
Abstract
PURPOSE:
The aims of the study were two-fold 1) to explore the treatment modalities musculoskeletal physiotherapists are utilising and the underlying reasons why and 2) report current continuing professional development (CPD) practises and their perceived effectiveness.
METHODS:
Using a cross-sectional questionnaire, musculoskeletal physiotherapists in the United Kingdom (UK) were invited to complete an online survey. The survey captured respondents’ professional characteristics and their main reason for selecting a range of treatments sub-grouped into three broad categories; Manual Therapy, Treatment Modalities and Education Based Approaches. Respondents were asked to report their CPD practises and their perceived effectiveness. Data was converted into proportions with lower and upper limits of the 95% confidence interval (CI). Likert scale questions were treated as numeric variables with the mean and standard deviation (SD) calculated for combined responses.
RESULTS:
Of the 414 responders, 408 were eligible for analyses. The most common reason for treatment selection, based upon a combined total of 9792 responses across all treatment modalities, was content taught in ‘entry-level training’ (n = 2010, 20.5%, 85% CI 20 to 21), followed by ‘practice related courses or CPD events’ (n = 1241, 12.7%, 95% CI 12 to 13). ‘Self-reflection’ was the most common form of CPD (n = 404). All forms of CPD were considered ‘effective’ for developing knowledge and skills except ‘clinical audit’ and ‘journal clubs’ which were rated as ‘indifferent’ by respondents.
CONCLUSIONS:
Treatment technique depends heavily on skills taught in entry-level training. Despite research articles amongst the most utilised forms of CPD, a disconnect exists in its implementation as the main driver of treatment selection. A wide range of CPD activities were undertaken by participants and rated as ‘effective’ for acquiring and applying physiotherapy related skills.
Introduction
Evidence based practice is the cornerstone of musculoskeletal physiotherapy practice and fundamental to the provision of quality patient care [1]. The concept uses current best evidence to inform decisions on individual patients based on skills, personal experience, and external evidence in a systematic and objective manner [2]. Clinical reasoning is a complex process in which the use of evidence-based practice is recommended [3]. One important aspect of clinical reasoning, alongside prior knowledge and information from patient assessment and diagnosis, is the selection of appropriate treatment interventions [4]. There is growing pressure on the physiotherapy profession to embrace evidence-based practice [5], enhancing proficiency and preventing misuse of healthcare services [6, 7]. A gap between evidence-based practice and physiotherapist treatment choices has previously been reported [8–10]. Following the beginning of the COVID-19 pandemic, clinicians have had to invent new approaches to patient care, adapting to drastically different ways of learning, teaching, practicing and researching the physiotherapy profession [11]. It is timely for musculoskeletal physiotherapists to re-examine their own selection biases to provide evidence-based practice ensuring quality patient care.
Physiotherapists’ reasons for treatment selection have previously been reported. Turner and Whitfield [9, 12] investigated the reasons for treatment selection with the choices primarily based upon the content of entry-level training. The use of journal literature represented only 5% or less of the reason’s respondents provided for technique selection. A similar study conducted in Kuwait reported less than 10% of respondents utilised research as a reason for treatment choice [8]. A divide exists between evidence-based practice and the actual reasons behind physiotherapists’ treatment selections. Up to 81% of treatments administered are either not recommended or have no recommendations [10]. Analysis of the justification behind musculoskeletal physiotherapists’ treatment choices may provide insight into the drivers influencing the application of evidence-based practice.
An additional component of evidence-based practice is on-going continuing professional development (CPD). CPD is integral in supporting graduates’ transition to clinical practice and for physiotherapists to maintain appropriate standards [13]. In much the way healthcare provision is undergoing a transformation, CPD is becoming increasingly innovative. The use of online courses, social media, webinars, and podcasts has increased in popularity and could be used as an effective way to provide continuous healthcare education [14, 15]. These methods of delivery are more accessible to a wider audience due to the cost and accessibility of online materials. Physiotherapists should recognise the importance of CPD for self-development and advancement of services among health care professionals [16], therefore additional knowledge of current physiotherapists’ choice of CPD and their effectiveness is warranted. Investigation of which methods of CPD physiotherapists adopt the most frequently and their perceived effectiveness alongside understanding the reasons behind their treatment choices will assist in understanding appropriate delivery methods of evidence-based practice.
Therefore, the aims of this research were two-fold. The primary aim was to understand the treatment modalities that UK musculoskeletal physiotherapists utilise and the underlying reasons why. Our secondary aim was to report current CPD practises and their perceived effectiveness.
Method
A cross-sectional survey of UK musculoskeletal physiotherapists was conducted from July 2020 to August 2020. The study was approved by Teesside University’s Health and Life Sciences ethics committee (249/19) in accordance with the declaration of Helsinki.
Design
The survey was based on previous work [9, 12] and was designed to capture; 1) participant background characteristics, 2) current musculoskeletal treatment approaches and reasons for selection and 3) current engagement and effectiveness of CPD (Supplementary Material 1). Questions were designed as dichotomous or Likert scale, of which all scales were unipolar [17]. The questionnaire was designed following pilot testing from ten musculoskeletal physiotherapists in the North East of England for content validity [18]. The pilot group were requested to provide comments on the format of the questionnaire, its content, wording, instructions, and overall ease of completion [8]. This process resulted in modifications to specific questions; additional questions (one), wording of questions simplified (three), addition of treatments (seven), addition of CPD options (four), and question sequence altered. The survey was piloted with a further five physiotherapists all of whom were requested not to complete the live survey. The final survey consisted of a total of 9 main questions (Supplementary Material 1).
Participants were asked to complete the questionnaire only if they were qualified physiotherapists within the United Kingdom and their current position included clinical duties. Participants were asked to answer the questions based on their treatment and CPD choices in the last 6 months of their clinical practice. Firstly, the survey gathered participants’ background characteristics including current position, duration of active clinical practice and physiotherapy related qualifications. The second section of the survey asked each participant to select current musculoskeletal treatment practices and the reasons for their use. Each respondent was asked to select only the main reason for treatment choice. The treatment list was not exhaustive and therefore respondents were able to select ‘other, please specify’ to capture those not included. The treatment approaches were separated into three broad categories ‘Manual Therapy (e.g. mobilisations, massage based treatments), Treatment Modalities (e.g. rehabilitation exercises, taping/strapping, acupuncture) and Education Based Approaches (e.g. self-management, movement/posture education)’. The reasons for selection of approaches were based on the work of Turner and Whitfield [9, 12] in addition to pilot testing.
Participants
The authors contacted the trade union body of UK physiotherapists, the Chartered Society of Physiotherapy (CSP), which currently has approximately 59,000 members. Due to the nature of the data held by the CSP, they were unable to identify the number of musculoskeletal practitioners amongst the membership. Therefore, conducting a formal sample size estimation to facilitate random sampling from an existing framework was not possible. We employed a recruitment strategy to seek the largest reach of UK musculoskeletal physiotherapists. A study recruitment message was posted via the Chartered Society of Physiotherapy’s interactive community (iCSP) providing the survey link (07/07/2020). The survey was hosted by onlinesurveys.ac.uk. Respondents were instructed regarding the aims of the study, the length of time required for completion (15 minutes) and the storage of anonymised data. Survey completion was voluntary with respondents able to withdraw prior to submitting the final answers. Respondents were instructed that by submitting the survey they were consenting to take part. No incentives were provided for survey completion. A reminder message was posted at two and four weeks prior to survey closure (31/08/2020). Respondents were encouraged to share amongst colleagues using a snowball method of recruitment [19].
Data analysis
Following survey closure the data were exported directly in Microsoft Excel (Microsoft, 2016), using the onlinesurveys.ac.uk analyse function. This survey was not designed to test for differences in practice between respondents and therefore no such analysis was performed. We present descriptive data with results from the dichotomous questions converted into proportions with lower and upper limits of the 95% confidence interval calculated using the Wilson procedure [20]. Likert scale questions were treated as numeric variables [21]. The mean and SD were calculated for combined responses across each potential option.
Results
Four hundred and fourteen physiotherapists completed the survey. Two participants began the survey but failed to complete and these responses were removed from data analysis. One was also removed due to not identifying themselves as a physiotherapist. A further three identified as a physiotherapist but not in a musculoskeletal role. This meant a total of 408 eligible participants completed the survey (Fig. 1) providing a total of 9792 individual responses.
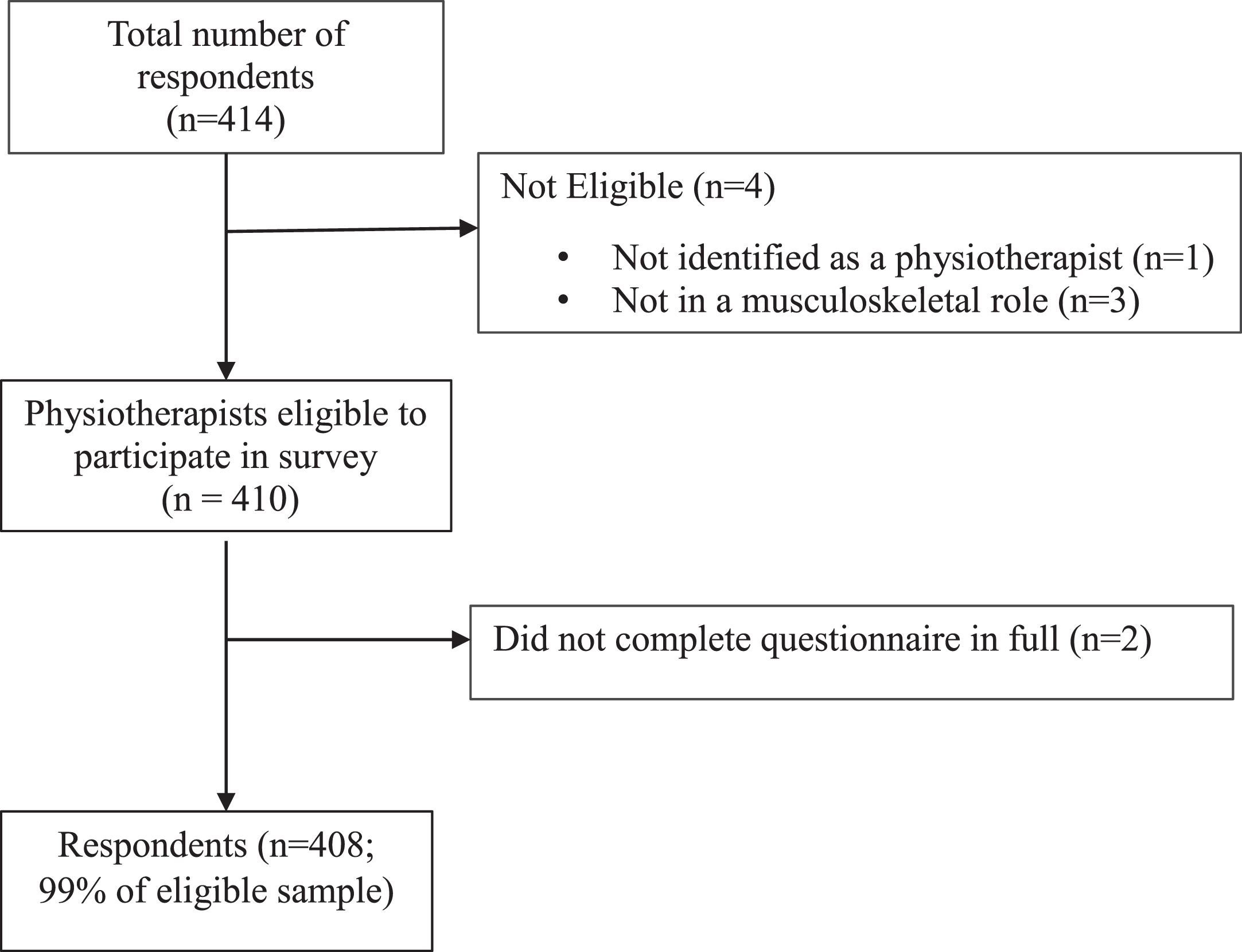
Flow diagram of musculoskeletal physiotherapists involved in the survey.
Participant characteristics are presented in Table 1. Of the 408 participants eligible for data analysis, in response to current position, 16 selected ‘other’. These can broadly be categorised as academics (n = 9, 2.2%), working clinically for the ministry of defence (n = 4, 1%), within a charity (n = 1, 0.2%), within occupational health (n = 1, 0.2%) and as a consultant physiotherapist (n = 1, 0.2%). Respondents were also asked about their background qualifications (Table 1). A total of 40 participants selected ‘other’, which were categorised as diplomas (n = 27, 67.5%), postgraduate certificates (n = 8, 20%), previous degrees (n = 4, 10%) and Master of Arts (n = 1, 2.5%). Sixty-five respondents who were registered on a postgraduate course included Masters of Science (n = 30, 46.2%), PhD (n = 10, 15.4%), postgraduate modules (n = 10, 15.4%), other non-accredited courses (n = 5, 7.7%) and Bachelor of Science (n = 2, 3.1%). For eight (12.3%) respondents not enough information was presented to categorise their post qualification course.
Participant characteristics
Key: NHS - National Health Service; MSc –Master of Science.
For each technique, the main reason provided for their selection was calculated as a percentage of the total number of potential reasons cited (total = 9792) per technique (Table 2).
Total reasons for treatment selection and their percentage of the total
Key: CI –confidence interval, CPD –continuous professional development.
For each of the broad categories, Manual Therapy (Table 3), Treatment Modalities (Table 4) and Education Based Approaches (Table 5), the number of reasons, overall % and 95% CI are presented. In each category, those participants who selected ‘other’ were able to input additional reasons not listed. Overall, the information provided reinforced already selected treatment choices, but a theme emerged of respondents only ‘occasionally’ using a technique for a specific condition rather than ‘always’. Other reasons for treatment selections include ‘following clinical guidelines’ and ‘own clinical reasoning’. A number of respondents did refer to carefully weighing up their scope of practice and clinical remit when answering the ‘Educational Based Approaches’ category in relation to ‘analgesia/medication related advice’.
Reasons for manual therapy treatment selections
Key: CI –confidence interval, CPD –continuous professional development.
Reasons for treatment modality selections
Key: * - including kinesiology tape, CI –confidence interval, CPD –continuous professional development.
Reasons for selection of educational based interventions
Key: CI –confidence interval, CPD –continuous professional development.
In relation to the Manual Therapy category, additional techniques utilised by participants not included in the original list were manipulations, muscle energy techniques, McKenzie approaches, Cyriax methods, cranial sacral therapy and neural mobilisations. A total of 49 participants selected ‘other’ from the ‘Treatment Modalities’ category. A range of additional treatment techniques were used regularly by respondents. The most popular included graded exposure, imagery, Tai Chi, electrical muscle stimulation, hydrotherapy, traction, laser therapy and pulsed shortwave diathermy. Motivational interviewing, cognitive behavioural therapy, health coaching, pain education, sleep management and signposting were the most common additional educational treatment approaches utilised.
Only 4 (1%) of participants had not engaged in CPD activity in the past 6 months. Reflection was the most used form of CPD (n = 404, 99%), followed by primary research articles (n = 387, 94.9%) and secondary research articles (n = 385, 94.4%). The perceived effectiveness of the range of CPD activities is presented in Table 6.
Respondents completed CPD within the last 6 months and perceived effectiveness
Likert Scale: 1, Very Ineffective; 2, Ineffective; 3, Indifferent; 4, Effective; 5, Very Effective. Key: RCT –randomised control trial, SD –standard deviation.
Evidence-based practice is at the forefront of musculoskeletal physiotherapy and involves clinicians integrating the best research evidence with clinical expertise to provide the most appropriate and effective service [2, 22]. The synthesis of research evidence from multiple sources, including formal education and CPD allows clinicians to generate clinical decisions known to improve patient outcomes [23]. The primary aim of this research was to understand the drivers which musculoskeletal physiotherapists in the UK use to influence selection of treatment modalities. Secondly, we aimed to establish the perceived effectiveness of a range of CPD activities. The results of this study suggest that entry-level education and practice related courses are the primary factor in treatment selection. Despite the utilisation of research articles, either primary or secondary, only 5.9% of total treatment selections were based on this evidence. Other key findings indicate that the most utilised forms of CPD are self-reflection and research articles however, podcasts/audio learning and practice-related courses are considered the most effective, questioning the perceived effectiveness of research-based articles and the utilisation of physiotherapists to translate this information into evidence-based practice.
Reasons for treatment selections
The most popular reason for treatment selection was associated with entry-level physiotherapy training (20.5%). For techniques administered by participants (i.e. those who did not select ‘never used’) entry-level training was overall the main reason across three categories: Manual therapy (30.9%), Treatment modalities (17%) and Educational based interventions (17%). The main reasons for the selection of these techniques are comparable to previous studies conducted in English based physiotherapists more than two decades ago [9, 12] suggesting a lack of progression towards enhancing the utilisation of research articles to influence evidence-based practice. It is important to acknowledge that clinical reasoning forms the basis of treatment selection and is itself the synthesis of numerous variables including prior knowledge, reflection, assessment information and diagnosis [24] and that participants may make treatment selection choices based on these factors. Respondents were asked despite this, to consider the primary reason for technique selection.
A large majority (82.8%) of respondents within our study had at least 5 years postgraduate experience with 66.9% accruing over 10 years. Despite this, techniques taught in entry-level training still played a substantial role in treatment selection and only a small number relied on information gained directly from research materials as the main reason for treatment selection. Despite this apparent lack of utilisation of research articles, it is understandable that a professional’s entry-level training may be based on information provided by research materials at the time of training, therefore interpretation of these findings should consider this. Our aim during this research was not to judge the treatment selections of UK physiotherapists against the evidence base but to understand the key metrics in decision making. This suggests that despite a physiotherapist’s professional responsibility to regularly updates one’s knowledge of evidence-based treatments [16], physiotherapists retain a bias towards treatments taught in their entry-level training. Only a small number relied on research articles as the main reason for treatment selection. Translation of research into clinical practice is considered an important part of a physiotherapist’s professional role [25]. Other studies have reported low rates of evidence used in decision making; UK 5.8%, Australia 6.2% [9, 12] and Kuwait 6.6% [8]. These studies asked respondents to consider up to three reasons for technique selection, however we wanted to understand the main selection biases of participants. Therefore, we are unable to conclude that use of research in the overall process of decision-making is low, our data does however indicate that UK musculoskeletal physiotherapists surveyed do not use research articles as the primary basis for treatment selection.
Physiotherapists value the role of evidence to support patient care, with literature deemed helpful in their practice [26]. American physiotherapists concluded that patient care was superior when evidence had been implemented [27]. Predictors of perceived research importance include previous research experience, being positive about undertaking research, working in a hospital environment, and holding postgraduate qualifications [28]. Constraints of the uptake of such evidence, which may have resulted in such low percentages of research articles at the forefront of treatment selections within our survey, include physiotherapists’ ability to access, read and interpret published research to allow implementation of findings [28]. Despite accessibility issues, our data shows that research articles are highly utilised within current CPD practices. Authors have a responsibility to present data in a meaningful and clinically relevant way to allow frontline staff to be able to interpret and implement evidence-based practice. A greater focus on research training within the scope of clinical skills, potentially within the entry-level training of physiotherapy, so important in our respondents’ decision making, may improve the uptake of evidence at the vanguard of clinical decisions.
Continuing professional development
CPD is a cornerstone of the profession and is mandatory in many countries to maintain physiotherapists’ registration. In the UK the physiotherapy regulator, the Health and Care Professions Council (HCPC) assesses the workforce against 15 ‘Standards of Proficiency’ [29]. CPD of registrants is monitored to ensure the continual development of new skills allowing clinicians to practice safely. A wide range of CPD activities exist which may influence the synthesis of treatment effectiveness [30] thus contributing to the generation of evidence-based practice. Whilst effectiveness is formed from many constructs, respondents were asked to consider their CPD engagements in relation to the acquisition and application of relevant physiotherapy skills in the delivery of high-quality care [30]. Our secondary study aim was to understand the perceived effectiveness of a range of CPD activities. Our data suggests a range of activities are undertaken by current musculoskeletal UK physiotherapists. Only audits and journal clubs were not considered ‘effective’. The most used forms of CPD were self-reflection (99%), and research articles both primary (94.9%) and secondary (94.4%). The significantly high levels of self-reflection reported within this study may be a consequence of its unique construct. Self-reflection is often not utilised in isolation but used in conjunction with other methods of CPD via exploring experiences which lead to new understandings and appreciations [31]. Though self-reflection is not a specific requirement for physiotherapists’ on-going registration with the HCPC it is encouraged across the broad range of potential CPD activities. This may explain in part our findings suggesting self-reflection as a pertinent component of physiotherapists’ continual learning. Self-reflection should be an important element of on-going CPD and that the delivery of evidence-based practice should include elements of this [32].
Despite our study suggesting a high percentage of research is used as part of respondents’ CPD, a disconnect appears to exist between this form of education and translation in the clinical environment. Primary care physiotherapists underuse evidence-based clinical practice guidelines or research recommendations when treating patients with musculoskeletal conditions [33]. Knowledge transition aims to integrate research into practice to enhance patient outcomes [34]. Currently, knowledge translation aimed at physiotherapists, has been concluded not to modify therapist behaviour and practice in the treatment of musculoskeletal conditions [35]. Further analysis of why this apparent disconnect between the high uptake of research articles but low utilisation in clinical practice may prove beneficial.
More recent online forms of CPD including podcasts and audio learning were considered the most effective (mean 4.27±SD 0.71) by the 90% of participants who accessed them. The CPD option with the least uptake of respondents, accredited practice related courses, scored amongst the most effective (4.27±0.84). Despite this perceived effectiveness, previous studies have demonstrated little supporting evidence for the benefit of course related activity in changing patient outcomes [36, 37].
CPD continues to be an integral aspect of physiotherapy with professionals obliged to undertake activity. Evidence suggests that CPD can positively impact the individual and the services in which they practice [38, 39]. As the clinical environment changes, so does the ways in which CPD is maintained. Accessibility to CPD through podcasts, webinars, online learning, and social media continues to grow. Web-based and computer-assisted learning in Canadian physiotherapists has been reported with 78% indicating a large positive interest in this format [40]. Whilst we acknowledge our list of CPD activities was not exhaustive, our data shows that most physiotherapists within our survey recently engaged in CPD and considered it effective.
In addition to registrant’s mandate to engage with CPD, the process is becoming increasingly important as the profession continues to evolve with specialist roles including first contact practitioners. Often the skills required for extended roles are not routinely part of entry-level physiotherapy education with training outside the traditional scope of their discipline necessary [41]. It is conceivable that modern forms of CPD may have a greater influence on the results from our study and a shift from the reliance on entry-level training as the cornerstone of treatment selection. Until this occurs, providers of physiotherapy education are required to digest the responsibility of providing graduates and clinicians with the key knowledge, theory, and skill acquisition to provide evidence-based care.
Limitations
Several limitations of this study need to be considered when interpreting the results. It is possible that the respondents are not representative of the entire target population [42, 43]. Due to the sampling method, it is not possible to estimate the denominator sample size of physiotherapists who received the invitation to complete the survey. We recognise that this survey does not represent the views of all musculoskeletal physiotherapists within the UK and that a reporting bias, as in participants who regularly participate in CPD are more likely to participate in the research, exists. Whilst entry-level training was the main driver for treatment selection, some treatment modalities utilised within this survey may not have been covered in pre-registration training. Such awareness may exist from other forms of CPD and therefore accessibility bias may exist. Our study was undertaken within the initial UK response to COVID-19. Whilst again, we did not seek to understand exact treatment selections for certain conditions, but the reasons for selection, we cannot rule out that responses were altered due to the pandemic. The six-month timeframe included pre-pandemic healthcare restrictions. Additionally, results may be subject to recall bias [44]. Respondents were asked to rate the perceived ‘effectiveness’ of CPD activities for their own learning and knowledge acquisition. Arguably ambiguous responses such as ‘effective’ and ‘not effective’ may reduce the specificity of participants opinions on forms of CPD. Future research should attempt to understand the reasons for the findings of this study and why entry-level training remains the main driver for technique selection. Investigating treatment selection and effectiveness between length of time qualified and postgraduate education would provide areas for exploration. Similar research to understand the effectiveness of knowledge transfer from the different forms of CPD highlighted in this study would be a welcome addition to the literature.
Conclusions
Despite physiotherapists perceiving the importance of evidence-based practice and implementation of research in patient care, a disconnect exists between the use of research and UK physiotherapists main reasons for treatment selection. Our data suggests that treatment technique depends heavily on those skills taught in entry-level training. Overall, a range of CPD techniques were considered effective, with self-reflection and research literature the most widely assessed. Podcasts/audio learning and accredited practice related courses were deemed the most effective methods of CPD.
Footnotes
Conflict of interest
None.
Ethical considerations
The study was approved by Teesside University’s Health and Life Sciences ethical committee (249/19) in accordance with the declaration of Helsinki.
Funding
This research did not receive any specific grant from funding agencies in the public, commercial, or not-for-profit sectors.