
Abstract
BACKGROUND:
Lung transplantation (LTx) is an established treatment option for patients with end-stage lung diseases. Nevertheless, exercise intolerance, respiratory muscle function impairment, functional disability, and peripheral muscle weakness often persist following LTx.
PURPOSE:
To examine the effectiveness of a pulmonary rehabilitation (PR) program and home-based inspiratory muscle training (IMT) alone or in combination, in post lung transplantation (LTx) patients.
METHODS:
In a prospective pilot study a sample of 22 patients who had undergone LTx 4–18 months prior, were randomized to groups of PR alone, or combined with home-based IMT, or IMT alone, for six months: four months in the intervention program and two months of follow-up. Inspiratory muscle strength was assessed by measuring the maximal inspiratory pressure (MIP).
RESULTS:
There was a statistically significant increase in MIP values as well as in the 6-min-walk-test, only in the PR combined with home-based IMT, and IMT exercise groups. From baseline after 2- and 4-months intervention and at 6-months at follow-up, there was a statistically significant correlation between MIP and Maximum Voluntary Ventilation (MVV) values.
CONCLUSIONS:
Pulmonary rehabilitation (PR) program combined with inspiratory muscle training (IMT) or home-based IMT alone, in post lung transplantation patients, seems to be the best exercise combination for achieving the optimal effect, in inspiratory muscle strength and exercise capacity, with evidence for long-term benefits. Patients should be encouraged to participate in a PR program that includes home-based IMT exercise, especially in times of restricted mobility, as currently due to the COVID-19 pandemic.
Keywords
Introduction
Lung transplantation (LTx) is currently an established treatment option for patients with a wide variety of end-stage lung diseases [1–3]. Nevertheless, exercise intolerance, functional disability, and peripheral muscle weakness often persist following LTx [4–6]. Moreover, prior studies illustrated respiratory muscle function impairment in patients who had undergone LTx [7, 8].
Pulmonary rehabilitation (PR) is an evidence-based standard, which is widely recognized as an important component of care for patients with chronic obstructive pulmonary disease (COPD), idiopathic pulmonary fibrosis (IPF) and interstitial lung disease (ILD), as a means to improve dyspnea, exercise tolerance, and quality of life, while reducing health care resource utilization [9–15]. The goal of PR following LTx is to enhance the physiological and functional benefits following the surgery [4, 14–17].
One approach that has the potential to increase function of the respiratory muscles is inspiratory muscle training (IMT). The inspiratory muscles, including the diaphragm, are morphologically and functionally skeletal muscles and therefore should respond to exercise in the same way as any striated muscle. The rationale behind the application of IMT is that weak respiratory muscles, is expressed in patient’s dyspnea and low exercise tolerance, thus ameliorating the inspiratory muscle weakness should reduce the level of dyspnea, as well as increase the level of exercise tolerance [18, 19]
A systematic review, by Geddes et al. (2008) determined the effect of IMT was in significant increases in inspiratory muscle strength and endurance, improvements in exercise capacity and health related quality of life (HRQoL) and decreases in dyspnea in adults with stable COPD [18]. A study by Magadle et al. (2007) determined IMT provides additional benefits to the exercise of COPD patients already involved in a long-term PR program, as a general exercise reconditioning program [20]. Indeed, many lung transplant centers require recipients to attend an outpatient rehabilitation program [15, 21]. Despite their widespread implementation, only a limited number of studies have described or evaluated PR programs following LTx.
Therefore, the aim of the present pilot study was to evaluate the contribution of PR and IMT treatment programs, examined together as well as separately, to assess their unique and combined effect on LTx patients’ short- and long-term recovery.
Methods
Participants
Twenty-two patients, 12 male and 10 females, who had undergone lung transplantation 4–18 months prior to the pilot study were recruited from the database of post lung transplant patients or at the outpatient clinic of the Pulmonary Institute, Rabin Medical Center, Beilinson Hospital, Petach Tikva, Israel. The patients were all new to an IMT program, and none were receiving additional regular exercise.
Inclusion criteria: included patients were (i) at least four months post-LTx; (ii) able to perform pulmonary function tests; (iii) clinically stable for at least one month.
Patients were excluded if they had (i) unstable cardiovascular disease; (ii) required supplemental oxygen; (iii) cor pulmonale; (iv) poor compliance.
Study design
The patients participated in the pilot study for six months: four months in an intervention program and two months of follow-up. Randomization was performed using a random – number table, concealed in opaque envelopes and prepared by an investigator not directly involved in the pilot study. The patients were randomized into four groups: Six patients were assigned to receive PR, 6 to receive PR combined with IMT, 5 to receive IMT alone, and 5 to receive IMT sham, (as a control group). In all patients, several practice tests were performed before taking baseline values in order to correct for a possible exercise and learning effect. All tests were recorded at baseline before exercises, and at 2, 4 and 6 months after starting the exercises, except for VO2 peak which was tested at baseline and 4 months after starting the exercises. All data were collected by the same investigator, who was blinded to the training group. The information about primary care consultation and hospitalization were self – reported by the patients and/or family members during the daily call of the physiotherapist. The pilot study protocol was approved by the institutional ethics committee. The pilot study complied with the principles of the Declaration of Helsinki, and informed consent was obtained from all subjects. The protocol was registered with Clinical Trails.gov (NCT01162148).
Measures
Spirometry test
A physiological test that measures lung expiratory and inspiratory volume and flow of air during one breath cycle. Forced vital capacity (FVC), forced Expiratory Volume in 1 second (FEV1) and maximum Voluntary Ventilation (MVV) were measured three times on a computerized spirometer according to standard techniques and American Thoracic Society/European Respiratory Society (ATS/ERS) guidelines (Zan 530: Oberthulba, Wurzburg, Germany) [22]. The measured FEV1 and FVC are normalized by the predicted FEV1 and FVC values, which depends on the patient’s age, height, gender and ethnicity, and hence referred to as percent predicted FEV1 (% FEV1). All the measured parameters were presented as the percent of predicted (% pred) values of the European Community for coal and Steel [23]. MVV was presented as L/min.
Cardiopulmonary exercise test (VO2 peak Test)
The cardiopulmonary exercise test (CPET) was performed according to established guidelines [24, 25]. All tests were supervised by a physician. Patients were instructed to take their usual medications, as prescribed. A 10–15 W/min ramp protocol was performed on an electromagnetically braked cycle ergometer (Ergoline -800S) to the patient’s maximal subjective exertion level and respiratory exchange ratio (RER≥1.1) [24]. During the tests, 12-lead electrocardiogram, blood pressure, pulse oximetry (SpO2) and breath-by-breath respiratory gas exchange were recorded and monitored (Zan 600, Oberthulba). All peak cardiopulmonary data were calculated and the analysis was based on the average of the last 30 s of the test. The anaerobic threshold was determined by the dual methods approach, using the V-slop method combining ventilatory equivalents (VE/VO2 and VE/VCO2). Predicted values of peak oxygen consumption (VO2 peak) were determined according to Jones et al. (1985), based on prospective data of 100 subjects (50 males and 50 females) from the general population aged 15–71 years [26].
Six-minute walk test
The six-minute walk test (6MWT) test was set according to ATS guidelines [27]. The distance the patient was able to walk in 6 min was determined in a measured 35-meter corridor at the pulmonary unit within the hospital. The patients were instructed to walk at their fastest pace and cover the longest possible distance in 6 min under the supervision of a physiotherapist. The test was performed twice, and the best result was recorded.
Inspiratory muscle strength
Inspiratory muscle strength was assessed by measuring the maximal inspiratory pressure (MIP) at residual volume, using the technique proposed by Black and Hyatt, (1969) [28]. Mouth pressures were measured by an electronic pressure transducer (MicroRPM; Micromedical, Kent, UK). Assessments were repeated at least three times (30 s recovery between attempts), and the value obtained from the best effort was recorded.
Procedure
An experienced senior physiotherapist monitored participation in the PR program and supervised the exercise classes.
Pulmonary Rehabilitation (PR) exercise training program (with or without IMT)
Participants who were randomized to either PR group, or to PR combined with IMT group received an exercise program consisting of the three main PR components:
(a) Endurance exercises; (b) Strength exercises; and (c) Stretch exercises.
The PR program was continued for 16 weeks, twice-weekly with 60-min group exercise sessions in our rehabilitation center at the Pulmonary Institute. The exercise program followed exercise guidelines prescribed for patients with chronic lung disease [9–12], and were instructed by a physiotherapist and supervised by a nurse and the pilot study physician. During all exercise sessions patients were monitored for blood pressure, SpO2, heart rate and symptoms.
*Two patients with orthopedic problems (one from the PR group and one from the PR combined with IMT group) practiced interval exercises on stationary cycling bike. The program began with bouts of 5 min, followed by 1 min of passive rest (interval), for 5 repetitions (5 min bout +1 min rest, repeated 5 times). The progression of the exercise program included adding 1 min to the duration of each bout in each session, until reaching 15 min of continuous exercise, thus maintaining the time frame of 30 min of aerobic activity.
Inspiratory Muscle Training (IMT) home-based program
Participants in the PR combined with IMT, in the IMT-only group, and in the IMT-sham group received resistive or very low resistance load (for the sham control group) IMT home-based exercise. All patients were given instructions for self-management of the Powerbreathe inspiratory muscle trainer at baseline assessment.
Powerbreathe is an inexpensive inspiratory muscle trainer, whose efficacy has been supported by previous studies [29–31]. Powerbreathe® is one of the existing linear load resistor models on the market, which generates resistance via a spring-loaded system or an electronic valve. The basic difference between this tool and the others is its ability to offer the largest load during the therapy, and to adapt inspiratory resistance to the pressure x lung volume curve [32], which could generate load stabilization along the breath this concept has a physiological basis.
Participants in the PR combined with IMT group and the IMT-only group were instructed to practice home-based IMT daily, six times a week (a 15-minute session twice a day), for a period of four months. The exercise was performed using the Powerbreathe trainer. The participants started breathing at a resistance that required the generation of 15% of their maximal inspiratory mouth pressure (MIP) for an adaptation period of one week. The load was then increased incrementally for each participant, at a rate of 5–10% each session, to reach a generation of 60% of their MIP by the end of the first month. IMT was then continued at 60% of their MIP and adjusted monthly to the newly achieved MIP. Participants in the IMT-sham group were instructed to apply the same exercise protocol as described above, but with a fixed load that required the generation of a mouth pressure of 7 cm H2O, which is too low to generate any therapeutic effect.
To verify, and as a reminder to perform daily home-based IMT, the main investigator contacted each participant by phone, three times a week, during the four-month period. Thus, also providing opportunity to answer questions regarding use of their IMT trainer. This is an accepted strategy for controlling clinician contact in clinical trials involving disabled patients with chronic lung disease [33].
Data analysis
All clinical and physiological parameters were presented as mean±standard deviation (SD). Patients baseline characteristics, all primary and secondary parameters, changes (delta) from baseline to post-intervention at each measurement time point were compared.
A nonparametric statistical method was applied because of the small number of participants in our pilot study. Kruskal-Wallis test was used to compare changes between three groups, while the Wilcoxon test was used to compare pairs of two groups. The correlations between MIP to MVV values, 6MWT and VO2 peak, were calculated at each time point for all three intervention groups using the Spearman Correlation Coefficient Test. The alpha level was set to 0.05 and the power to 80%.
Results
Baseline clinical characteristics of exercise groups are summarized in Table 1. There were no significant differences between the three groups (PR, PR combined with IMT and IMT alone) in age, height, weight, mean baseline FEV1, FVC, MVV, MIP, VO2 peak, 6MWT, and prior hospital admissions (Tables 1 and 2)
Baseline Clinical and Demographic Characteristics of groups
Baseline Clinical and Demographic Characteristics of groups
Abbreviations: CF, cystic fibrosis; BMI, body mass index; DLT, double lung transplantation, SLT, single lung transplantation. Data presented as means and standard deviations at the following measures: Age, Time from transplantation, BMI, Weight, and Height. All other measures are presented as frequencies.
Baseline (T0) Results of Respiratory Muscle Strength and of 6-Minute Walk Test by Group
Abbreviations: PR, pulmonary rehabilitation group; PR + IMT, pulmonary rehabilitation combined with inspiratory muscle training group; IMT, inspiratory muscle training group; T0, baseline; 6MWT, 6-minute walk test; MIP, maximal inspiratory pressure; MEP, maximal expiratory pressure. Data presented as means and standard deviations.
Notably, only measurement results of PR combined with IMT, IMT alone, and PR alone groups were compared; the statistical analysis excluded the IMT-sham group due to drop-out of 3 of its 5 members.
No adverse events were observed during either the PR or the IMT in any of the exercise groups. The participants did not practice any other exercises or sports activity at home while participating in the pilot study and none of the participants was hospitalized.
There was no statistically significant change in FEV1, FVC, MVV and VO2 peak in the exercise groups (PR, PR combined with IMT and IMT).
Inspiratory muscle strength
A statistically significant increase in MIP values was evident from baseline after 2- and 4-months (19.1±27.8 and 37.8±22, p < 0.01) intervention and at 6-months (8.3±26, p = 0.02) at follow-up, in the PR combined with IMT exercise group, and in the IMT only (21.2±12.6 and 31.8±14.6, p < 0.01; 10.4±15.2 p = 0.02) exercise group, but not in the PR group (Table 3 and Fig. 1).
Intergroup Differences in the Extent-of-Change in Maximal Inspiratory Pressure (MIP), at t1 =ΔT1-T0, t2 =ΔT2-T0, t3 =ΔT3-T0
Intergroup Differences in the Extent-of-Change in Maximal Inspiratory Pressure (MIP), at t1 =ΔT1-T0, t2 =ΔT2-T0, t3 =ΔT3-T0
Abbreviations: PR, pulmonary rehabilitation group; PR + IMT, pulmonary rehabilitation combined with inspiratory muscle training group; IMT, inspiratory muscle training group; T0, baseline; T1, after 2 months of intervention; T2, after 4 months of intervention; T3, 6 months after T0; MIP, maximal inspiratory pressure. Data presented as means and standard deviations. Significant differences between the groups: *p < 0.05, **p < 0.01.
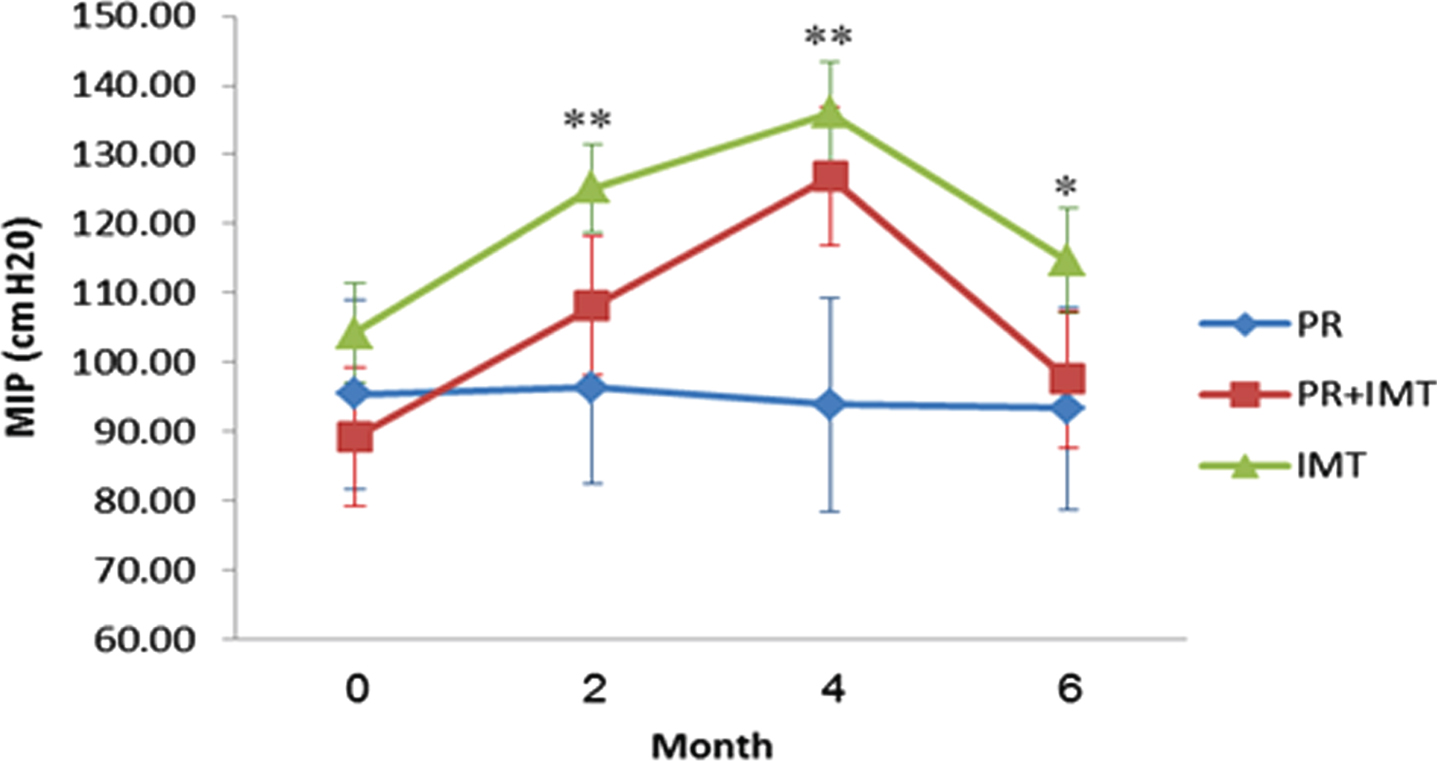
MIP (cm H2O) by month and group. Abreviations: PR, pulmonary rehabilitation group; PR + IMT, pulmonary rehabilitation combined with inspiratory muscle training group; IMT, inspiratory muscle training group; T0,baseline; T1, after 2 months of intervention; T2, after 4 months of intervention; T3, 6 months after T0; MIP, maximal inspiratory pressure. Data presented as means and standard deviations. Significant differences between the groups: *p < 0.05, **p < 0.01.
After 4 months of exercises, there was a statistically significant increase in the 6MWT in the PR combined with IMT and IMT exercise groups (30.6±80.5 and 48.8±71, p < 0.01), but not in the PR group (Table 4 and Fig. 2).
Intergroup Differences in the Extent-of-Change in 6 -Minute-Walk-Test (6MWT) Results, at t1 =ΔT1-T0, t2 =ΔT2-T0, and t3 =ΔT3-T0
Intergroup Differences in the Extent-of-Change in 6 -Minute-Walk-Test (6MWT) Results, at t1 =ΔT1-T0, t2 =ΔT2-T0, and t3 =ΔT3-T0
Abbreviations: PR, pulmonary rehabilitation group; PR+IMT, pulmonary rehabilitation combined with inspiratory muscle training group; IMT, inspiratory muscle training group; T0, baseline; T1, after 2 months of intervention; T2, after 4 months of intervention; T3, 6 months after T0; 6MWT, 6-minute walk test. Data presented as means and standard deviations. Significant differences between the groups: **p < 0.01.

6MWT (m) by month and group. Abbreviations: PR, pulmonary rehabilitation group; PR + IMT, pulmonary rehabilitation combined with inspiratory muscle training group; IMT, inspiratory muscle training group; T0, baseline; T1, after 2 months of intervention; T2, after 4 months of intervention; T3, 6 months after T0; 6MWT, 6-minute walk test. Data presented as means and standard deviations, significant differences between the groups: **p < 0.01.
There was a statistically significant correlation between MIP and MVV values, at baseline (r = 0.723, p = 0.001) after 2- and 4-months intervention, (r = 0.737, p = 0.0007 and r = 0.679, p = 0.0027) and at 6-months (r = 0.702, p = 0.0017) at follow-up (data not shown).
There was also a statistically significant correlation between MIP and 6MWT values at baseline (r = 0.661, p = 0.003) and after 2 months (r = 0.548, p = 0.022), and 6 months of the pilot study (data not shown).
Discussion
To the best of our knowledge, the present pilot study is the first prospective clinical trial to examine effects of PR, PR combined with IMT and IMT alone in a 4-month intervention, on inspiratory muscle strength, functional capacity, predicted values of VO2 peak and pulmonary function in post- LTx patients. The majority of the participants (13/19 participants, 68%) were more than one-year (16±2.2 months) post LTx.
The main findings show that in post LTx patients, PR combined with IMT and IMT alone yields statistically significant improvements in MIP and 6MWT values. Furthermore, the addition of IMT, to a PR program, results in an increase in inspiratory muscle strength, and an increase in 6MWT values. In PR alone (without IMT), no significant increases were seen. Compliance with the PR and IMT programs was very good, and the programs were well tolerated by all patients.
Prior studies illustrated respiratory muscle function impairment in patients who had undergone LTx [7, 8]. The results of this pilot study were in agreement with previously published studies on patients with COPD who received IMT [20, 34].
According to the World Health Organization’s Global initiative for COPD (GOLD) consensus, PR should be considered in all patients with FEV1 below 80% of the predicted value [35].
The importance of incorporating an exercise program in the management of LTx patients is emphasized in the latest update (2013) on PR in the American Thoracic Society/European Respiratory Society guidelines [36]. However, the quality of the evidence supporting this recommendation is low to moderate, and does not consider new experimental studies published in recent years. Moreover, the dosing and types of exercises that are most effective in this population have not been clearly defined, due to the wide variability in exercise protocols. Considering these facts and that the most recent review on this topic by Didsbury et al. (2013) only critically assessed the VO2 peak values in a subgroup of LTx recipients [37], the contribution of our current pilot study in updating the evidence on the benefits of exercises with the addition of IMT, or an IMT program alone, in adult LTx recipients, is of utmost importance.
In an evidence-informed clinical approach article, Wickerson et al. (2016) reported that MIP and maximal expiratory pressure (MEP) values, lower-extremity muscle force, and 6MWT distance continued to improve at 12 and 18 months after the LTx procedure. The VO2 peak test value, however, reached its highest predicted value at 6 months post LTx with no change at 12 or 18 months follow up [38].
IMT has been extensively investigated in patients with COPD, demonstrating it was associated with significant improvements in inspiratory muscle strength (MIP) and endurance, exercise capacity and quality of life, and decreased dyspnea [18, 19]. The addition of IMT to PR was also recommended by the joint ACCP/AACVPR 1997 committee [39]. Nonetheless, this intervention does not appear to be routinely incorporated into PR programs for COPD patients.
Our findings of the positive effect the PR program combined with IMT or IMT alone has on physiological and clinical outcomes in post- LTx patients can be explained by several mechanisms. It is possible that repetitive stimulus of high ventilator demands during exercise sessions, chest expansion during deep breathing, while exercising with the inspiratory muscle trainer device and strengthening and stretching of the thoracic and respiratory muscles, all of which were used in the present pilot study, resulted in a more efficient breathing pattern, and improved the respiratory muscles’ strength and performance.
Notably, given the interesting and positive results of our study, the lack of data on the level of respiratory muscle performance before admission to LTx is a drawback. It is likely that the starting level of respiratory muscle performance may be a factor conditioning the change after exercise. The results of our study consequently raise the question whether routine screening for weakness of inspiratory muscles should be performed in patients who are candidates for LTx. Particularly, in COPD patients, in whom respiratory muscle weakness is already well established.
To date, the prognostic value of PR alone, PR combined with IMT, or IMT alone in patients following LTx is unknown. Due to the simplicity, applicability, and cost effectiveness of using a home-based IMT program, we propose that a PR program combined with IMT or even IMT alone could provide additional benefits for patients following LTx. Although the maintenance strategy of IMT is still to be evaluated, there are conditions that would benefit from short IMT programs, such as post-surgery and after weaning from mechanical ventilation (e.g., post-ECMO COVID-19 patients). Moreover, respiratory muscle evaluation and rehabilitation should be an integral part of the management protocol of patients who have undergone LTx, given that statistically significant improvements were detected in MIP and 6MWT values, following these interventions, and enhancement in these parameters may increase physiological reserves. This issue needs to be further ascertained through long-term studies.
Limitations
Initially the pilot study design included a control group, however 3 of 5 patients dropped out of this group shortly after the research was initiated. Thus, improvements by natural history alone, without any exercise or IMT, could not be assessed. The pilot study results are limited due to the small number of participants combined with the high variability between participants, additionally the pilot study did not include other exercise or exercise combinations, thus to corroborate the current findings warrants conducting larger cohort studies. Langer et al. (2012) stated one limitation of their study was refusal of almost 40% of eligible candidates to participate [15]. We agree, this low participation rate, reflected in the small number of participants in these studies, indicates the difficulty in motivating patients to attend outpatient exercise training programs following LTx. Possible reasons are large travel distances to reach the transplant centers, or the large spontaneous improvements, perceived by patients. To partially overcome this drawback, we also exercised, supervised and evaluated a home-based training program with an inspiratory muscle trainer device. Moreover, in times of restricted mobility, such as due to the current COVID-19 pandemic, home-based training programs constitute an alternative to inaccessible outpatient exercise programs.
Recommendations and implication for future research
To establish whether patients who have undergone LTx require prolonged periods of PR to maximize the functional benefits of this procedure. To establish whether a home-based IMT program alone performed by patients who have undergone LTx can provide a sufficiently positive effect on exercise capacity. More research is required to assess the effect of inspiratory muscle training or combined inspiratory muscle training with additional pulmonary rehabilitation interventions that did not include inspiratory muscle training for different outcomes. Studies should aim to determine: optimal frequency, intensity and time of inspiratory muscle training for lung transplantation patients.
Conclusions
Outpatient PR together with home-based IMT seems to be the best exercise combination for achieving the optimal effect on inspiratory muscle strength and exercise capacity in our pilot study group of patients who have undergone LTx. Maintenance exercise should be implemented, otherwise the benefits achieved during the basic exercise will not be maintained beyond the exercise period. Whether maintenance exercise needs to be performed on a regular basis or by intermittent pulse exercise needs to be determined. Patients post LTx are able to perform IMT unaided at home, under some supervision, with relatively good compliance, and low monetary cost. Thus, patients should be encouraged to participate in a PR program that includes home-based IMT exercise as a part of the treatment protocol for this population, especially in these times of restricted mobility, due to the COVID-19 pandemic.
Footnotes
Acknowledgments
The authors thank the pilot study coordinators and nurses of the Pulmonary Institute for their help in the recruitment process, and the pulmonary function technicians for their professional assistance in the study. Finally, the authors extend thanks to Ms. Dalia Dawn Orkin for her important English language contributions and editing services and to Ms. Efrat Yaskil for her statistical assistance.
Conflict of interest
None of the authors have financial or other potential conflicts of interest to disclose.