
Abstract
BACKGROUND:
Balance-based torso-weighting has improved gait and balance performance in people with multiple sclerosis (MS) in a single session with torso-weights on, demonstrating an orthotic effect. Daily use of torso-weighting may promote motor learning and more enduring therapeutic effects but has not yet been studied.
PURPOSE:
Confirm orthotic effects and compare therapeutic effects of daily torso-weighting versus shape/sham-weighting or no weighting. We hypothesized that daily torso-weighting would result in positive effects on gait and balance, tested without weights.
METHODS:
Five participants with MS experienced three conditions for 2-4 weeks each: no weights first, then double-blinded randomization to torso-weighting or shape-weighting first then cross-over to the alternate condition. Personalized torso-weighting on a vest-like garment countered individual reactive balance responses following manual perturbations. Postural sway recorded orthotic effects with/without torso-weights while standing on a force plate with eyes open/closed. Clinical measures recorded therapeutic effects while unweighted: gait parameters, 6-Minute Walk Test (6MWT), and Sensory Organization Test (SOT). Weighting conditions were compared using paired t-tests with one-tailed alpha at 0.05.
RESULTS:
Postural sway decreased significantly with torso-weights. Cadence and step width improved significantly after torso-weighting versus shape-weight periods. Average gait parameters showed no improvement after shape-weight periods. Velocity, 6MWT, and SOT tended to improve with torso-weighting, averaging improvements of+15%,+16%, and+13.8%, respectively.
CONCLUSIONS:
Findings support both orthotic and therapeutic effects of torso-weighting. Daily use of torso-weights for multiple weeks may promote motor learning of gait parameters and balance. Further research is warranted to examine sensory augmentation as a potential mechanism.
Introduction
Over 2.8 million people worldwide have a diagnosis of multiple sclerosis (MS) [1]. MS affects more females than males and is commonly first diagnosed in ages 20 to 50, typically years of high work productivity. MS is characterized by an immune response that attacks myelin and damages axons leading to lesions that slow or diminish conduction of neural impulses [2]. Dysfunction often includes reduced proprioception, muscle weakness, poor balance, and gait disorders, with an increased risk for falling. In fact, 30-70% of this population experiences falls within a 2-6 month period, and 30% of those who experience multiple falls sustain injuries [3–5]. Neural dysfunction and injuries can reduce activity and independence, putting people with MS at risk for comorbidities that negatively impact the rate of disease progression [6]. Promoting gains in motor skills may increase activity and decrease risk of injury, thereby lessening impairment and disability, and potentially slowing disease progression in people with MS.
Orthotic devices can help manage impairment and disability by correcting deviations in positioning or improving muscle activity for people with MS [7]. Orthotic effects have been reported during single-session applications of Balance-Based Torso-Weighting (BBTW), the customized placement of light weights on a vest-like garment (BalanceWear®, Motion Therapeutics, Inc., Oakland, CA, USA) based on directional balance loss with perturbation [8]. Torso-weighting using the BBTW protocol has improved upright mobility with weights on versus weights off [9–12]. However, clinical practice reveals that daily use of torso-weights may also promote motor learning [13]. Motor learning through augmented sensorimotor practice would mean that use of torso-weights carries over into improved performance observed after the individual takes the weights off; thus, a therapeutic effect could promote motor skill recovery.
So far, theories regarding mechanisms of action for weighting interventions [10, 14] address the orthotic effects but do not address potential therapeutic effects. For example, researchers have suggested that augmented sensory input, which may include customized placement of torso-weights, enhances feedback and thereby improves motor output [10, 16]. In people with MS, the immediate orthotic effect of torso-weighting may occur because torso-weighting helps compensate for poor sensory input, processing, or integration. However, daily use of torso-weighting while individuals engage in usual activities may also provide the repetition required for motor learning while directly targeting the sensorimotor aspects of balance recommended as the most successful type of intervention for improving upright postural control [17, 18]. If better motor output is practiced sufficiently, motor learning and neuroplasticity may result in a therapeutic effect of more automatic and efficient balance and gait. Further, research shows that people with MS having high fall risk and fear of falling tend to have less physical activity [19] which is associated with a greater number of comorbidities [20]. If motor output improves, fall risk and fear of falling may decrease, potentially increasing physical activity and ultimately decreasing comorbidities.
The purpose of this pilot study was to examine whether daily use of torso-weighting over a multi-week period had orthotic and therapeutic effects. We examined the orthotic effect of torso-weighting through centre-of-pressure measures with torso-weights off and on. We hypothesized that people would show decreased postural sway when wearing the weights compared to not wearing the weights. We examined the therapeutic effect of daily use of either torso-weighting or shape/sham-weighting through gait and balance measures tested without weights. We hypothesized that following 2-week periods during which participants wore torso-weights, they would experience more positive effects on gait and balance than after 2-week periods of daily use of shape-weighting.
Materials and methods
This pilot study was a double-blinded, randomized cross-over trial approved by the Institutional Review Boards of Samuel Merritt University in Oakland, CA, and San Francisco State University in San Francisco, CA, USA.
Participants were independent community-dwelling individuals recruited through the National Multiple Sclerosis Society and local neurologists’ offices. A convenience sample was selected of the first 5 volunteers to meet the eligibility criteria. Eligibility criteria included a self-reported diagnosis of MS, ability to ambulate at least one minute at a time (with or without assistive device), reported balance or mobility difficulties, and ability to endure up to 3 hours of testing with rest breaks. In addition, participants had to be at least 18 years of age and able to communicate in English. Individuals were excluded if they reported an exacerbation of MS in the two months before entering the study, a diagnosis of a concurrent neurological condition (head injury, stroke, Parkinson’s disease, etc.), or reported pain that could be exacerbated by testing. All participants signed written consent forms prior to participation.
Before testing, participants completed a medical questionnaire with information about their symptoms including self-reported visual and sensory dysfunction, walking ability, and fall history. Testing measures included force-plate measures of centre of pressure (COP) to assess the presence of an orthotic effect. COP changes were recorded while standing on a 600 Hz force-plate (BMS400600, Advanced Medical Technology Inc, Watertown, MA). COP statistics were calculated sampling at 25 Hz as in Hunt, et al. [21], using equations by Prieto, et al. [22]. Motor learning effects were assessed using clinical measures of gait and balance. We assessed gait parameters on an instrumented gait-mat (Zeno, Protokinetics, Havertown, PA), including velocity, step length, percent of gait cycle in single limb support, stride width, and cadence. Gait endurance was assessed by the distance covered during a 6-Minute Walk Test (6MWT). Balance measures included the Sensory Organization Test (SOT) using the NeuroCom® SMART EquiTest Balance Master (Natus Medical Inc., Pleasanton, CA) and a diary of falls experienced during the three periods of the study. Self-report questionnaires included the Movement Ability Measure-Computer Adaptive Test (MAM-CAT) [23], Activities-Specific Balance Confidence Scale (ABC) [24], Multiple Sclerosis Impact Scale 29 (MSIS-29, physical and psychological components) [25], and Multiple Sclerosis Walking Scale 12 (MSWS-12) [26]. The balance, disease impact, walking self-report measures, and the 6MWT are endorsed for assessment in people with MS by the MS-EDGE taskforce of the American Physical Therapy Association [27]. The MAM-CAT has good reliability and validity for documenting participant-centred goals and progress in outpatient populations, and has been successfully used in MS [28]. The SOT has been used to examine the sensory components of balance and has a documented 7-point cut-off for meaningful change in MS [12, 29].
Participants attended 4 sessions in the research lab. During the first visit, participants performed baseline testing on the clinical balance and gait measures, completed the self-report questionnaires, and were measured to order a custom-fitted vest for weight application. At the end of visit 1, participants selected a sealed envelope that randomized the order of weighting they would experience for the 2-week periods between visits 2–3 and 3–4 (Fig. 1).
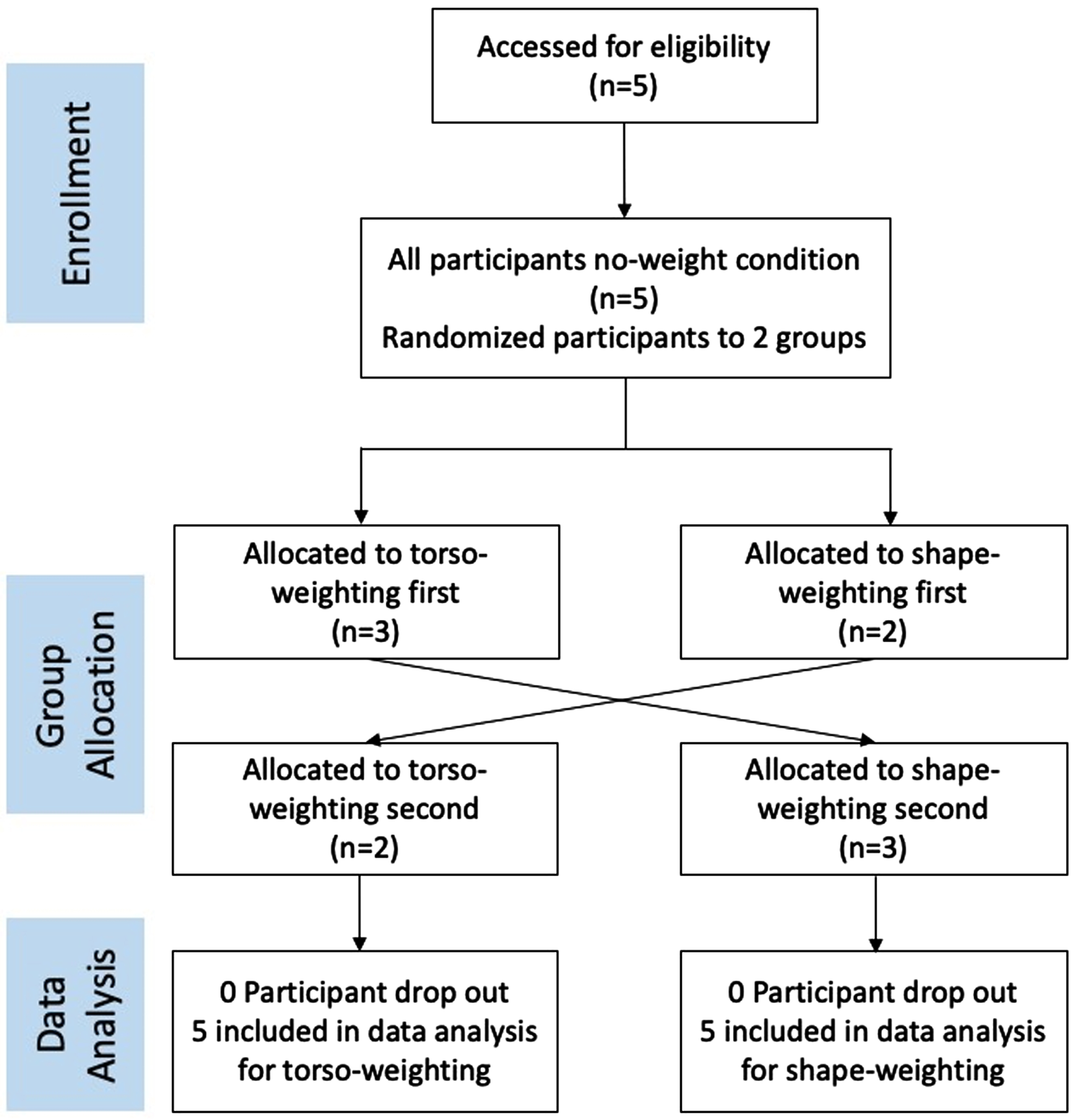
Consort Diagram showing cross-over research design.
The custom-fitted vest was ready by visit 2, approximately 4 weeks after visit 1 (Fig. 2). In visits 2–4, participants repeated all baseline tests and then donned the unweighted vest. Then their static standing balance was tested by standing on a force-plate with eyes open and then eyes closed for 30 seconds each.
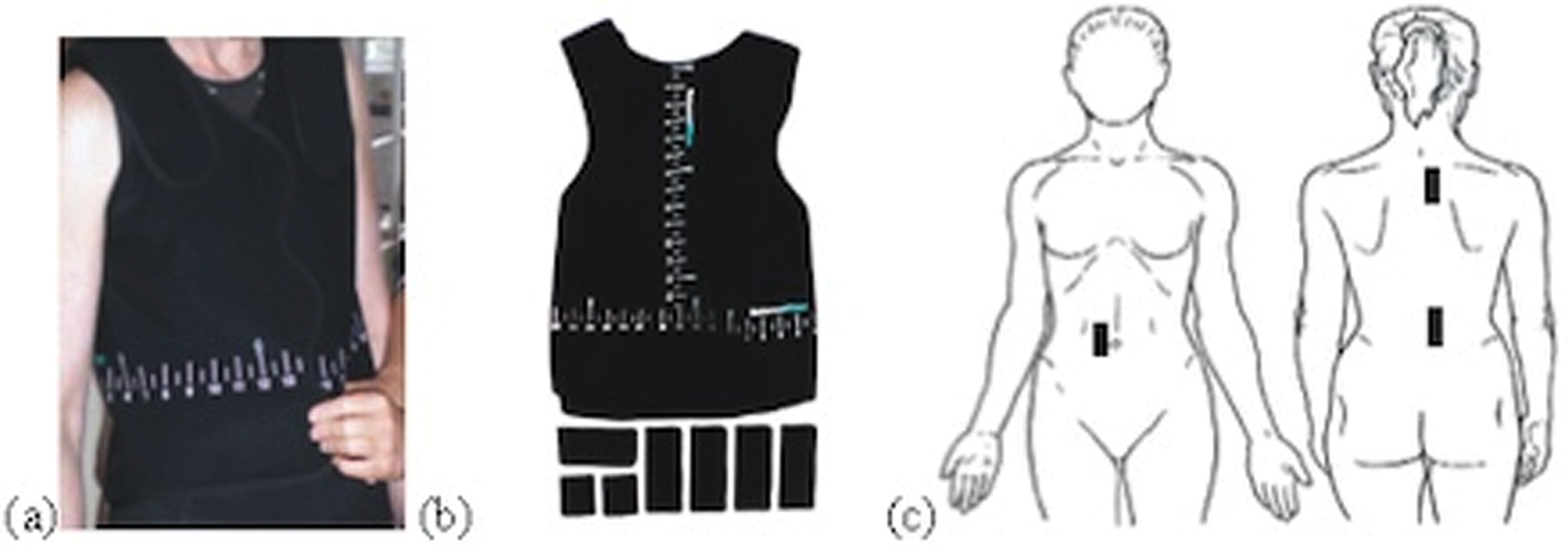
Torso- and shape/sham-weighting vest (a) on a person; (b) with weights depicted below the vest; and (c) with sample weight placements.
After the force-plate assessment with the unweighted vest on, a trained clinician followed a standardized torso-weighting procedure [10]. The participant stood with feet together. The clinician applied systematic manual perturbations and observed the participant’s directional balance loss or instability. Perturbations included nudges in the anterior-posterior and lateral directions at shoulders and pelvis, and resisted rotations in clockwise and counter-clockwise directions also at shoulders and pelvis. The clinician then determined the optimal location and amount of weight in an iterative process and applied the weights to the vest via Velcro (Velcro Companies). Optimal torso-weighting minimized loss of balance, movement of the feet, or latency of recovery to upright position; total weight ranged from 0.1 to 0.9 kg.
After the torso-weighting procedure, participants repeated the force-plate assessment with the weights on. When testing was completed, the vest was removed, and a single researcher (GLW) not performing the clinical tests marked the locations and weight amounts and determined the appropriate weighting according to the randomized order for that participant: either keeping the torso-weights or substituting them with same-shaped sham-weights (SW). The shape/sham-weights were polystyrene foam in the same size and shape and covered with the same black material as the torso-weights. Shape or sham-weights made an authentic placebo because, like torso-weights, sham-weights were placed on the inside of a close-fitting vest, usually worn over clothing; the sham-weights helped control for the potential effect of similar shapes pressing lightly against the torso in the same location as torso-weights would.
All assessors during testing were blinded to randomization order. Participants were told that the vest would have variable weights at different periods during the study. Participants were instructed to wear the vest for 2-4 hours per day until the next visit 2 weeks later. In addition, participants completed a daily activity log to record falls experienced throughout the study periods, and how long they wore the vest each day. Following the final intervention period, participants returned for final testing in session 4.
Data were analysed using paired t-tests in a cross-over study design. No order effect of conditions became apparent, so torso-weighting and shape-weighting periods were analysed together without regard to order of weighting experienced. Changes in variables following torso-weighting and shape-weighting conditions were calculated based on the value for each measure at the visit immediately before that condition was experienced. Comparisons were made based on each participants’ paired changes for torso-weighting compared to shape-weighting periods.
We used one-tailed tests with alpha value of 0.05 because we expected the torso-weighting condition to have better outcomes than the shape-weighting condition. Graphs detailing percent change for each variable during weighting periods include the no weight period between visits 1 and 2 (about 4 weeks). Percent changes are shown with standard error bars calculated using equations specified for percent differences [30, 31].
The five volunteers with MS (Table 1) had median (range) Patient Determined Disease Steps scores of 4 (2-5), where 4 indicates a late cane-dependent stage where the person cannot walk 25 ft without the use of a cane or other unilateral support. The number of falls reported in the last six months averaged 2.4 (range 0-8). Participants 1, 2, and 4 wore torso-weights between visits 2–3 and sham-weights between visits 3–4. Participants 3 and 5 wore sham-weights between visits 2–3 and torso-weights between visits 3–4.
Participant characteristics
Participant characteristics
PDDS=patient determined disease steps, MS = multiple sclerosis, TW = torso weight, SW = shape weight.
In all participants, the amount of torso-weight required to achieve reduction in balance loss decreased over the 3 weighting visits (Table 1). The range of torso-weighting (in kilograms) was 0.31-1.29% body weight.
Figure 3 shows the COP paths and 95% confidence interval circle areas of the sway path with and without weights. Comparison of COP path mean distance, resultant distance, and 95% circle area showed statistically significant decreases (p < 0.05) in sway with weights on compared to weights off with both eyes open and eyes closed. The difference in 95% circle area was 4.8 (0.4, 9.2) cm2 with eyes open and 9.1 (0.8, 17.5) cm2 with eyes closed.
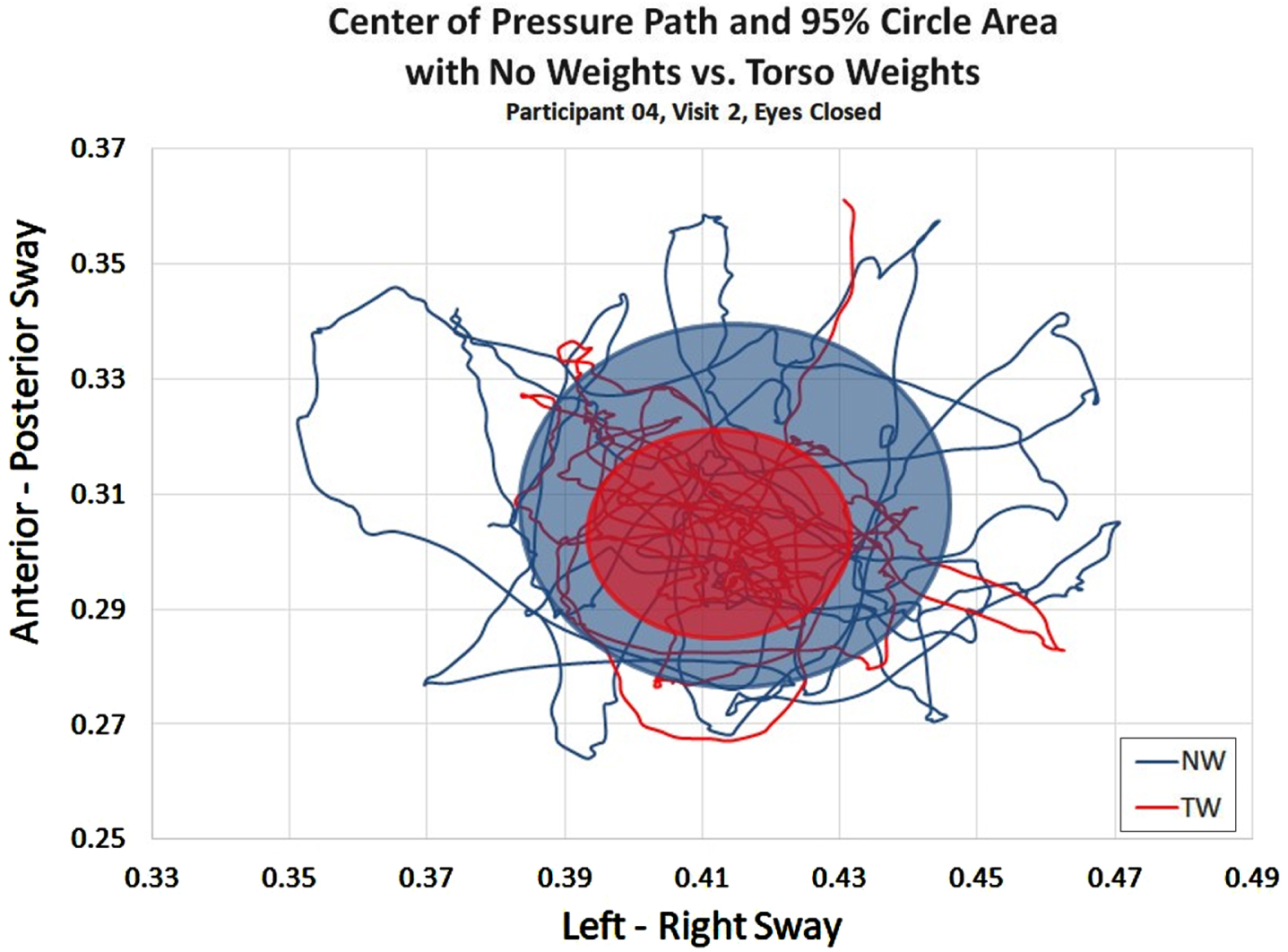
Representative participant (P04) and condition (eyes closed) comparing centre of pressure path and 95% circle area of sway path while standing on a force-plate with and without torso-weighting. NW = non-weighted, TW = torso-weighted.
Participants reported having no falls during weeks with the torso-weighting condition, while 1 non-injurious fall occurred in time periods with the SW condition. No other adverse events were reported. Additional outcomes are presented in Fig. 4. For the non-weighted initial period between visits 1–2, average performance for each variable decreased or showed negligible improvement (13.4% decrease to 3.5% increase). Changes in participants’ average values for torso-weighting and shape-weighting periods were calculated by subtracting the values obtained at the beginning from the ending visits of the applicable period.
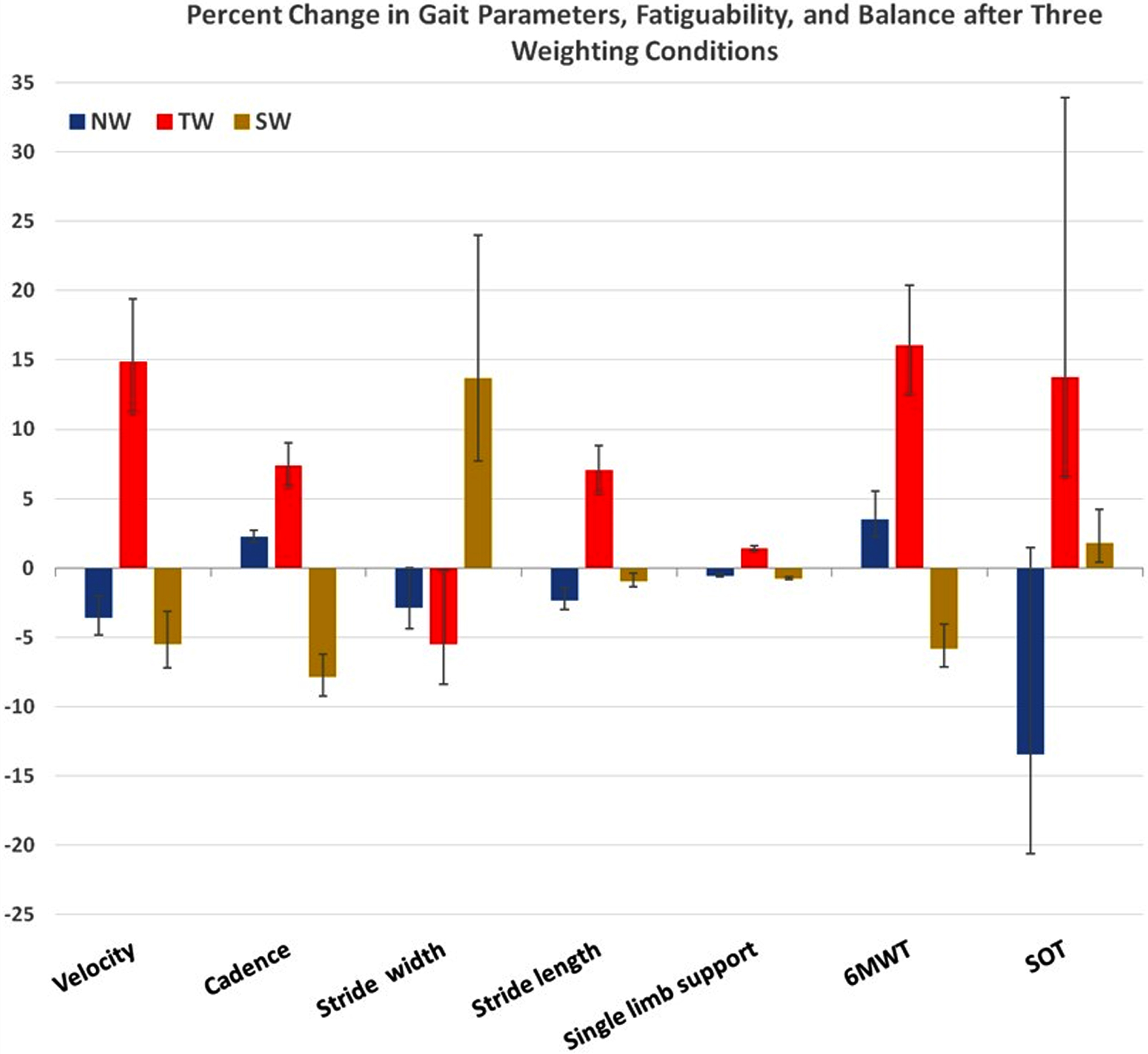
Percent changes in gait parameters, motor fatiguability, and balance after each of the three weighting conditions. Positive and negative standard errors were calculated from percent change confidence intervals [31]. NW = no weight; TW = torso-weighting; SW = shape-weighting; 6MWT=6-Minute Walk Test; SOT = Sensory Organization Test.
All gait parameters tended to improve with torso-weighting, and to worsen with shape-weighting (see Fig. 4). Differences in stride width and cadence were significant: for stride width, the difference between torso-weighting and shape-weighting was -3.9 (95% CI: -6.7, -1.1) cm with p = 0.02. For cadence, the difference between torso-weighting and shape-weighting was 14.6 (95% CI: 1.1, 28.0) steps per minute with p = 0.04. Differences in gait velocity after torso-weighting versus shape-weighting periods did not reach significance (p = 0.08) although the average change was 12.7 cm/sec (95% CI: 0.42, 25.0) after torso-weighting periods and -5.3 cm/sec (95% CI: -17.5, 6.9) after shape-weighting periods.
Differences in participants’ average distance walked during the 6MWT averaged 46.0 m (95% CI: –4.8 m, 96.8 m) (+16%) during torso-weighting periods compared to an average difference of –19.0 m (95% CI: –61.3 m, 23.3 m) (–5.8%) during SW periods. The paired t-test comparing torso-weighting and shape-weighting differences in 6MWT did not reach statistical significance (p = 0.08).
Standing stability
SOT tended to improve after wearing torso-weights by an average of 7.4 (95% CI: –0.7, 15.5) composite score points (+13.75%) compared to 1.0 point (95% CI: –8.2, 10.2) (+1.8%) after wearing sham-weights. The paired t-test comparing torso-weighting and shape-weighting changes did not reach statistical significance (p = 0.19).
Mean differences in outcomes for Torso-weighting (TW) compared to Shape-Weighting (SW) Interventions
Mean differences in outcomes for Torso-weighting (TW) compared to Shape-Weighting (SW) Interventions
†Baseline values given for reference. TW (torso-weighting) and SW (shape-weighting) values and percent changes reflect differences from values obtained at visit (2 or 3) immediately preceding the time-period for each condition. ††Pooled standard errors calculated from upper and lower bounds of 95% confidence intervals for percent differences. [31]. * p < 0.1; **p < 0.05. SE- Standard Error, 6MWT-6 Minute Walk Test, SOT-Sensory Organization Test, MS-Multiple Sclerosis, MAM-CAT-Movement Ability Measure Computer Adaptive Test, ABC-Activities Balance Confidence Scale.
This pilot study provided evidence of both an orthotic and therapeutic effect with torso-weighting. Participants showed changes in postural sway with torso-weights on versus off, consistent with an orthotic effect. We rejected a null hypothesis of no difference for postural sway. Participants also showed improvements in gait parameters after wearing torso-weights but not sham-weights for 2–4 hours a day for 2 weeks. We rejected a null hypothesis of no difference for the gait parameters of step width and cadence. All gait parameters were assessed with weights off, implying a therapeutic effect. Changes in gait velocity, 6MWT, and SOT tended toward improvement, but did not reach statistical significance in this 5-person study.
Decreased 95% circle areas of postural sway in this study advanced the findings of previous studies. Crittendon et al. [10] documented greater postural sway changes in the right-left direction than in the anterior-posterior direction but did not record 95% circle areas of sway. Previous studies examined orthotic effects in single sessions [10, 21]; participants in the current study showed consistent orthotic effects across multiple visits despite decreasing amounts of torso-weights placed (see Table 1).
Unique to this study were the therapeutic effects noted when comparing performance after torso-weighting and shape-weighting periods. Improved stride width and cadence (p = 0.02 and 0.04, respectively) along with trends toward improvement of gait velocity and 6MWT distance can have clinical importance. A decreased stride width typically indicates improved stability; increased cadence indicates faster movement, implying higher gait velocity. Gait velocity showed an average improvement with torso-weighting at 0.127 m/sec (95% CI = 0.0042, 0.25 m/sec), higher than previous reports of MCID at 0.1 m/sec for pathologic populations including MS [32], or adult geriatric populations [33]. Improvements in step width, cadence, and gait velocity may reflect greater economy of locomotion, with more energy directed forward rather than side to side. Greater economy may have contributed to the 46.0 m (95% CI = –4.8 m, 96.8 m) average increase in walking distance during the 6MWT. While no MCID is available for people with MS [34], a calculated minimally important change for individuals with mild symptoms from MS is 21.6 m on the 6MWT. For adults with non-neurologic pathology, MCID ranges from 14–30.5 m [35], implying that improvements in walking distance after daily use of torso-weighting may be clinically important in the current sample. Further, average gait velocity changed over the 6MWT: overall gait velocity was 7.5 (95% CI = 2.8, 12.1) cm/sec less than gait velocity for the initial 26 feet of the 6MWT. A two-tailed t-test confirmed that the slow-down in velocity from the beginning of the 6 minutes was significant (p = 0.003). Participants used the 0–10 Rate of Perceived Exertion (RPE) scale immediately following the 6MWT, with four participants rating exertion 2–5 and one participant rating the exertion as 7–8. Such ratings indicate a broad range in the experience of exertion among the participants in this sample, although the 6MWT distances at baseline ranged from 196 m to 367 m, below normative values for healthy adults (616 m±61.9 m) and below average values for those with severe disability from MS (378 m±83.1 m) [36]. In comparison, in a study of the orthotic and therapeutic effects of functional electrical stimulation (FES), the baseline 6MWT for 11 people with MS was 372 m±114. The authors reported average improvement to 384 m±128 with FES off after 8 weeks of use, but no indication of wear time during the 8 weeks [37].
While prior research has shown that wearing torso-weights has an orthotic effect on SOT performance [12], SOT scores after torso-weighting versus shape-weighting periods did not reach statistical significance in the current 5-person sample (p = 0.19). However, the 7.4 point average improvement after daily use of torso-weighting exceeds the 7.0 point minimal detectable change identified by Hebert [29] and Horn [12]. These results suggest that the SOT is worth incorporating into future research examining the potential therapeutic effects of torso-weighting on stability. Static and dynamic stability are relevant to people with MS because of their propensity for falls. The average number of falls claimed by our participants in the 6 months prior to beginning the study was 2.4. There were no reported falls during the two-week torso-weighting period, and only 1 fall each during the 4-week baseline (no-weighting) and 2-week shape-weighting periods. Further research is needed to determine fall risk reduction with daily use of torso-weighting.
Clinical implications
Strategic torso-weighting does not act solely as an orthotic device, supporting function when donned. Improvement noted with weights doffed implies that motor learning may occur during a period of regular use of weights. Torso-weighting could be used initially as an orthosis for several hours a day, potentially improving balance control. Practicing movement with augmented sensory input could promote the motor learning effects we recorded in gait efficiency with decreased stride width and increased cadence. As changes in their condition and mobility occurs, an individual could return to their physiotherapist or other healthcare provider to have the torso weights adjusted to fit the individual’s current balance deficits. We noted that the amount of torso-weight decreased over the 3 weighting visits for all participants (Table 1); if people accommodated to the sensory input, they would have needed additional weights to retain the same level of effectiveness. Further research is warranted to study the long-term effects of torso-weighting across larger populations. This would increase the generalizability and external validity of our research.
Limitations
This pilot study examined only 5 people, which limits power for several variables. However, these people represent the variability of MS effects, with PDDS levels ranging from 2 to 5. Parametric statistics were used in the comparisons of torso-weighting and shape-weighting performance despite the small sample size; we repeated the analysis with the non-parametric Wilcoxon matched pairs signed ranks test which confirmed that both cadence and gait width were significantly different across the two conditions. Future studies should increase the sample size to improve precision of effects for gait velocity, 6MWT, and SOT. In addition, future studies should increase the number of weeks that people wear the torso-weights to provide more than two weeks to integrate sensory augmentation and develop motor skills through the repetition of experience. The decrease in amount of weight required across three visits (Table 1) suggests that people may still be learning through both torso-weighting and shape-weighting periods. Perhaps wearing the vest with torso-weighting or shape-weighting encouraged participants to increase their activity levels.
The 6MWT provides information about gait endurance but typically does not stress most participants to fatigue. In our sample, participants were unusually low in their recorded 6MWT distances compared to age-matched adults and people with MS, and some had relatively high levels of fatigue and high perceived exertion on the 6MWT. These findings occurred even though the test was performed without the weights on, and performance tended to improve after periods when participants wore the torso-weights daily. Future studies could take participants’ fatigue levels into account by obtaining self-report fatigue data that delineates which tasks cause motor fatigue. Future studies could also capture qualitative information about comfort and ease of use that might affect long-term fatigue and adherence.
No specific activity levels were prescribed along with torso-weighting or shape-weighting although participants were instructed to wear the vest during active periods of their days. Future studies could personalize exercise prescription and activity monitoring for individuals to assess whether improved performance and motor skill gains are associated with increased activity when participants wear the weights. Such information could help confirm that sensory augmentation via torso-weighting may encourage practice and yield greater motor learning.
Conclusion
Daily use of torso-weighting can improve gait and balance compared to sham-weights or no-weights. Regular use of strategic torso-weighting can improve motor performance with weights on and when assessing performance without weights. While donning torso weights in a single session, improvements are seen in decreased postural sway on a force-plate, confirming the orthotic effect. Use of torso-weighting for 2-4 hours daily over two weeks may promote motor learning through practice, resulting in a therapeutic effect of improved gait and balance even when the torso-weights are removed. This was the first study to investigate torso-weighting using the BBTW protocol as more than just an orthotic device. The findings add to the body of knowledge of effective interventions for people with MS to promote motor skill recovery, increased physical activity, and decreased fall risk in this population. Future studies are warranted to assess the therapeutic effects of torso-weighting in a larger sample size to increase external validity and generalizability.
Footnotes
Acknowledgments
This study was partially funded by a small grant from San Francisco State University –Office of Research and Special Projects (ST649).
Conflict of interest
The Authors declare that they have no conflicts of interest.
Ethical considerations
This cross-over pilot study was registered: Clinicaltrials.gov identifier: NCT02743312.