
Abstract
BACKGROUND:
Motor impairments are common consequences in people with multiple sclerosis (PwMS). These impairments limit function independence and decrease activities of daily living. Focal muscle vibration (FMV) produces vibration signals affecting the central nervous system. No systematic review has been published investigating the effects of FMV on motor impairments in people with MS.
OBJECTIVES:
This review was conducted to investigate the effects of FMV in motor rehabilitation in PwMS.
METHODS:
PubMed, SCOPUS, REHABDATA, PEDro, CINAHL, EMBASE, MEDLINE, and Web of science were searched from their inception until May 2023. Studies were included if they were experimental studies, used FMV in PwMS, and evaluated motor impairments. Studies were excluded if they used other forms of vibration application (e.g., whole-body vibration) or used pharmacological treatments as a primary intervention. We evaluate the risk of bias using the Physiotherapy Evidence Database (PEDro) scale.
RESULTS:
Five studies met our eligibility criteria. Three studies were randomized controlled trials, a clinical controlled trial (n = 1), and a pilot study (n = 1). A total of 123 participants were included in this review (Mean age = 47), 42.28% of whom were men. The PEDro scale scores ranged from three to eight. The findings revealed beneficial and non-beneficial effects of FMV on motor function in PwMS.
CONCLUSIONS:
The FMV application is safe and well-tolerated in PwMS. The evidence for the impacts of FMV on motor impairments in PwMS was limited. Additional studies with long-term follow-ups are encouraged.
Introduction
Multiple Sclerosis (MS) is a neurodegenerative disorder characterized by autoimmune-induced demyelination and inflammation of nerves in the central nervous system (CNS) [1]. This damage interrupts the transmission of signals along the axons, leading to various symptoms [2]. Approximately 2.8 million individuals live with MS worldwide in 2020 [3]. Women are three times more likely to be affected by MS than men [4]. Most MS cases are recorded between the ages of 20 to 50 years [4].
Motor impairments such as gait dysfunction, balance deficits, spasticity, and muscle weakness are expected consequences of MS [5]. Approximately 85% of people with multiple sclerosis (PwMS) develop gait dysfunctions due to balance deficits, increased muscle tone, and mobility restriction [5, 6]. The severity of gait dysfunction is linked with the degree of muscle weakness, spasticity level, and degree of impaired coordination [7]. Spasticity may limit the range of motion (ROM) and cause pain and abnormal body postures that affect individuals’ activities of daily living (ADL) [8]. Spasticity in PwMS should be assessed and treated as this impairment negatively disturbs walking abilities [9], general mobility, and balance [10]. A wide range of rehabilitation and medical interventions are available to address motor impairments linked with MS [11].
Most disease-modifying treatments use medications that regulate immune stimulation to reduce disease progression, relapses, or reverse disability [12]. However, these medications encompass many side effects, such as a developed risk of secondary immunosuppression, thus increasing the risk of infections. Treatments have been reported in monotherapy only, while other non-pharmaceutical treatments without identified side effects might have added benefits [12], one of which is focal muscle vibration (FMV).
FMV is a mechanical apparatus designed to create vibrational impulses targeting a specific muscle or tendon [13]. These vibrations induce the activation of muscle spindles [14], thereby generating Ia inputs and subsequently modifying corticospinal pathways [15]. It has been reported to increase excitability in the primary motor cortex following the application of low-intensity FMV [16]. The FMV intervention was used to promote motor ability post spinal cord injuries [17], strokes [18–20], and Parkinson’s disease [8]. This review aims to examine the impacts of FMV on motor impairments in PwMS.
Methods
Search strategy
The Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) guidelines were followed [21]. A literature search was conducted to identify suitable studies published from inception to May 2023 in PubMed, SCOPUS, CINAHL, EMBASE, MEDLINE, PEDro, REHABDATA, and the Web of Science databases (Fig. 1). The key search words were (Multiple sclerosis [MeSH] OR Relapsing-Remitting OR Chronic Progressive OR MS) AND (Local vibration OR focal vibration OR segmental vibration) AND (Postural balance [MeSH] OR Motor function OR Gait ability OR Walking function OR Muscle spasticity [MeSH] OR Muscle tone OR Hypertonia [MeSH] OR Paresis [MeSH] OR Muscle strength OR Motor impairments OR Motor) (Appendix A).
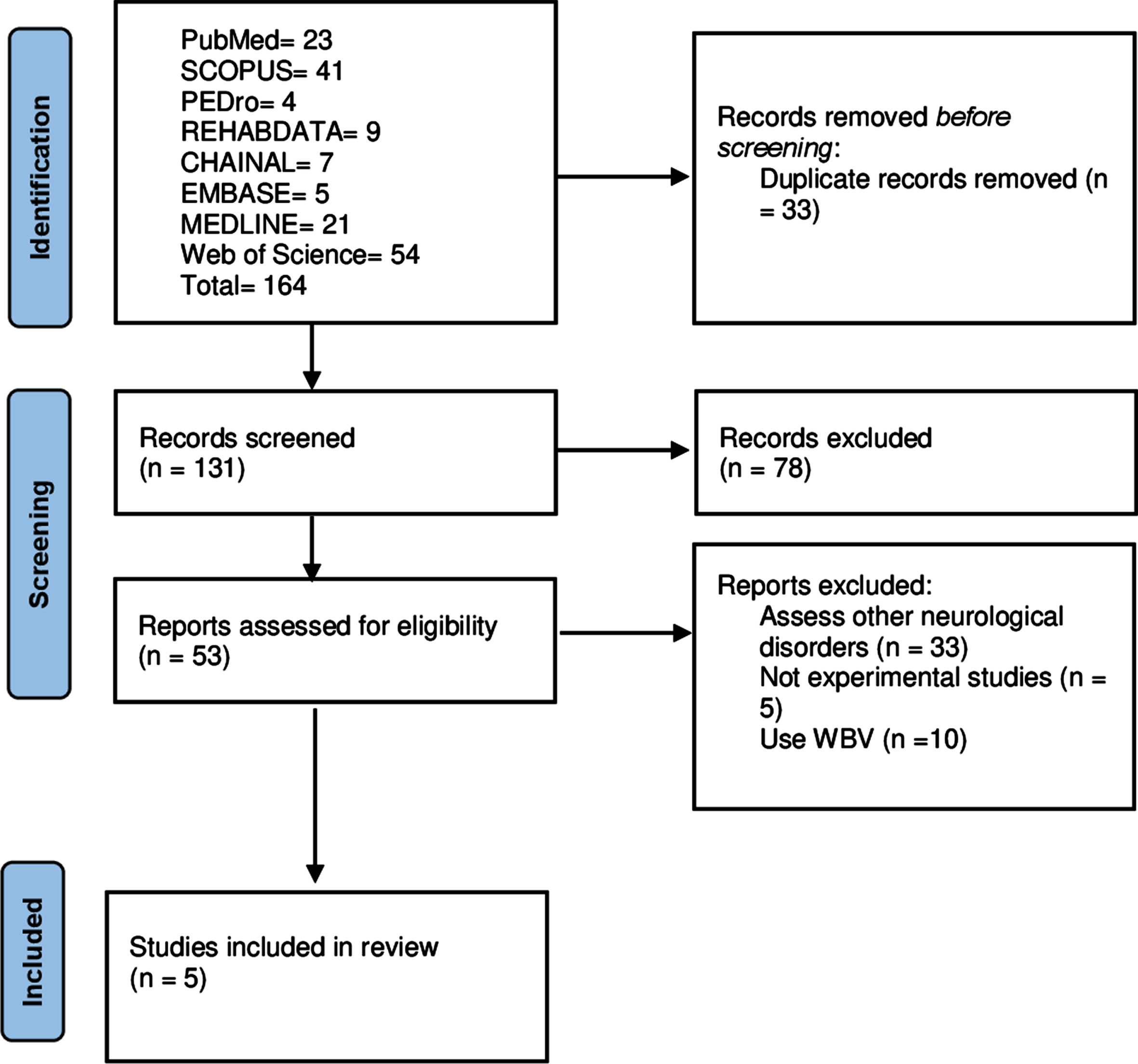
Summary of the literature review process.
The Patients, Intervention, Control, Outcomes, and Subjects (PICOS) approach was applied [22]. Studies were selected if they were (a) conducted on individuals with a diagnosis of MS, (b) used FMV technology with or without combination with other interventions, (c) compared with other active, placebo, or no treatments, (d) evaluated motor impairments (e.g., gait deficits, balance dysfunction, spasticity), and (e) being randomized controlled trial (RCT), clinical controller trial (CCT), or pilot studies published in English. Exclusion criteria were (a) conducted on individuals with other conditions (e.g., traumatic brain injury, cerebrovascular disease), (b) using the whole-body vibration (WBV) training method, and (c) using the pharmacological treatments as the main intervention. The initial evaluation was completed by studying the studies’ titles and abstracts. Wherever needed, the whole study’s manuscript was reviewed.
Data extraction
Table 1 displays the study characteristics of the selected studies. The following information was extracted independently: (a) authors and publication date, (b) patient characteristics, (c) vibration treatment details (i.e., Apparatus, Frequency, Amplitude, Target muscle), (d) intervention group, (e) comparison group, and (f) adverse events. The following information was summarized: (a) outcomes assessed spasticity, (b) time of evaluation, (c) intervention outcomes, (d) comparison outcomes, and (e) the findings (Supplementary File 1). The quantitative analysis was not appropriate due to the heterogeneity among the studies.
Participant characteristics and study design
Participant characteristics and study design
FMV: focal muscle vibration; CPT: conventional physiotherapy; Con: control; wk: week; min: minute; n: number; M/F: male/female; sec: second, RR: relapsing remitting; PP: primary progressive; SP: secondary progressive; NA: not applicable.
The risk of bias was assessed using the Physiotherapy Evidence Database (PEDro) scale. It is a reliable and valid tool for evaluating the risk of bias [23–25]. Based on https://pedro.org.au/english/learn/pedro-statistics/ [26], >5/10 is considered ‘high quality’, 4–5 ‘moderate quality’, <4 ‘poor quality’ (Table 2).
Methodological quality scores
Methodological quality scores
+ Low risk of bias. –High risk of bias.
Study selection
A search of PubMed (yielding 23 citations), MEDLINE (21), CINAHL (7), EMBASE (5), SCOPUS (41), PEDro (4), REHABDATA (9), and Web of Science (54) produced 164 citations. After eliminating duplicates, 131 papers were checked. Of those, 78 studies were dismissed because their summaries did not meet the eligibility criteria (i.e., MS, FMV). After that, 53 articles were assessed in full because suitability could not be defined by the abstracts. Then, 48 citations were excluded because they: (a) assessed other neurological diseases, (b) used WBV, and (c) did not do experimental studies. A total of five experiments were involved in the present study (Fig. 1).
Participants
Five experimental studies met the eligibility criteria. Three studies were RCTs [27–29], a CCT (n = 1) [30], and a pilot study (n = 1) [31]. A total of 123 participants were included in this review, 42.28% of whom were men. The mean age of the included participants was 47±10.33 years. The Expanded Disability Status Scale (EDSS) mean score for the included participants was 4.77±1.12 (Table 1).
Intervention
In the RCT by Paoloni et al. [27], the participants in all groups received botulinum toxin to the rectus femoris muscle, gastrocnemius muscle, and soleus muscle 15 days before the FMV intervention. After that, participants in the experimental and first control groups received 30 minutes of FMV over the rectus femoris and gastrocnemius muscles (10 minutes each) using (Horus, Akropolis, Rome, Italy), 30 Hz, 10 μm, three times a week for four weeks [27].
In the RCT by Ayvat et al. [28], all the participants received 60 minutes of traditional physical therapy intervention. After that, the experimental interventions were administrated (50 Hz, 100 Hz, 1 μm) using Vibrasens\copyright over the medial heads of the right and left gastrocnemius (5 minutes each). Three weekly sessions for eight weeks were administrated [28].
In the RCT by Spina et al. [29], the experimental intervention consisted of 9000 Hz FMV using Equistasi ® with an amplitude set at 0.02 μm over bilateral quadriceps (30 minutes each). Participants in the control group received placebo-turned-off FMV. All participants received five weekly sessions for three weeks [29].
In the CCT by Feys et al. [30], the participants in the experimental group and the healthy individuals in the control group received FMV using (Dynatronic; vibrateurs proprioceptive: VB10) with an amplitude set at 1 μm and 70 Hz frequency over tendons of the wrist extensor muscles (5 minutes each) for a single session [30].
Finally, the participants in the pilot study by Camerota et al. [31] received FMV with a frequency set at 100 Hz and 200–500 μm amplitude applied over bilateral quadriceps tendon lumbar paraspinal muscles (30 minutes each) using (CRO ®SYSTEM, NEMOCO srl, Italy) for 3 consecutive sessions [31].
Adverse events
No adverse events were expressed following the FMV applications in the included studies.
Effects of FMV on motor impairments in PwMS
Balance
There were significant improvements in the Single Leg Stance Test (SLST) [28], Level of Stability (LoS) [28], Medio-lateral sway- normal stability eyes closed (NSEC) [28], and Berg Balance Scale (BBS) [29, 31] following the FMV interventions. No significant differences between groups in the LoS Antero-posterior [28], LoS Stability Score [28], Antero-posterior sway-normal stability eyes opened (NSEO) [28], Medio-lateral sway-NSEO [28], Antero-posterior sway-NSEC [28], and Dynamic Gait Index (DGI) [29] were reported.
Gait
The patients improved significantly in the gait speed [28, 31], step length [28], the base of support [28], stance phase for more and less affected limbs (reduced stance phase) [31], double support phase for more and less affected limbs (decreased double support phase) [31], swing phase for less affected limb [31], step length for more and less affected limbs [31], stride length for more and less affected limbs [31], cadence [31], spatial asymmetry index (SAI) (decreased SAI) [31], temporal asymmetry index (TAI) (reduced TAI) [31], stride length [29], and double support (reduced double support phase) [29] following the vibration interventions. No significant differences in the double support [28], single support [28], stance [28], swing phase for more affected limbs, and step width were reported [28, 31].
Spasticity
The participants in the study by Ayvat et al. [28] showed that the Modified Ashworth Scale (MAS) scores of medial heads of right and left gastrocnemius improved (spasticity reduced) after the FMV interventions [28]. All participants in the study by Paoloni et al. [27] had improved significantly in the MAS scores (spasticity reduced) of knee extensor and ankle plantar flexor muscles [27]. The MAS scores for bilateral quadriceps did not change significantly between the groups [29].
Muscle power, range of motion (ROM_, and tremors
There was a significant enhancement in ROM for more and less affected hips [31], power for more and less affected hips [31], and power for more and less affected ankles [31]. No significant differences in the ROM for more and less affected knees [31], ROM for more and less affected ankles [31], and Fahn’s tremor rating scale were reported [30].
Methodological quality
The PEDro scale scores ranged from three to eight (Median = 6). Generally, one study met eight criteria [29], one met seven criteria [27], one met six criteria [28], one met four criteria [30], and one met three criteria [31].
Discussion
This is the first systematic review on the effects of FMV on motor impairments in PwMS. The main results demonstrated mixed evidence of the benefits of FMV for various motor outcomes in PwMS. Recently, a systematic review by Alashram et al. [18] reported that the impacts of FMV on gait and postural balance following neurological disorders were ambiguous [18]. Other systematic reviews showed that FMV plays a crucial role in reducing spasticity poststroke and spinal cord injuries[19, 32].
FMV stimulates the Ia inputs through the alteration of the muscle spindle leading to stimulating the corticospinal tract excitability by encouraging inputs and adjusting cortical inhibition to the cerebral primary motor area [13–16]. Muscle vibration can raise the motor potential from the muscle at relaxation [33]. This presented the development of corticospinal excitability changes [16]. FMV impacts proprioception and expands its role in supporting balance and encouraging gait [34, 35]. Increased muscle tone and reduced muscle strength are the major factors that influence walking and balance in individuals with neurological diseases [36, 37]. It has been reported that the vibration of the antagonist may decrease agonist tone [19] and enhance muscle strength [38]. Although there has been significant development of disease-modifying treatments in PwMS, it is essential to manage various impairments linked with MS [39]. MS impairments interfere with daily life and result from motor disorders. In turn, motor impairments are widespread and associated with a poor prognosis [40].
Spasticity is common in PwMS [5]. The included studies assessed spasticity using MAS. This scale is used as a clinical measure for muscle tone assessment in patients with various neurological diseases. However, this outcome measure is inappropriate for objective assessment of muscle tone and often requires to be paired with other outcome measures [41, 42]. Studies show that spasticity reduced after 50 Hz [43] and 30 Hz [29] FMV treatment to rectus femoris after spinal cord injuries. In a further study, a reduction in spasticity was demonstrated (using MAS) after 30 Hz FMV application to the flexors of upper extremity stroke survivors [20]. Spina et al. [29] explained the failure to find FMV efficacy on spasticity since as in most clinical assessments [29], several scales suffer from ceiling impacts and are not reactive enough to evaluate small progress [44].
Balance impairments can restrict the activities of daily living [45]. The included studies demonstrated heterogeneous evidence for the effects of FMV on balance abilities. Many lower limb muscles and joints are essential in adjusting the balance in the anteroposterior direction [46]. On the other hand, balance in the mediolateral direction is accomplished only by stimulation of the hip abductors and adductors, and the other lower limb joints do not contribute to modifications in the mediolateral direction [47]. Hence, any deficits in the mediolateral balance would be more opposing due to the risk of falling [48].
Most PwMS experience gait impairments [6]. Most of the included studies showed enhancements in gait ability after FMV. Ayvat et al. [28] demonstrated that the training group revealed an enhancement in the single support and stance [25]. The fact that the development in gait parameters was more auspicious following FMV application could be ascribed to the reduction in spasticity and activation of proprioception [10, 49]. The reduction in spasticity offers the development of numerous spatiotemporal gait parameters [9].
The vibratory stimuli application of specific muscles can recover the activation of the locomotion neuronal generators in the central nervous system through reestablished sensorimotor integration [50]. An increase in hip extension movement is associated with a rise in moment and power peaks [51]. Furthermore, the significant increase in the lower limb’s ROM could relate to a reduction in muscle tone and the capability of the FMV to adjust the sensory inputs to the CNS through the alteration of muscle spindles [15].
The study’s methodological quality was different. The selected studies had a high risk of bias in concealed allocation [27–31], which could generate selection bias. On the other hand, one study [31] had a small sample size, which is not appropriate to estimate differences [52]; hence, it is not feasible to demonstrate the significance of the stated impacts. The selected experiments did not demonstrate adverse events following FMV application. Therefore, while the clinical impact has not been established evidently, FMV seems to be a secure application for PwMS. Alashram et al. [18] reported that FMV is safe in patients with neurological diseases [18].
Future recommendations
As the selected studies used various treatment interventions for FMV, including numerous parameters and applications, the ideal treatment protocols for treating motor deficits in PwMS remain indistinct. The studies did not mention clear information about the FMV tools and some parameters (i.e., on/off ratio, force). Reporting the FMV device characteristics and parameters in upcoming research would focus on this point. Furthermore, the MS population (i.e., Secondary Progressive, Relapsing-Remitting, Primary Progressive) expected to benefit from FMV remains ambiguous. Recently, systematic reviews suggested combining rehabilitation interventions to enhance motor outcomes in patients with neurological disease [18, 45]. Imminent studies should emphasize the investigative impacts of combining FMV with other concurrent non-pharmacological treatments, such as virtual reality, WBV, functional electrical stimulation, transcutaneous spinal cord stimulation, stretching, and rhythmic auditory stimulation at the same time. Additional experiments with a larger sample size are encouraged to define the optimal FMV parameters in treating motor impairments.
Limitations
There are several limitations to the present review that should be acknowledged. The search process in the current review was limited by papers available in English. Studying only articles available in English could lead to an overrating of treatment impacts [53, 54]. Moreover, the current review included different study designs due to the paucity of published RCTs on the current subject. Lastly, the meta-analysis was not conducted because of the heterogeneity in the application designs, protocols, and tested areas among the selected studies.
Conclusion
FMV is well-tolerated in PwMS. The evidence for the impact of FMV on motor impairments in PwMS was limited. Combining FMV with concurrent rehabilitation treatments may lead to significant enhancement in motor impairments in PwMS. The most effective FMV application dosage remains ambiguous. Further studies are encouraged.
Footnotes
Acknowledgments
I would like to thank Dr. Qusai Janada, assistant professors in the physiotherapy department at Middle East University, and Dr. Giuseppe Annino, Associate professor, University of Rome Tor Vergata, for their general supervision in search strategy, data extraction, and methodological quality assessment.
Conflicts of interest
The author declares no conflicts of interest.
Funding
None.
Appendix A: Search strategy in MEDLINE
Multiple sclerosis [MeSH] Relapsing-Remitting Chronic Progressive MS 1 or 2 or 3 or 4 Focal vibration Local vibration Segmental ibration 6 or 7 or 8 Postural balance [MeSH] Motor function Gait ability Walking function Muscle spasticity [MeSH] Muscle tone Hypertonia Paresis [MeSH] Muscle strength Motor impairments Motor 12 or 13 or 14 or 15 or 16 or 17 or 18 or 19 or 20 5 or 9 or 20