
Abstract
BACKGROUND:
There has been extensive literature examining the efficacy of exercise interventions in the treatment of depression over the past few decades. However, there is ongoing debate regarding the optimal dosage, and the implications of utilising physiotherapists for the management of clinically depressed adults using exercise has not been examined.
OBJECTIVES:
This review aimed to examine the effectiveness of exercise as a treatment for depression (without comorbidities) and to determine the most effective dosage/mode to treat this population. This review strived to appraise the literature for a potential role for physiotherapists in depression management.
METHODS:
Following the Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) protocol, a search for randomized controlled trials was conducted on the nine databases. All studies were appraised for quality using the Physiotherapy Evidence Database (PEDro) scale and Cochrane Risk of Bias Tool (RoB). Data was manually extracted, and pre- and post-intervention depression scores and program variables were analysed.
RESULTS:
Of the 5036 papers retrieved, 7 papers met this review’s inclusion criteria. The results of the meta-analysis reveal that exercise as a sole treatment and as an add-on is significantly effective in reducing depressive symptoms. The findings support the use of moderate intensity aerobic exercise for three sessions per week.
CONCLUSIONS:
Exercise was shown to significantly improve depressive symptoms in depressed adults. This review adds to the growing body of evidence regarding the important role of physiotherapists in the treatment of psychiatric disorders in the design and implementation of exercise interventions.
Introduction
Depression is characterised by incessant low mood, despondency and disinterest in activities previously enjoyed [1, 2]. At present, depression is the greatest contributor of disability and mortality [3], and the most prevalent psychiatric disorder globally [4]. In Ireland alone, at least 8% percent of the population present with moderate depression [5]. Moreover, up to 110.4 per 100,000 adults present to psychiatric services for the treatment of depression, of which 41.5% are first time admissions [6]. Yet, despite increased interest in depression management over the past three decades [7], by 2030 depression is still predicted to be the greatest contributor to the global disease burden [8].
The predominant treatment for depression over the past 30 years has been pharmacotherapy [9]. However, given the sustained pervasiveness of this disorder and the issues associated with antidepressant medication, research focused on examining alternative therapies is warranted [10]. Of these treatments, exercise-based interventions have elicited considerable examination in the past decade. Although several clinical guidelines recommend this modality as a potentially effective treatment for depression [11–14], pharmacotherapy remains the dominant therapy prescribed in Ireland and the UK [15, 16]. In Ireland, a minimum of 25% of patients attending GPs do so due to mental health problems. Yet, the level of onward referral to specialised therapies or programs is low (approx. 5%) [17].
Arguably, exercise is underutilised in depression care for two reasons. Firstly, the prescription of exercise requires collaboration between physicians/psychologists/psychiatrists and exercise specialists [18]. Despite the expertise of the physiotherapists and the potential value of the profession’s contribution to treatment deliverance [19], the role of the physiotherapy in mental health services remains negligible and poorly understood [20]. Although previous literature endeavouring to determine the most effective dosage [21], there is still ongoing debate regarding this aspect of the prescription process. Secondly, while several reviews have evaluated exercise as a treatment for depression, the efficacy of this modality varies. Reviews by Josefsson et al. [22] and Morres et al. [23] observed a significant antidepressant effect of exercise (–0.77, –0.79 respectively), whereas other reviews [24–26] noted only low to moderate efficacy (–0.62, –0.44, –0.61 respectively).
Previous published reviews have had several limitations. From the outset, they have either failed to isolate depression from confounding somatic and psychological comorbidities and/or lacked rigour in restricting their population to only those clinically diagnosed [22, 27–29]. Likewise, some systematic reviews are further undermined by the poor quality of the evidence they examined [22, 26]. Moreover, prior reviews have failed to identify and evaluate the practitioners involved in the prescription process. This further emphasises the significant gap in the evidence regarding the roles of professionals, particularly physiotherapists, in the implementation of exercise as a treatment.
Considering these shortcomings and the issues associated with the provision of this modality in healthcare, an updated review of the literature is warranted to determine whether exercise should become a dominant facet of depression management hereafter. From an Irish context, this is increasingly relevant considering a ‘National Exercise Referral Framework’ is currently in development across the country, which if successful will allow GPs to refer patients with chronic conditions (including depression) onwards for supported exercise interventions [30].
This systematic review aims to address these issues by assessing the efficacy of exercise as an antidepressant therapy using the following objectives: investigate the effectiveness of exercise in depressive symptom improvement in adults, when compared to a control, using a recognized outcome measure clarify the most effectual dosage/mode of exercise for maximal symptom remission evaluate the literature regarding the personnel involved in exercise prescription and determine the prospective role for physiotherapists in this process
Given the lack of reviews examining the effect of exercise on clinical depression in the absence of confounding factors, the current review will exclude studies including participants with co-morbidities (physical or psychological).
Methods
Literature identification
This systematic review followed the PRISMA protocol [31]. A search of randomized controlled trials (RCTs) written in English from January 1st, 1979 to June 30th, 2019 (40 years) was subsequently conducted by the principal author (MED) using the inclusion and exclusion criteria detailed in Table 1. This timeframe was chosen to maximise the number of studies included in this review, some of which may not have been highlighted in more recent systematic reviews in this field [23, 27]. To facilitate direct comparability between studies, the participant base was restricted to adults (age range 18–65 years). This step was undertaken given that both paediatric and geriatric participants with depression were highlighted to differ from the adult counterparts in the following ways: (1) depression symptomology, (2) responsiveness of depression to treatment and (3) adherence to interventions [26, 32–34],
Inclusion and Exclusion Criteria
Inclusion and Exclusion Criteria
Trials where exercise was not prescribed or involved non-traditional exercises were excluded on the basis that: (1) data regarding the effect of dosage could not be extracted, and/or (2) the possible confounding effects of the ‘mindfulness’ aspects of non-traditional exercise could not be removed. Additionally, multi-modal interventions were excluded as it was not possible to determine the individual effect of each component on depressive symptoms. Equally, all trials had to utilise a non-exercise control so the full effect of the intervention could be determined.
A search of the following databases was performed: CINAHL Complete, PubMed, PsycINFO, EMBASE, MEDLINE, psychARTICLES, CENTRAL (The Cochrane Central Register of Controlled Trials), Sports Discus and PEDro. The final search on these databases was completed at the beginning of August 2019. A sample of this search strategy, including the keywords used to refine the search is detailed in additional materials Figure S1. To ensure rigor, an independent reviewer independently implemented the search strategy, and the results were compared.
Study selection
The papers identified in the search strategy were recorded and collated on Microsoft Excel to facilitate the principle author (MED) to remove duplicates. All papers were screened following the PRISMA protocol. An independent reviewer implemented a review of a subset (10%) of the papers first identified through the search to confirm the studies selected by the principal author and consensus was reached.
Data extraction
The principal author completed data extraction independently. Depressive symptom scores measured on a validated outcome measure i.e. Hamilton Depression Rating Scale (HAM-D; [35]) were inputted into Excel and catalogued by study and grouping (i.e. control versus exercise intervention). Data regarding sample demographics, characteristics of the interventions, the outcome measures used and the personnel implementing the interventions were also recorded in Excel. Further to this, the principal author contacted several of the authors of included studies to seek missing data or further information. An independent reviewer independently screened 10% of the inputted data to ensure accuracy. The effect of the intervention on depressive symptoms relative to their controls were determined based upon the reported effect sizes (p-values). As with standard practice, a p-value≤0.05 was considered the cut-off for efficacy.
Methodological quality assessment
The studies were evaluated using the PEDro scale [36] and the RoB [37]. The principal author independently reviewed each trial using the criteria outlined in Table S1. An independent reviewer evaluated a subset (14%) of the studies and consensus was reached.
Both tools are considered robust measures of bias and have been shown to have good psychometric properties [36, 38] and moderately concurrent criteria [39]. As the main tool employed in physiotherapy research [40], the PEDro scale was utilised to facilitate dissemination. Per the RoB, all domains had to be satisfied for a study to be deemed to be of low risk of bias. Where criteria were not satisfied or only partially satisfied, the study was determined to have a high or unclear risk of bias respectively. On the PEDro scale, one point was awarded for each criterion met and the study was given a score out of ten. A study with a score of six points or greater was regarded as moderate to high quality [41].
Statistical analysis
The Cochrane Review Manager (RevMan Version 5.4) software was used to calculate the efficacy of exercise as an antidepressant. Post-intervention scores for both the intervention and control groups were pooled together based upon their intervention type. Given that the samples were expected to be heterogeneous and acknowledging the different measures employed across the trials, a random effects model which estimated standardised mean difference (SMD) and 95% confidence intervals (CIs) was used to determine treatment effect. Additionally, all studies were allocated a weighting factor relative to their sample size to account for their respective impacts of on the overall treatment effect i.e. larger sample equals higher weighting factor and larger effect. For trials where more than one exercise group was present or where more than one measure of depressive symptoms was used, the data was coded to identify the specific subgroup in the analysis.
Results
Study identification and selection
From the search strategy, over five thousand papers (n = 5036) were identified. Of these papers, seven trials met this review’s inclusion criteria. The process of inclusion is detailed in Fig. 1. Reasons for exclusion are further extrapolated in Figure S2.
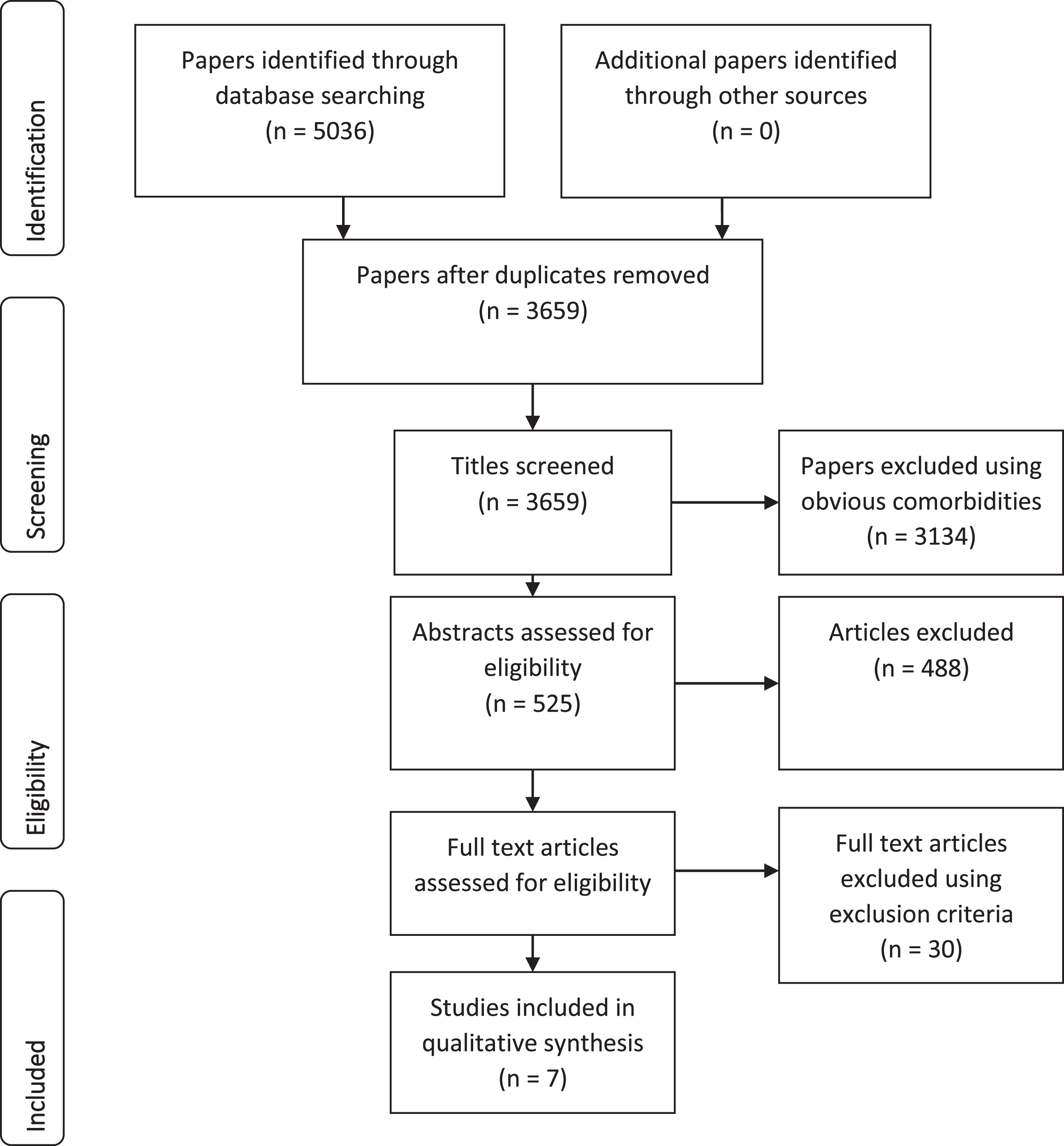
PRISMA Flow Diagram.
Table 2 shows the characteristics of the participants in the seven trials (n = 352). Of these trials, two were from Iran [42, 43]; two were from Brazil [44, 45]; two were from India [46, 47] and one was from the USA [48]. Two of the trials had three arms [33, 48]. Of these trials, one compared two exercise interventions (resistance exercise, aerobic exercise) to a waitlist control [48]. The other compared exercise intervention to cognitive therapy and a control [43]. Five of the trials had two arms, two of which compared exercise to usual care (antidepressants and/or electroconvulsive therapy) [44, 47], two compared exercise to antidepressants [45, 46] and one compared exercise to no treatment [42].
Participant Characteristics
Participant Characteristics
SD: Standard Deviation; % F: % Female; % M: % Male; AE: Aerobic Exercise Group; RE: Resistance Exercise Group; MDD: Major Depressive Disorder; MiDD: Minor Depressive Disorder.
Of the participants included, five trials recruited from clinical populations-inpatients and outpatients [44–48], while two of the trials recruited from non-clinical populations [42, 43]. All participants were diagnosed with depression via Structured Clinical Interview (SCID) using the Diagnostic and Statistical Manual of Mental Disorders (DSM-IV) and/or the International Statistical Classification of Diseases and Related Health Problems (ICD-10) criteria. In three trials, none of the participants received any pharmacological treatment [42, 43,48]. At least a portion of the participants in both arms of one trial were taking antidepressants [44], while in three of the trials all participants concurrently used antidepressants [45–47].
Interventions
All trials employed aerobic exercise in their interventions. Only Doyne et al. [48] compared both resistance-based and aerobic-based interventions to a control. All trials provided prescribed programs, the specific characteristics of which are detailed in Table 3. One trial allowed patients to choose between exercise at a preferred intensity with a stationary bike, treadmill or elliptical to achieve the prescribed dosage [44]. Two trials prescribed running [46, 48]. Three trials prescribed unspecified aerobic exercises for which patients were required to maintain intensity within a specific percentage max heart rate [42, 45]. One trial [48] prescribed a video assisted aerobic program, of which the exercises used were not specified. This trial used moderate to low intensity. However, this was not determined using an intensity-related measure. The duration of the interventions ranged from 10 days [47] to 24 weeks [46]. Two trials did not have a set length for the intervention, as it was determined based upon a desired number of sessions [42] or the duration of a patient’s hospitalization [44].
Intervention Characteristics
Intervention Characteristics
AE: Aerobic Exercise; RE: Resistance Exercise; Max HR: Maximum Heart Rate; NR: Not Reported.
The studies used various measures for depressive symptom severity. Five used the Hamilton Rating Scale for Depression (HAM-D) [44–48]. Four used the Beck Depression Inventory (BDI-II) [42, 48]. Additional measures used included the following: The Depression Adjective Check Lists Form A (DACL; [48]), the Visual Analogue Mood Scale (VAMS; [47]), the Depression Somatic Symptom Scale (DSSS; [47]), the Automatic Thoughts Questionnaire (ATQ), and the Dysfunctional Attitudes Scale (DAS; [42, 43]). Only two studies measured depressive symptoms during the intervention [46, 48] and only one study [48] presented data for follow-up at specific intervals post-intervention (1-month, 7-months and 12-months). The pre- and post-intervention scores for all trials are detailed in full in Tables S2-S3.
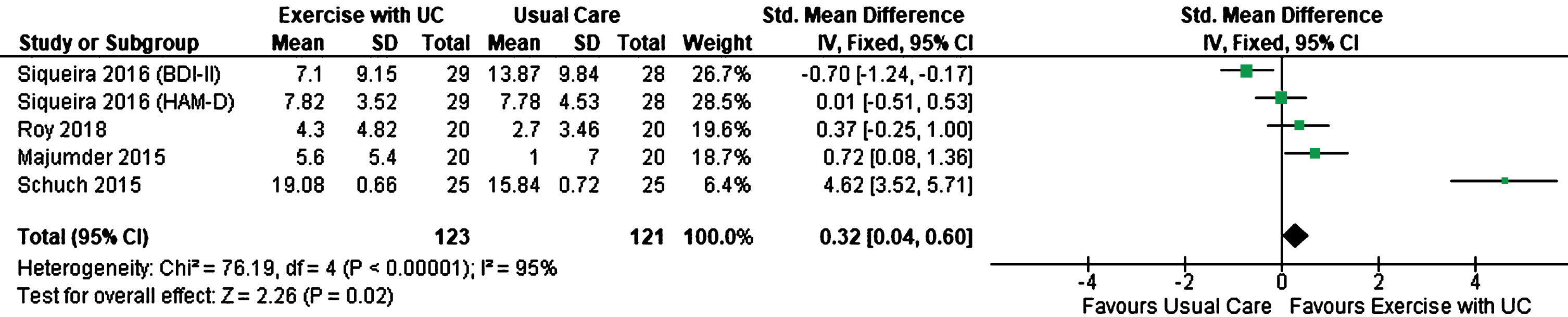
Meta-Analysis of depressive symptom score ‘Intervention 1: Exercise with Usual Care vs Usual Care’.
Details of the quality assessment on both the PEDro scale and the RoB are provided in Figures S3-S4 and Tables S4-S5. On the ten-point PEDro scale, two out of the seven trials were determined to be of high quality [44, 45]. The remaining studies scored five on the scale. Only one trial [41] specified concealed allocation. Four trials blinded their assessors [43–45, 48]. Though given the nature of the treatment, it was not possible for either the therapists or participants to be blinded in any of the studies. Five trials [42–44, 47] were determined to have a low risk of attrition bias.
Meta-analysis
Of the seven included trials, four trials compared exercise with antidepressants to usual care (‘Intervention 1’) [44–47] while three compared exercise (as the sole treatment) to unconventional/ no care (‘Intervention 2’) [42, 48]. Across both intervention groups, two main outcome measures were used to record depressive symptom severity: the HAM-D [44–48] and the BDI-II [42, 48]. For ‘Intervention 1’, five subgroups were pooled (n = 254), with post-intervention scores for one trial [45] on both outcome measures being recorded. For ‘Intervention 2’, six subgroups were also pooled (n = 215), allowing for the inclusion of two different exercise groups (AE and RE) scores on both measures for one trial [48].
The pooled results indicate that post-intervention there was a significant antidepressant effect associated with exercise (when used solely and as an add-on) when compared to both usual and unconventional care. Notably, the treatment effect was greater in studies included in the ‘Intervention 2’ group (REM, STD 1.29, 95% CI 0.86 to 1.72, p < 0.00001) compared to the ‘Intervention 1’ group (REM, STD 0.32, 95% CI 0.04 to 0.60, p = 0.02) as outlined in Figs. 3.6 and 3.7. However, for ‘Intervention 1’ there was significant heterogeneity observed (I2 > 75%).
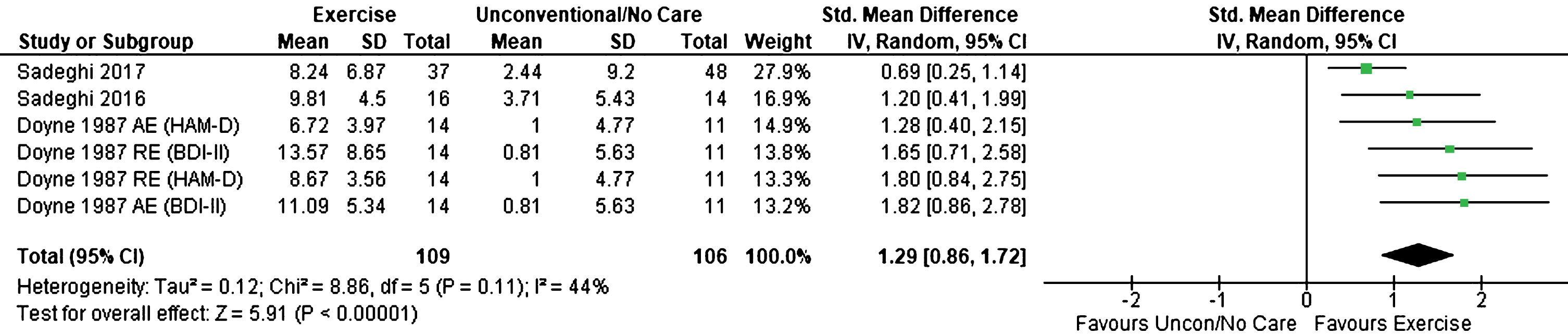
Meta-Analysis of depressive symptom score ‘Intervention 2: Exercise vs Unconventional/No Care’.
Intervention 1: Exercise with usual care versus usual care (anti-depressants and/or ECT)
Four trials compared exercise with usual care [44–47]. Of these trials, all four measured depressive symptoms pre- and post-intervention, with only one trial [46] measuring depression during the intervention. Siqueira et al. [45] used the BDI-II scale, while Roy et al. [47] employed the VAMS and DSSS measures. No trial conducted follow-up assessments beyond post-intervention. One trial [46] investigated the efficacy of exercise and antidepressants following 4 weeks of pharmacotherapy. In this trial, remission (HAM-D score < 16) was achieved using anti-depressants. It aimed to examine the efficacy of combined exercise and pharmacotherapy in the prevention of relapse or continued improvement of depressive symptoms. Although, there was greater and statistically significant improvements in depressive symptoms for the intervention group, this did not transfer into a significant difference in relapse rates (p = 0.07). Schuch et al. [44] also compared the difference in remission rates between groups at the discharge of the participants from hospital and found that the difference was not statistically significant.
On the HAM-D, three trials [44, 47] involved intervention groups whose depressive symptoms significantly improved. Of these trials, the depression severity varied from mild to severe (mainly severe), with the majority of the participants receiving pharmacotherapy (usual care). Though, only Roy et al. [47] retained all participants. Majumder et al. [46] and Schuch et al. [44] lost 12% and 8% of their intervention groups respectively. Siqueira et al. [45] studied adults with major depressive disorder, 31% of which dropped out. Although, the intervention group’s depressive symptoms significantly improved, on both the HAM-D and BDI-II this effect was not statistically significant when compared to the pharmacotherapy control. Roy et al. [47] reported significantly improvements in both objective mood (VAMS: p < 0.001) and somatic symptoms (DSSS: p < 0.01) in the intervention group.
Intervention 2: Exercise versus no treatment or unconventional care
Three trials compared exercise (without pharmacotherapy) to either no treatment [42], a waitlist control [48] or to the effect of a single facilitated group discussion [43]. Of these trials only Doyne et al. [48] used the HAM-D, while all three trials used BDI-II. Sadeghi et al. [42, 43] also used the ATQ and DAS, while Doyne et al. [48] utilized the DACL. Only Doyne et al. [48] measured depressive symptoms during the intervention and at four intervals post-intervention.
On the BDI-II, all trials [42, 48] showed statistically significant symptom improvement. These improvements were maintained long-term in the Doyne et al. [48] trial (both HAM-D and BDI-II p-values < 0.01). The significant changes (p < 0.05) shown regarding the use of positive and negative adjectives (DACL) in this trial were maintained at follow-up. In Sadeghi et al. [42, 43] the improvement in negative thoughts and dysfunctional beliefs (on the ATQ and DAS) were not statistically significant post-intervention.
The results of this review indicate that exercise with or without pharmacotherapy is effective in reducing depressive symptoms and potentially has a positive impact on other factors associated with depression (i.e. mood, somatic symptoms, depressive adjective usage). Although one trial’s intervention [45] did not reach significance regarding antidepressant efficacy (HAM-D p-value = 0.16; BDI-II: p-value = < 0.82), the intervention’s participants did require a lower dose of antidepressants following treatment. Similar results were observed by Schuch et al. [44]. Equally, one study [46] noted a greater effect of exercise on maintenance of remission rates for patients up their discharge from hospital.
Effective dosage
Only two trials [44, 45] outlined all intervention characteristics. Three trials [42, 45] used both interval and continuous training modes, while Doyne et al. [48] used only interval training and Majumder et al. [46] prescribed continuous exercise. Six trials reported training frequency: two prescribed daily exercise [46, 47], two had four sessions/week [45, 48] and two had 3 sessions/week [42, 44]. All trials reported levels of intensity. However, intensity measures were not consistently used across the trials; four trials prescribed moderate to vigorous intensity exercise [42, 46] one trial prescribed only vigorous aerobic exercise [48], while others prescribed moderate activity [44] or low to moderate activity [47]. One trial did not report a session duration and only one [47] reported participants exercising in a group-setting. Schuch et al. [44] and Siqueira et al. [45] had participants exercise individually. All trials were supervised to an extent.
Despite the variability of the interventions, only one study [45] did not show a significant improvement in depression. This trial had high attrition rates in both the intervention (31%) and control (28.5%) groups. The trials [42, 44] with three sessions/week showed the most significant improvement in depressive symptoms. While these scores were recorded on the two different measures (BDI-II and HAM-D respectively), given the low level of attrition from these studies (≤8%) these results potentially highlight an effective frequency dosage. The trials also indicate that in a clinical population moderate intensity may be the most effective. Schuch et al. [44] only used moderate intensity exercise and showed the greatest significance in results (p = 0.005), while the trial that utilised only vigorous aerobic exercise had an attrition rate of 40% [48]. The Doyne et al. [48] study indicates that resistance and aerobic exercise are equally effective antidepressant modalities. However, this was the only trial to investigate this comparison. Due to inadequacy and variance in reporting, the results of the seven trials do not highlight any other characteristics which contribute to increased efficacy.
Intervention personnel
None of the seven trials involved physiotherapists in the design or implementation of the interventions. Two trials [44, 46] were administered by their researchers. For two trials [42, 43] supervision was provided by a sport expert. One study [46] was supervised by a nurse, while another [48] was supervised by university students (of unknown discipline) who were provided training to monitor the exercise sessions.
Discussion
Summary of principle findings
Findings from this systematic review and meta-analysis indicate that exercise may be an effective antidepressant therapy for adults with clinical depression. The meta-analysis indicated that exercise appears strongly effective in improving depressive symptoms, both as an add-on therapy and as a sole therapy in inpatient and outpatient cohorts. Greater significance in depressive symptom improvement was demonstrated in the meta-analysis for ‘Intervention 2’ (exercise as a sole treatment). However, when the participants’ depression type in the intervention groups are compared, the severity of depression is greater for ‘Intervention 1’ participants. This difference could be a potential confounding factor with respect to the greater significance of ‘Intervention 2’ efficacy.
One trial conducted follow-up measurements in addition to post-intervention scoring and reported that improvements in symptoms were maintained 12 months post-intervention. Two trials also indicated that exercise could potentially reduce antidepressant dosage, while one trial showed a positive correlation between exercise and decreased relapse rates. Regarding effective dosage, the results of this review highlight that three sessions/week at moderate intensity (60–75% HRmax) may be optimum. Based on one trial, aerobic and resistance exercise were noted to be equally effective. The narrative review highlighted that a mixture of personnel was involved in the design and implementation of the interventions. However, physiotherapy input was absent.
Results in the context of current literature
The results of this review indicated several important factors related to the potential effects of exercise on depression. Despite mixed evidence [24, 27], this review contributes to the growing body of literature supporting exercise’s effectiveness as an antidepressant therapy [7, 23]. Though only one study [48] measured and demonstrated the significant long-term efficacy of exercise on depression, these findings align with previous research which identified exercise as a protective factor against the reoccurrence of depressive episodes in depressed adults who remained active [49, 50]. However, the evidence regarding this efficacy aspect is limited and the consistency of exercise’s effectiveness beyond intervention is debatable [51].
Though, one trial in this review highlighted a potential positive association between exercise and relapse prevention [46], the evidence regarding this correlation is mixed. While exercise has been shown to improve probability of remission by up to 22%, the significance of this effect was not evident in trials with higher methodological quality [18, 27]. Two trials [44, 45] observed decreased antidepressant usage by its participants following the intervention. These results indicate that exercise could potentially reduce patients’ dependence upon pharmacotherapy, as noted in previous literature [52].
This review concurrently examined the effect of exercise on other depressive factors (i.e. thoughts, negative mood, etc.), which have been correlated with depression severity [53–56]. Although, one study [48] showed statistically significant changes in use of negative adjectives, this did not translate into significant improvements in depressive thoughts or beliefs [42, 43]. The improvement, but lack of significance, in negative thoughts/beliefs may correlate to the diversionary nature of the intervention. However, in absence of specific cognitive therapy to challenge underlying beliefs, significant modification of thought processes is not feasible [42, 57].
One study [47] did show that exercise had a greater impact on mood and somatic symptoms compared to antidepressants, which aligns with research by Krogh et al. [58, 59]. Meyer et al. [60] suggest that these changes relate to the potential impact of exercise on brain-derived neurotropic factor (BDNF) serum levels. This neurotrophin has been identified as a key factor in neuronal circuits maintenance, including those involved in emotional control and is notably reduced in the presence of depressive disorders, resulting in a depressed mood [61]. Although previous research could not determine any dose-response in acute interventions, it is possible that dosage (specifically intervention length or intensity) could have impacted the efficacy of exercise on these symptoms [18, 62–64].
This review aimed to determine the most effective dosage of exercise. However, in line with the findings of Stanton and Reaburn [21], the insufficiency of data reported by trials and the heterogeneous nature of the program principles proved to be a limiting factor. However, this review indicated that, similar to previous research and guidelines in this area, three sessions/week of moderate intensity aerobic exercise appears optimum [21, 66]. Due to high variation across the studies this review did not identify a specific dosage for intervention or session durations. Previous literature [21, 66] recommends on average thirty-minute sessions for at least nine weeks. However, in view of satisfying the recommended physical activity guidelines for adults (i.e. minimum of 150 mins/week of moderate intensity aerobic activity [67, 68]), a progression to 3x50-minute sessions is required. Given that all trials in this review utilized at least some supervision and were mainly aerobic, the findings do not reflect the efficacy of the reverse modes. Though, for maximal adherence, supervised (either aerobic or resistance) group exercise is recommended [66, 70].
Intervention adherence is important to consider, as adults with depression are a greater risk for non-compliance [71, 72] and are more likely to be sedentary [18, 74]. Hence, while higher exercise dosage may result in greater efficacy [75, 76], there is a strong likelihood of it equally contributing to increased attrition and thus, minimizing longer-term adherence or potential benefits. For instance, in the Doyne et al. trial [48] the high intensity (80% HRMax), high volume (x4 sessions per week) exercise prescribed to the AE group resulted in a 40% drop-out rate. Notably, research suggests that motivational interventions could be employed alongside exercise to help elicit greater adherence and long-term behaviour change [71, 77].
Regarding intervention personnel, this review noted mixed involvement of both researchers and reported ‘exercise specialists’. Across all studies, minimal information was provided on the expertise of these practitioners. Despite the proficiency of physiotherapists in exercise prescription, they were absent from the reviewed studies.
Though this review examined exercise in the adults with depression without comorbidities, exercise has been shown to be effective on depression in adults with other conditions [78]. In practice, physiotherapists already manage clients with multi-morbidities through exercise prescription [79–81]. Therefore to facilitate the expansion of physiotherapy’s scope into mental health, future research should involve physiotherapists in the design and implementation of programmes. Current research suggests that physiotherapists’ involvement could contribute to decreased attrition and superior outcomes [82, 83]. Hence, from an MDT perspective the onward referral of clients with depression (recommended by the ‘National Exercise Referral Framework’) should be facilitated towards physiotherapists for specialized exercise program design and implementation.
Limitations
There are four main limitations of this review. Firstly, only a small number of studies were included in this review, as commonly observed in previous reviews [23]. However, this was the first systematic review to rigorously require a clinical diagnosis of depression and exclude trials with participants with comorbidities, including anxiety. These criteria further restricted the number of relevant studies.
Secondly, the heterogeneity of the trials sampled was high for ‘Intervention 1’ (I2 = 95%). Given that this heterogeneity was expected due to the variable use of the BDI-II and HAM-D and the varying characteristics of participants sampled across the trials, a random effects (RE) model had to be utilized in the meta-analysis. Therefore, there is an underlying assumption that the ‘true effect’ of exercise as an anti-depressant varies from study to study and the overall effect determined is an estimation of the distribution’s mean. Though in the case of the trials sampled, the ‘summary effect’ of both intervention types were similarly significant when both the RE and fixed effect (FE) models were used, the small sample sizes of the included trials highlights the other shortcoming of this meta-analysis. In that, the efficacy of exercise is greater in smaller studies and possibly skews the estimate of ‘true effect’ due to the absence of larger, potentially more methodically rigorous studies.
Thirdly, the type of participants recruited in the trials was skewed in favour of younger (average age: 32.31) female (average: 62% female) adults. However, research suggests that depression rates are greater in women [84] and in recent years the prevalence has increased in young adults [85], thus potentially contributing to this sample’s skew. Finally, all trials were determined to have methodological issues: four trials with a high risk of selection bias and one trial with a high risk of detection and attrition bias on the RoB. Inadequate design description in terms of randomisation, blinding and reporting also contributed to unclear risk of bias in all studies. Additionally, convenience in participant recruitment contributed to the bias of some trials [42, 43] and could possibly have skewed uptake and retention rates, possibly enhancing intervention efficacy. Overall, only one of the trials was deemed high quality on the PEDro scale, with the other six being of moderate quality. Given that participants partook in an exercise-based treatment blinding was not feasible. Hence, from the outset, the quality of the included papers was always going to be limited by this factor.
Previous reviews [7, 86] reported similar issues with methodological quality, highlighting the lack of high quality RCTs available investigating exercise efficacy in treating depression. Although Morres et al. [23] found that the level of bias did not impact the significance of the results, previous reviews [24, 86] observed that the efficacy of exercise was lower in higher quality trials. Hence, the relative significance of the results identified in this review should be cautiously considered.
Areas for future research
Given the lack of available literature and the heterogeneity in design of available RCTs, further research is warranted in this field. Future RCTs should address the following topics: (1) effectiveness of exercise as a monotherapy versus as an adjunctive therapy in clinical depression, (2) efficacy of exercise in adults with pharmacotherapy resistance or in remission, (3) controlled investigation of the effects of different program variables including varying intervention lengths, levels of supervision, comparison between inexperienced and experienced exercisers and comparing efficacy between preferred versus prescribed exercise. Regarding these latter variables, future research could employ Sequential Multiple Assignment Randomized Trial (SMART) design to individualize programs to client preference, for potential long-term adherence and benefits. Additionally, future literature should explore the effect of exercise on antidepressant dosage and relapse rates.
Conclusions
Based upon this review’s results, exercise was deemed to be an effective antidepressant therapy across various severities of depression and in varying settings. This review highlighted that three sessions/week of moderate intensity aerobic exercise is effective. Finally, considering the mounting evidence in favour of exercise in the treatment of depression, physiotherapy involvement in the multidisciplinary team management of this condition is more than warranted.
Footnotes
Acknowledgments
We would like acknowledge Dr Felipe Schuch and Dr Amrita Roy for their time and correspondences.