Scale Motor Subscale; RBANS = Repeatable Battery for the Assessment of Neuropsychological Status; % = percentage; SD = standard deviation; TUG = Timed Up and Go; s = seconds.
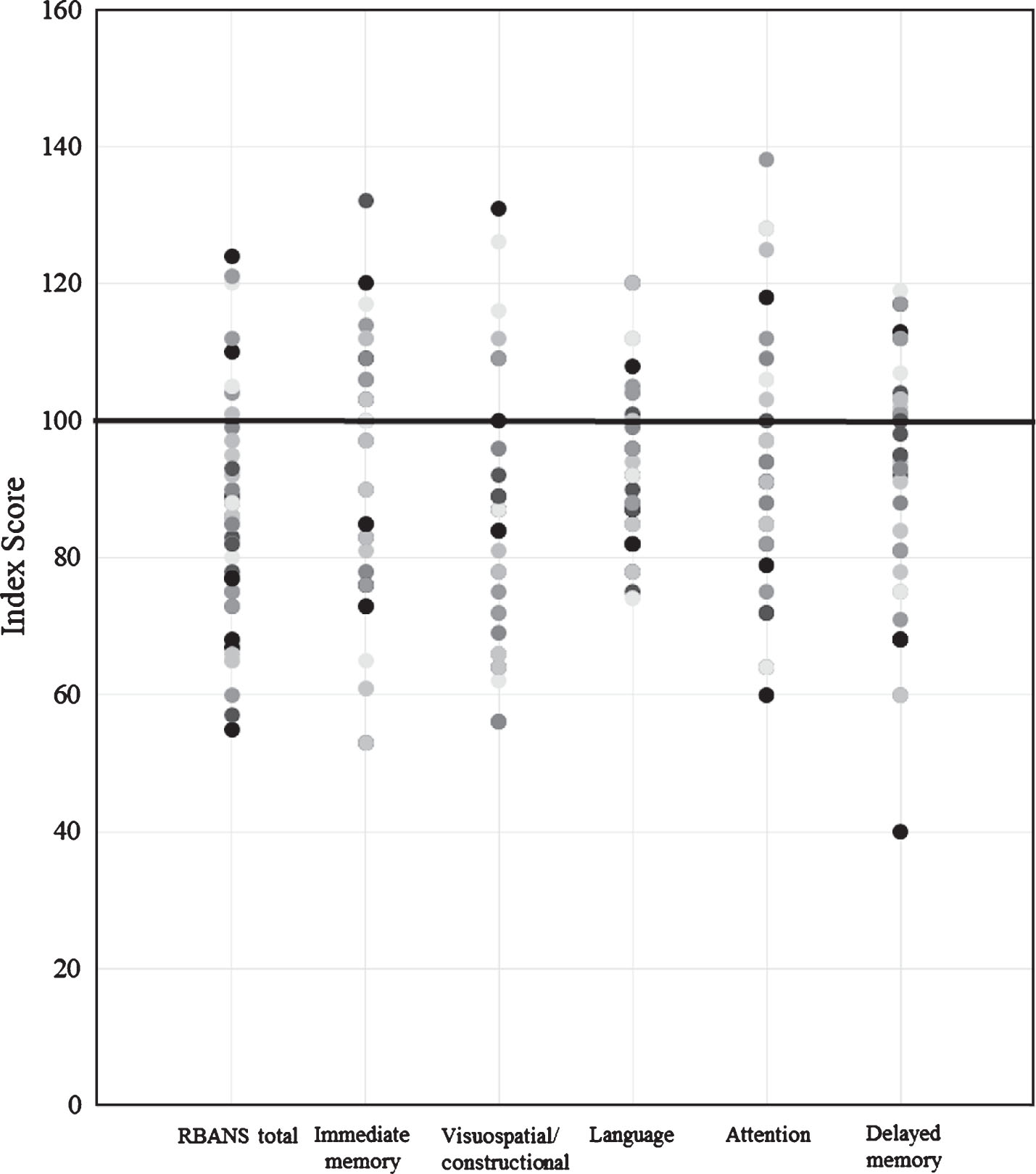
Participant Performance on Repeatable Battery for the Assessment of Neuropsychological Status (RBANS) and Subscales (n = 45). Note: 100 represents 50th percentile of the aged normative population.
Spearmans’ rank correlations coefficient was used to evaluate the strength of the relationship between TUG tasks and UPDRSm, RBANS (total scaled score and subscales), and S&E. Strength of correlations were determined based on the following scale: 1 to 0.25 = little to no relationship, 0.25 to 0.50 = fair relationship, 0.50 to 0.75 = moderate to good relationship, and greater than 0.75 = good to excellent relationship [38]. In general, the TUGalone had no correlation with the RBANS total scaled score (rho = –0.072; p = 0.572), but significant relationships with UPDRSm (rho = 0.375; p = 0.011) and S&E (rho = –0.413; p = 0.005). For the TUGmotor, there were a significant correlations with the RBANS total scaled score (rho = –0.266; p = 0.034), UPDRSm (rho = 0.524; p < 0.001) and S&E (rho = –0.589; p < 0.001). The TUGcognitive had no correlation with the RBANS total scaled score (rho = –0.22; p = 0.080), but significant correlations with the UPDRSm (rho = 0.495; p < 0.001) and S&E (rho = –0.581; p < 0.001). Of the RBANS subscale scores (immediate memory, visuospatial/constructional, language, attention, delayed memory), the Language subscale was consistently most closely related to TUG tasks. See Fig. 2 for details. Age was not significantly correlated with UPDRSm (rho = 0.122; p = 0.425), S&E (rho = –0.068; p = 0.587), RBANS total scaled score (rho = 0.164; p = 0.455) or any of the TUG conditions [TUGalone (rho = 0.200; p = 0.279); TUGmotor (rho = 0.202; p = 0.190); TUGcognitive (rho = 0.281; p = 0.097)].
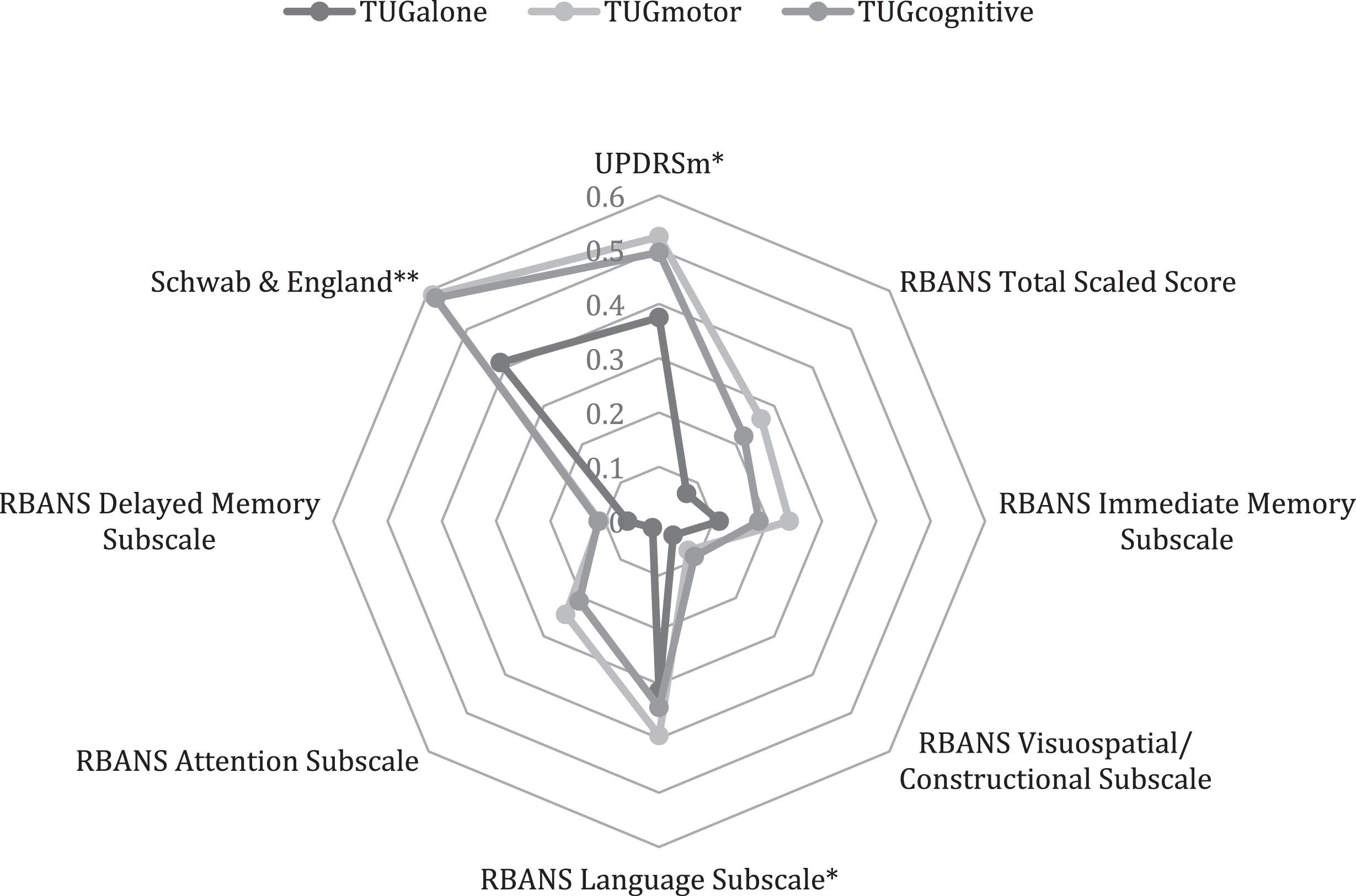
Radar Plot of Relational Strength Between Motor Impairment, Cognitive function, and Daily function on Dual Task Gait Conditions (n = 45). Note: UPDRSm = Unified Parkinson’s Disease Rating Scale Motor Subscale; RBANS = Repeatable Battery for the Assessment of Neuropsychological Status; Schwab & England = Schwab and England Activities of Daily Living Scale; TUG = Timed Up and Go; *=correlation is significant at the 0.05 level for TUGalone and 0.01 for TUGmotor and TUGcognitive; **=correlation is significant at the 0.01 level for TUGalone, TUGmotor and TUGcognitive; analysis with Spearmans’ rank correlations coefficient.
Forward stepwise multiple linear regression indicated that only the S&E was predictive of performance on the TUGalone (R2 = 0.150; F (1,43) = 7.56) and TUGcognitive (R2 = 0.375; F (1,43) = 25.81). Both the S&E (R2 = 0.234; F (1,43) = 13.14) and RBANS Language subscale (R2 = 0.305; F (1,42) = 4.31) were predictive of TUGmotor performance. Refer to Table 2 for details.
Summary of Multiple linear regression analyses predicting single and dual task performance
Note: TUG = Timed Up and Go; S&E = Schwab & England Activities of Daily Living Scale; RBANS = Repeatable Battery for the Assessment of Neuropsychological Status; Model Summary: TUGalone (R2 = 0.150; R = 0.387; F (1,43) = 7.56); TUGmotor (R2 = 0.305; R = 0.553; F (1,43) = 4.307); TUGcognitive (R2 = 0.375; R = 0.612; F (1,43) = 25.81).
The post hoc power analysis based on the significant TUGcognitive regression model (N = 45) revealed a large effect size of.51 (f2) and the achieved power was.98. Further, multicollinearity and heteroscedasticity assumptions of regression were not violated. Slight, but not extreme variations, of error distribution was observed by looking at P-P plots.
In general, motor impairment (UPDRSm) and daily function (S&E) were more closely related to mobility tasks (TUGalone, TUGmotor, TUGcognitive) than cognitive function (RBANS total scaled score). Further, the relationship between mobility tasks and motor impairment and daily function strengthened as the mobility task complexity increased (see Fig. 2). By contrast, the cognitive contribution to dual task performance was less consistent. Moreover, the relative contribution of motor function and cognitive performance were unequal and varied with the demands of the mobility task. That is, motor-cognitive interplay appears to be task dependent in people with PD [2].
People with PD demonstrate significant gait variability [39] during motor-cognitive interplay scenarios (i.e. dual tasking) contributing to risk of falls [5, 40]. While motor and cognitive dysfunction common to people with PD are typically evaluated separately, there appears to be a need in clinical practice for concurrent assessment through dual task mobility [5]. In this study, we explored the relationships between motor impairment, cognitive function, daily function, and dual task mobility in people with PD. In contrast to our hypothesis, we observed a significantly stronger relationship between mobility and motor impairment and daily function, but generally not cognitive function, as the gait task complexity increased.
During a dual task paradigm, task complexity is often increased by the addition of a cognitive load. However, our participants’ cognitive function did not demonstrate a stronger relationship in the context of a cognitively loaded dual task (see Fig. 2). A few reasons may account for this finding. First, our participants had mild motor deficits, but cognitive function capacity was significantly below peer norms (16th percentile). Though the rate of cognitive decline varies widely among people with PD [41], accelerated decline in cognition is generally associated with non-dopaminergic mechanisms corresponding to a ‘postural instability gait difficulty (PIGD)’ motor subtype [42]. Nonetheless, our participants may have drawn on their most ample resource (motor function) while unable to pull from their least available resource (cognitive function) to complete dual task mobility. Further, whereas gait velocity is a known predictor for dual task gait performance [43], cognitive function is more closely linked with impairment and disability in PD [44]. As an example, our participants, of whom nearly 75% were rare or non-fallers, were able to complete the TUGalone in a comparable time frame (11.2 seconds) as reported for non-fallers [45]. Thus, the minimal motor impairments in our sample may have allowed our participants to walk at a faster pace despite a relative low cognitive capacity.
Although gait velocity has been associated with most brain regions [46], recent work suggests that discrete gait characteristics are associated with regional brain function [46]. For example, step length is linked with the parietal and occipital lobes while step width is associated with the inferior parietal lobe and the basal ganglia [18, 47]. Additionally, gait impairments of pace and step variability are indicators of cognitive decline in attention and visual memory [47]. We assessed only the relative walking pace to complete single and dual task gait. Consequently, our ability to comment on the quality of gait as it relates to the cognitive performance of our participants is limited. Nonetheless, there is an apparent need for the clinician to assess gait impairment [dual tasking and discrete characteristics (e.g., step length, step width, stance time)] and cognitive function in a multi-faceted manner.
In this study, neither global cognitive function (RBANS total score) nor individual subscales was strongly related to dual task gait performance. However, the RBANS Language subscale was the most closely related component of cognitive function to mobility performance. The RBANS Language subscale is assessed through picture naming and semantic fluency (i.e. naming as many fruits and vegetables possible in one minute) tasks. While seemingly disparate from performance in mobility, language is recognized as a complex task requiring timely integration of multiple brain regions and is capable of inducing gait deviations during dual tasking [48]. As such, the relationship between the RBANS language subscale and dual task mobility may be partially explained by a common reliance on processing speed necessary to successfully complete both tasks [49]. Deficits in processing speed were previously linked with gait disturbances in people with PD [12]. Interestingly, though dual task mobility is often described as a divided attention task [5, 50], the RBANS attention subscale was poorly related to dual task mobility. The RBANS attention subscale is assessed through a digital span task and a timed coding task [21]. These tasks appear to require a sustained attention rather than alternating or divided attention. Neuropsychological measures such as Trail Making Test B or Paced Auditory Serial Addition Test may test aspects of attention more similar to dual task mobility [51, 52]. Further, our results suggest inclusion of clinical measures emphasizing speed of processing may be most salient to performance on complex mobility tasks.
In this study, daily function (S&E) was more closely related to each of the mobility tasks than either motor impairment or cognitive function. The nature of functional activities of daily living may explain the observed strength of relationship. That is, typical daily function activities such as walking and dressing requires an individual’s attention to be divided among motor and cognitive distractors [53]. Further, daily function was the only predictor for all three mobility tasks and the relative predictive strength increased with mobility task complexity supporting the link between daily function and motor-cognitive interplay in individuals with PD [2, 54]. However, daily function only accounted for 15% to 37.5% of the variance in mobility performance. Others have reported motor symptoms [6], physical activity [55], depression [55], quality of life [5], and aspects of executive function (i.e. processing speed) [5], as important contributors that impact mobility performance. Notwithstanding, the subjective experience of a person with PD in completing daily tasks should provide the clinician a window into potential deficits with complex mobility. Weighing daily task challenges with concurrent assessments targeting dual task mobility will further guide clinicians to optimally manage available motor and cognitive resources in the individual with PD.
From a pathophysiological perspective, dopamine depletion within the striatum and associated circuit connectivity impairs the ability to perform dual tasking. Specifically, disruption of the parallel cortico-striatal circuits leads to dysfunctional motor and cognitive processes during dual tasking [56]. Recent findings suggest this disruption drives an extension of striatal activity into uninitiated cortical regions causing a functional blurring in parallel processing required to perform dual tasking [11]. For our participants, higher complexity of the dual task gait (TUGmotor and TUGcognitive) likely elicited greater functional blurring of the parallel cortico-striatal circuits than single task gait (TUGalone). However, patterns of striatal degeneration are not uniform across all people with PD. In fact, striatal degeneration varies across PD subtypes (i.e. tremor dominant vs. postural instability gait difficulty) [57]. Thus, both task complexity and individualized pattern of striatal deterioration may explain our participants’ abilities to perform daily tasks.
Limitations
This study is limited by several issues impacting our ability to make firm conclusions about the relationship between the UPDRS, RBANS, S&E, and dual task mobility in people with PD. First, our small sample size consisting primarily of mild motor impairments reduces our ability to generalize to a broader PD community. Despite the smaller sample size, post hoc power analysis on the TUGcognitive regression model revealed a large effect size of.51 (f2) and the achieved power was.98 lends support for our findings. Nonetheless, we only performed our post-hoc power analysis on one of regression models. It is likely that the effect size and power observed in the TUGcognitive regression model were not achieved in the TUGalone and TUGmotor regression models. Thus, our results particularly in these models should be understood with caution. Additionally, our participants demonstrated mild motor deficits on average; therefore, our sample is likely not representative of all people with PD. Moreover, though the selected outcome measures in this study may not have comprehensively assessed the desired attributes in our sample. For example, the TUG tasks may not have been sufficiently rigorous to adequately assess the motor-cognitive demands of dual tasking in our sample with mild motor deficits. Lastly, each participant performed all testing during their self-reported “ON” phase. It is possible that the maximal benefit of the medication (e.g., therapeutic window) was not realized across the entirety of the assessment session and thus impacted our findings. Further, we are unable to comment how our findings apply to people with PD during “OFF” phases.
Conclusion
Daily function, as reported by people with PD, appears to be more closely related to dual task mobility performance than individual assessments of motor and cognitive function. However, motor function and cognitive function (particularly speed of processing) may contribute to mobility performance under different conditions. Though cognitive function likely contributes to motor-cognitive interplay in dual tasking, clinicians may find it useful to measure cognitive function using various methods. Further, motor and cognitive dysfunction common to people with PD are typically evaluated separately suggesting a potential need in clinical practice for concurrent assessment through dual task mobility [5]. The results of this study may assist the clinician with assessment and treatment of a person with PD with gait disorder. Future trials may consider the role of PD subtypes in the assessment of motor-cognitive interplay. In particular, multi-dimensional assessments of gait and cognition should be included to obtain a more thorough understanding of this relationship.
Conflict of interest
None to report.