
Abstract
BACKGROUND:
Combined physical and psychological programmes (CPPP) are recommended for people with disabling low back pain (LBP). Cognitive Functional Therapy (CFT) is a physiotherapist-led low intensity CPPP with positive effects in previous studies. The clinical and cost effectiveness of CFT has not previously been evaluated in a randomised controlled trial (RCT) in the United Kingdom (UK) National Health Service (NHS). Before a definitive RCT can be completed it is necessary to determine if completing such a study is possible.
PURPOSE:
To determine the feasibility of completing a definitive RCT, that will evaluate the clinical and cost-effectiveness of CFT in comparison to usual physiotherapy care for people with persistent LBP in the UK NHS.
METHODS:
A pragmatic two-arm parallel feasibility RCT comparing CFT with usual physiotherapy care for people with persistent LBP will be completed. Sixty participants will be randomly allocated to receive CFT or usual physiotherapy care. The primary outcome will be feasibility of completing a definitive RCT. Participant reported outcome measures will be recorded at baseline, three, six and twelve-month follow-up, including disability, pain intensity, quality of life and psychosocial function. Data will be analysed descriptively. A qualitative process evaluation will explore the acceptability of the research processes and interventions.
DISCUSSION:
The rationale and methodological design of a mixed methods feasibility RCT is presented. This study aims to inform the planning, design and completion of a future definitive RCT in the UK NHS. The results will be disseminated through peer reviewed open access journal publication.
Introduction
Low back pain (LBP) disability has increased by more than 50% in the last 25 years, maintaining its position as the primary cause of years lived with disability globally [1]. The economic impact is considerable with costs comparable to that of diabetes mellitus, cardiovascular disease, mental health disorders and cancer [2, 3]. It is suggested this burgeoning trend may be attributed to the inadequacy of previous models of care to effectively manage the complexity of LBP across the biopsychosocial spectrum [4]. An individual’s LBP presentation may reflect a range of physical (i.e. movement avoidance, protective guarding), psychological (i.e. negative LBP beliefs, low self-efficacy, fear of pain and/or movement, depression, anxiety), social (i.e. family and work relationships, socio-economic factors, work satisfaction), lifestyle (i.e. activity levels, sleep) and co-morbid health-related factors (i.e. obesity, mental health) [5–11]. There is growing evidence that many of these factors may interact to mediate the transition from acute to persistent LBP [6, 12].
Existing interventions have been criticised for being reductionist by targeting singular dimensions of the disorder and have, so far, yielded suboptimal outcomes for patients [12]. Treatments that just target physical or psychological aspects of persistent LBP have shown consistently modest effects in reducing pain and disability [13–16]. One systematic review that compared physical, psychological and combined (physical and psychological) interventions for persistent spinal pain reported that only small reductions in pain (measured on a scale between 0–10) (mean difference (MD)<0.5, 95% confidence interval (CI) –1.38–0.38) and disability (standardised mean difference (SMD) = –0.25, 95% CI 0.07–0.43) were sustained across all between-group comparisons [17]. Consequently, identifying effective biopsychosocial interventions for persistent LBP remains a key goal of researchers and clinicians alike [18].
In the United Kingdom (UK), the updated National Institute for Health and Care Excellence (NICE) LBP and sciatica guidelines recommend access to combined physical and psychological programmes (CPPP) for those patients identified at risk of a poor outcome (using a validated risk stratification tool [19]) or where previous self-management strategies and treatments delivered as a package of care (including exercise, manual therapy, pharmacological and psychological therapies) have been ineffective [20]. However, access to CPPP for LBP patients in the UK is limited and where available there is no standardised approach to delivery with heterogeneity in the type (e.g. multi-disciplinary versus single profession delivery, outpatient versus residential), intensity, frequency, duration (e.g. daily/weekly attendance, total hours of contact time) and therefore cost of such programmes. The Department of Health Spinal Taskforce in the UK previously identified the absence of CPPP as the biggest gap in service provision for LBP patients [21], a group who cost the National Health Service (NHS) and society a significant proportion of resources [2].
The National Low Back and Radicular Pain Pathway was a commissioned NHS England pathfinder project that aimed to provide an end to end care pathway for people with LBP and radicular pain and was recently updated to align with the NICE guidelines [22]. The pathway is designed to restrict unwarranted interventions, reduce variations in care and improve timely access to evidenced-based alternatives, including CPPP so that improved patient outcomes and system efficiencies are realised [22]. Whilst the overall pathway has projected significant cost savings and reported improved patient satisfaction [22], clinically important improvements in disability have not been observed in established CPPP [23, 24].
Psychologically informed physiotherapy is a lower intensity, physiotherapy-led form of a CPPP. Psychologically informed physiotherapy augments traditional physiotherapy interventions for LBP, such as manual therapy and exercise, with ‘third wave’ cognitive behavioural principles such as education, relaxation techniques, mindfulness, graded activity and exercise and acceptance-based therapy [25]. A number of psychologically informed physiotherapy approaches for LBP have been developed and evaluated in clinical trials [26–31]. However, a recent systematic review and meta-analysis did not identify long-term improvements in pain (0–10 scale) (MD = –0.25, 95% CI –0.63–0.12) or disability (SMD = –0.06, 95% CI –0.22–0.11) when psychologically informed physiotherapy was compared to usual physiotherapy care in LBP trials. It was postulated that interventions may have failed to adequately integrate cognitive, behavioural and physical aspects of pain and disability and individually tailor management [32]. Cognitive Functional Therapy (CFT), which explicitly integrates these elements, was noted as an outlier in this review with large effect sizes reported for reducing pain (0–10 scale) (MD = –1.50, 95% CI –2.33–0.67) and disability (SMD = –0.91, 95% CI–1.33–0.48) as well as fear of movement, anxiety and depression at twelve-month follow-up [32].
CFT is an individually tailored psychologically informed physiotherapy intervention for LBP, which aims to facilitate sustained self-management [33]. CFT utilises a multidimensional clinical reasoning framework that enables the clinician to identify modifiable and non-modifiable biopsychosocial factors underlying an individual’s LBP. It targets these factors by, helping the patient ‘make sense of their pain’, develop confidence to engage in movement and activity, and adopt positive lifestyle behaviours [33]. CFT has shown clinically important (> 30%) improvements in pain and disability in a number of previous studies [34–37], including two RCT’s in Norway and Ireland [38, 39]. While the eligibility criteria and comparison interventions varied in these RCTs, both demonstrated sustained clinically important (> 30%) improvements with CFT, especially for pain-related disability [38–40]. A recent case-control study, within a secondary care specialist pain centre in Denmark, that included a highly disabled cohort of LBP patients, reported larger reductions in pain-related disability (SMD = 0.52, 95% CI 0.13–0.93) (measured using the Pain Disability Index on a scale of 0–50 where zero represents no disability)) and a 93% cost saving of € 3,688.29 in favour of CFT in comparison to a multi-disciplinary CPPP [36]. However, the clinical and cost effectiveness of CFT has not previously been evaluated in an RCT in the UK NHS or compared to usual physiotherapy care. This is important as there is evidence that complex LBP interventions might not be as effective in different countries and settings [27, 41].
RCT’s are recognised as the ‘gold standard’ research design in determining the effectiveness of different healthcare interventions due to the methodological control exerted over potential confounding factors [42]. Both CFT and usual physiotherapy care can be considered complex interventions [43], lending themselves to evaluation in a pragmatic RCT [44]. However, before the clinical and cost-effectiveness of CFT can be measured in a suitably powered RCT in the UK NHS, it is unknown whether such a trial can be completed [45]. To determine the feasibility of completing a definitive future trial, a pragmatic two-arm parallel feasibility RCT comparing CFT with usual physiotherapy care for people with persistent LBP is proposed.
Considering the concerns reported by physiotherapists regarding their ability to deliver psychologically informed physiotherapy safely and effectively [46–53], the willingness of some patients to engage in such programmes [54, 55] and the challenges inherent in completing RCTs, a nested qualitative study will evaluate the acceptability of the interventions and research processes to participants with persistent LBP and their treating physiotherapists.
The objectives of this feasibility RCT are to determine: The number of eligible participants and actual recruitment rate. Retention rates of enrolled participants. If CFT can be delivered to fidelity by NHS Physiotherapists. The acceptability, return and completion rates of the patient reported outcome measures. The most suitable primary outcome measure and calculate the sample size for a definitive RCT, should feasibility be assured. The type and frequency of adverse events. Adherence rates to the interventions through attendance to scheduled physiotherapy appointments and a self-completed exercise diary. The acceptability of the intervention and the research process as experienced by participants with LBP and physiotherapists.
Methods
The planning and reporting of this protocol has followed the recommendations of The Standard Protocol Items: Recommendations for Interventional Trials (SPIRIT) [56], the Template for Intervention Description and Replication (TIDieR) [57] and the extension of the Consolidated Standards of Reporting of Trials (CONSORT) for pilot and feasibility studies [58]. Qualitative data will be reported in accordance with the COnsolidated Criteria for REporting Qualitative research [59].
This study conforms to the Declaration of Helsinki and received ethical approval from East Midlands Nottingham 1 Research Ethics Committee on the 1st February 2019, reference number 18/EM/0415. The trial was registered with www.isrctn.com on 10th May 2019, ISRCTN12965286, https://doi.org/10.1186/ISRCTN12965286.
The aims and objectives will be met through two phases. In Phase 1, a feasibility RCT will compare CFT to usual physiotherapy care in 60 participants with persistent LBP. In Phase 2, qualitative semi-structured interviews will explore the acceptability of the research processes and interventions to a minimum of ten patient participants, enrolled in Phase 1. Two focus groups will evaluate the acceptability of the training package and participation in the feasibility RCT to all usual care and CFT trained physiotherapists.
Recruitment
Phase 1
Participants will be recruited from a secondary care physiotherapy outpatient service waiting list at University Hospitals of Leicester NHS Trust. Recruiting 60 participants (30 per arm of the study) requires just over one patient per week to be enrolled for the 12-month recruitment phase. The recruitment target is thought to be achievable as the host physiotherapy service receives approximately 500 LBP referrals per month.
Referrals will be screened against the eligibility criteria by departmental physiotherapists during a telephone triage consultation, which is standard practice. Fifteen senior physiotherapists will receive training and supporting material, covering the aims and objectives of the study, the eligibility criteria and the recruitment processes during a departmental training session, lasting one hour. Those patients that are potentially eligible will be asked if they consent to being contacted by the research team. The research team will then provide information about the study, establish a postal or email address for the potential participant to receive the participant information sheet and arrange a study screening appointment. This will be more than one week after the phone call to ensure the potential participant has the opportunity to consider the study information before providing consent.
All potential participants will be given the option of receiving physiotherapy care as usual or taking part in the study. It will be clearly stated that there are two active interventions and that based on current understanding it is not known which is superior. People willing to participate will be consented by the research team and will then complete the baseline assessments, prior to randomisation. The schedule of participant enrolment, intervention allocation and assessments is depicted in Table 1.
Template for the schedule of enrolment, interventions, and assessments
Template for the schedule of enrolment, interventions, and assessments
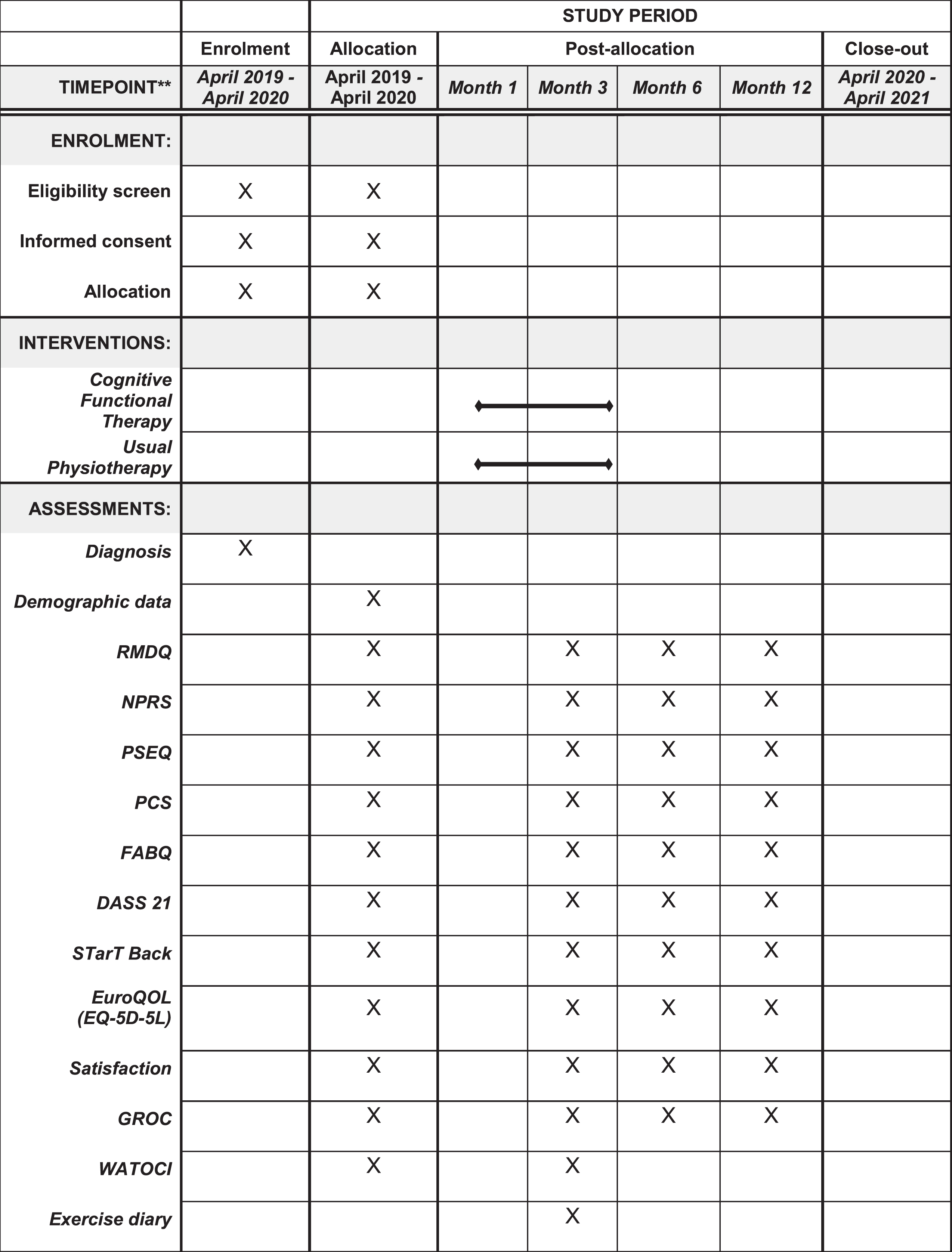
RMDQ; Roland Morris Disability Questionnaire, NPRS; Numeric Pain Rating Scale, PSEQ; Pain Self-efficacy Questionnaire, PCS; Pain Catatsrophising Scale; FABQ; Fear Avoidance Beliefs Questionnaire, DASS 21; Depression, Anxiety and Stress Scale, STarT Back; Sub-groups for Targeted Treatment Screening Tool; GROC; Global Rating of Change Scale, WATOCI; Working Alliance Theory of Change Inventory.
As the primary aim of the proposed research is to determine the feasibility of conducting a full-scale pragmatic RCT of CFT, a sample size calculation is not required. A sample size between 40 and 60 participants is recommended to achieve the key objectives of feasibility studies [45]. An upper limit of 60 participants has been chosen to provide adequate data to assess the clinical parameters including the standard deviation and confidence intervals of the primary outcome data to calculate the sample size for a future definitive trial, should feasibility be assured, whilst allowing for drop-outs.
Phase 2
Initially, a purposeful sample of eight to ten participants, enrolled in Phase 1, will be invited to discuss the acceptability of the research processes (e.g. study recruitment procedures, randomisation and outcome assessments) and their experiences of the intervention they received. To enhance variability and to limit selection bias, a purposive sample of responders and non-responders to the interventions (identified using a minimum clinically important change threshold of < 30% change in the Numeric Pain Rating Scale (NPRS) [60]) will be invited to participate. Data collection will continue until the research team is satisfied that data saturation has been reached.
Following completion of the intervention they will be contacted by the research team (CN) to determine participation in Phase 2. A second (Phase 2) participant information sheet will be provided. An appointment will then be arranged at a mutually convenient date, time and venue (their own home or physiotherapy department) for consent and the interview to be completed.
To determine the acceptability of the training package and participation in the RCT, all ten physiotherapists delivering the interventions in Phase 1 will be invited to participate in a focus group. Two focus groups will be held. Focus group 1 will contain the intervention (CFT) physiotherapists and focus group 2 the physiotherapists delivering usual physiotherapy care. The interviews and focus groups will be completed by the research team (a trained patient and public involvement (PPI) representative and (CN)) in the physiotherapy department.
Eligibility criteria
The study eligibility criteria are reported in Table 2.
Eligibility criteria
Eligibility criteria
Ten physiotherapists will be purposefully sampled to deliver the interventions based on a broad range of experience (NHS Band 5 to Band 7 clinicians). Attempts will be made to match the age, level of experience and job grade of physiotherapists between the two study arms. Five physiotherapists will complete CFT training in preparation for the RCT and to control for contamination between the study arms five different physiotherapists will provide usual physiotherapy care.
Cognitive functional therapy
A detailed description of the CFT intervention is provided in the supplementary file (Appendix 1) and has been reported elsewhere [33]. CFT will be delivered face-to-face by the trained physiotherapists. The Örebro Musculoskeletal Screening Questionnaire (short form) [61] followed by a comprehensive interview and a functional examination will inform the intervention.
Pain history and contextual factors (e.g. physical, cognitive, emotional, social, lifestyle and general health) at the time of onset to differentiate traumatic and non-traumatic causes. Mechanical and non-mechanical pain characteristics to determine stimulus-response relationships to postures, movements, activities and rest. Cognitions (e.g. beliefs regarding cause, future consequences, pain controllability) and emotional (e.g. fear, low mood, anxiety) responses to pain. Painful and feared valued functional activities will be identified, as well as behavioural responses to pain such as movement and activity avoidance. Social (e.g. work and home relationships) and cultural obstacles to adopting positive lifestyle and health behaviours. Lifestyle factors, such as physical activity levels, sleep hygiene, stress levels, diet and smoking. Personally relevant short and long-term goals will be identified. Past medical history to include, general health, vitality and co-morbidities and their relationship to pain.
Make sense of their pain from a biopsychosocial perspective using their own narrative and personal experience. Achieve pain control, where possible, through graduated exposure to feared, avoided and/or painful movements and valued activities. Adopt healthy lifestyle behaviours (e.g. increase physical activity levels, improve sleep, healthy diet and stress management) [33].
To facilitate behaviour change and develop therapeutic alliance, motivational interviewing and empathetic communication will underpin this process [62]. An individualised self-management program will be provided, monitored and evolved that includes progressive functional exercises and lifestyle modifications, where indicated [33]. The dosage and intensity of the exercise programme will be tailored towards an individual’s valued activities, goals, preferences and levels of physical conditioning, with the aim to coach people toward self-management of their condition. A personalised handout that outlines an individual’s vicious cycle of pain and web-based educational resources (www.pain-ed.com) that address common misconceptions about LBP, physical activity, sleep hygiene and the role of imaging will be provided where appropriate.The initial consultation will be for one hour and subsequent appointments for 30 minutes. Participants will be seen over three months and will typically receive between five to ten individual sessions of CFT, as determined by the participant’s confidence to effectively to self-manage their condition, through shared decision making with the physiotherapist [34–39]. At the end of the intervention, participants will be provided with a pain exacerbation plan to guide self-management in the event of an increase in LBP.
Cognitive functional therapy training
Training in CFT will be based on the core components of the examination and intervention developed and refined over the previous 20 years (49). Training will include attendance at a three-day clinical workshop, delivered by a CFT educator (PO). During the workshop, evidence regarding the multi-dimensional nature of persistent LBP and an introduction to the multi-dimensional clinical reasoning framework underpinning CFT will be provided. Demonstration of the key components of the CFT intervention will be exemplified during live observation of four patients with persistent LBP, during a masterclass by a CFT educator (PO). Website resources (www.pain-ed.com) and two electronic-books, detailing the multi-dimensional clinical reasoning framework and CFT intervention, with embedded clinician and patient videos, will be provided to each physiotherapist to support a period of experiential learning following the workshop. During this time each physiotherapist will complete video-recorded assessments of two new patients with persistent LBP to evaluate their progress in delivering CFT. Each video will be reviewed on a one-to-one basis with a clinical mentor (CN) and a bespoke action plan provided, including written and verbal feedback summarising key learning points. Peer support will include further clinical observations and case discussions between the physiotherapists and mentor during this period. Finally, an assessment of competency in the delivery CFT will be completed. Each physiotherapist will be observed by CN and PO whilst assessing and treating one new patient with persistent LBP within the clinicians own clinical environment. A pre-defined fidelity checklist covering the core components of the CFT examination and intervention will be used to determine physiotherapist competency to deliver the intervention (Appendix 2).
Usual physiotherapy care
Participants will receive usual physiotherapy care for LBP reflective of current practice and decision-making of physiotherapists managing LBP within the UK NHS [20, 63]. This will include psychosocial screening using the short form Örebro Musculoskeletal Screening Questionnaire [61].
Usual physiotherapy care training
In contrast to the CFT intervention, no additional skills will be required for the physiotherapists to deliver usual physiotherapy care, they will do so in line with their existing skillset and scope of practice. However, to reinforce existing knowledge and skills each physiotherapist will attend a three-hour teaching session comprised of lectures and practical demonstrations covering the contemporary physiotherapy assessment and management of LBP, aligned to UK clinical guidelines (self-management advice, psychosocial screening, manual therapy and exercise as a package of care) [20]. The teaching session will be delivered by a member of the research team (SO), who is an Associate Professor of Musculoskeletal Physiotherapy and has not received any formal training in CFT.
Assessment of treatment fidelity
Treatment fidelity will be monitored and evaluated during the intervention period in accordance with the behavioural change fidelity framework guidelines for treatment delivery [64]. Firstly, the physiotherapists’ clinical notes, for all participants, will be evaluated against the intervention checklists (Appendix 2) by CN to determine protocol adherence. Secondly, up to two video assessments (∼20%) will be competed at random for each physiotherapist, subject to informed patient consent. These videos will be analysed and assessed against the intervention checklists by CN (CFT group) and SO (usual physiotherapy care group) to ensure competency is maintained and that the interventions are being delivered as intended. Individual feedback will be provided on treatment delivery (e.g., intervention drift or protocol deviations). Fidelity of treatment delivery will be confirmed if > 80% of the intervention components are delivered as intended, as measured against the pre-defined checklists for both the clinical notes and video recordings [64]. Thirdly, the qualitative interviews and focus groups will explore treatment differentiation and integrity further.
Outcome assessments
Demographic data will be collected at baseline to include participant’s age, gender, duration of LBP and employment status. The chosen Patient Reported Outcome Measures (PROM’s) include measures of disability, pain intensity, quality of life and psychological function and have been used widely in previous LBP RCT’s, based on their strong psychometric profile and capacity to capture clinically important change [60]. The PROM’s were deemed to involve an acceptable burden by the PPI group. The PROM completion schedule is reported in the SPIRIT figure (Table 1) and a description for each PROM, including psychometric properties, is provided in Table 3.
Patient reported outcome measures
Patient reported outcome measures
Consenting participants will be randomly allocated to receive CFT or usual physiotherapy care. The randomisation order was generated using online software (www.randomization.com; accessed on 21st March 2019) and included blocks of variable size (block sizes 2, 4, 6, and 8). Group allocation will be concealed via sequentially numbered opaque envelopes, issued to the participants following baseline measurements and consent. Participants will take the sealed envelope to physiotherapy reception. The envelope will contain a colour coded card (blue for CFT, red for usual physiotherapy care) to indicate to the physiotherapy administrative staff which physiotherapist to book the initial physiotherapy appointment with. The researchers completing baseline and follow-up assessments will be blinded to treatment allocation throughout the trial. It is not possible to blind the physiotherapists.
Planned data analysis
Phase 1
Descriptive statistics for participant demographic data will be reported using means, standard deviations (or medians and interquartile ranges) for continuous variables and totals and proportions for categorical variables. The number of eligible and recruited participants will be recorded each week. Number of participants lost to follow-up at each data collection period will be reported and the reasons for drop out documented. Feasibility of the selected PROM’s will be assessed quantitatively by calculating the total time to complete, number of missing items, completion rates and qualitatively through the process evaluation in Phase 2. All data collection and analysis procedures will be completed by the lead author, CN.
Feasibility thresholds
The criteria for progression to continue to a future fully powered RCT include the following and are based on similar musculoskeletal feasibility RCT’s [65, 66]. 50% of screened referrals will meet the eligibility criteria. 50% recruitment rate into the study. 70% of participants are retained in the study at six-month follow-up. Intervention adherence by participants will be measured as greater than 80% attendance to the allocated intervention after randomisation. Less than 20% of data are missing on the returned patient PROM’s at each follow-up time. Less than 5% of participants report adverse events. All physiotherapists trained in CFT will be deemed competent to deliver CFT.
Phase 2
Qualitative data will be analysed using framework analysis [67]. Framework analysis shares the same analytical principles of thematic analysis but employs a systematic and visible approach to enhance methodological rigor [68]. Each interview will be played back several times to gain familiarity with the dialogue and then transcribed verbatim by CN. This will afford the opportunity to listen, reflect and re-examine the information [69]. Next, a coding framework will be formed for two transcripts based on patterns, threads, similarities, discrepancies and relationships that emerge through interpretation of the data. The first two transcripts will be coded blind by CN, the PPI representative, who will receive training in qualitative analysis, and VB who will then meet to discuss and reflect on their analyses of the data. Codes will be compared across the transcripts for coherence and pooled where patterns emerged to form an analytic framework. The analytic framework will be indexed against the remaining transcripts by CN. Data will be pooled and charted by case and code into a framework matrix. Cross comparison of codes within and between participants will be made and a final set of themes will be generated. Each theme will be discussed with the research team at a final meeting to confirm representation of the data.
Monitoring
As this is a feasibility study as part of the fulfilment for the lead authors’ (CN) Doctoral studies and that funding arrangements did not allow, no formal trial management or steering committee will be convened. Safety and study management will be monitored by the lead authors’ academic supervisory team at University of Nottingham during monthly supervision meetings, led by PL.
The dignity, rights, safety and well-being of participants and staff will be monitored and safeguarded in accordance with the sponsor’s, University Hospitals of Leicester NHS Trust, standard operating procedures. The risk of adverse events associated with physiotherapy are reported to be low in previous studies [70]. The health of participants will be monitored through attendance to physiotherapy and the study monitored by the research team at University of Nottingham. Should any adverse events occur, they will be documented and reported to the sponsor (University Hospitals of Leicester NHS Trust) in line with standard operating procedures and the appropriate action taken.
Patient and public involvement (PPI)
Three patient advisers, who have previously attended the host physiotherapy service with persistent LBP have informed the development of this research protocol. They assessed the suitability and practicality of PROM’s, which have informed the choice for the proposed study. One PPI representative will continue involvement in the study throughout. They will assist in developing the interview schedules for Phase 2, will receive training in qualitative data collection and thematic analysis in preparation to interview participants and contribute to the qualitative data analysis in Phase 2.
Discussion
This paper has presented the rationale, aims and methodological design of a mixed methods feasibility RCT that will compare CFT to usual physiotherapy care for people with persistent LBP attending a secondary care NHS physiotherapy service in the UK. A nested qualitative process evaluation aims to understand the acceptability of the research process and interventions to participants with LBP and their treating physiotherapists. The parameters that will determine feasibility have been described. The findings will inform the planning, design and completion of a future, definitive RCT that will compare the clinical and cost-effectiveness of CFT in the UK NHS, should feasibility be established.
The results of the feasibility RCT and qualitative process evaluation will be published open access in separate papers, once available, and abstracts submitted to national and international physiotherapy and LBP specific conferences.
Footnotes
Acknowledgments
The authors would like to acknowledge the study’s patient and public involvement group for their contributions towards designing this study.
Author contributions
CN, KOS and POS were responsible for the conception and design of the study. CN prepared the manuscript. VB, CD, SO, PL are co-investigators and contributed to the design of the study. All authors contributed to revising and editing the manuscript.
Conflict of interest
KOS and POS receive income from workshops promoting the biopsychosocial management of low back pain. All other authors have no conflict of interest to report.
Ethical considerations
Funding
This study is funded by the National Institute for Health Research (NIHR) Applied Research Collaboration East Midlands (ARC EM). The views expressed are those of the author(s) and not necessarily those of the NIHR or the Department of Health and Social Care.
This work was also supported by a Grant from the Chartered Society of Physiotherapy Charitable Trust (Grant number PRF/18/B18).