
Abstract
BACKGROUND:
Respiratory physiotherapy is a core area of practice, but little is known about pre-qualification physiotherapy curricula across institutions. The purpose of this study was to identify and categorise the pre-qualification content of respiratory physiotherapy curricula across the island of Ireland.
METHODS:
This cross-sectional survey was conducted remotely and eight respiratory module coordinators/teaching leads participated. Respiratory physiotherapy curricular topics and assessment details from each participating institution were documented. Curricular topics were then grouped and categorised into discrete broader curricular topic areas by agreement. A representative from each higher education institution rated the curricular topic from their programme as ‘foundation’, ‘core’, ‘not essential but desirable’ or ‘broadly relevant’. Assessment strategies for each programme were documented.
RESULTS:
From 246 individual topics, seven broad category areas were generated which were operationally defined and divided into 41 content topics. Of the content topics 18 out of 41 (44%) topics were unanimously rated as core to the respiratory module by each participating programme. A diverse range of assessment strategies were employed across programmes with all including written and practical components.
CONCLUSION:
Between programmes and institutions, there was a reasonably high degree of overlap of the respiratory physiotherapy topic areas which are delivered within or outside of core respiratory modules. Content appears to be broadly standardised and appears to support the preparedness of graduates for practice in this area. The identification of ‘core’ respiratory topics in this study may be useful for the design of new respiratory physiotherapy modules or ongoing curricular review.
Introduction
Respiratory physiotherapy is widely regarded as a core subspecialty of physiotherapy [1]. The practice of respiratory physiotherapy can improve quality of life in people across the age span with respiratory disease and plays a key role in their management [2, 3].
The concept of physiotherapy is over a century old with respiratory physiotherapists originally promoting deep breathing exercises to ‘strengthen the chest, lungs and stomach’ [4].Some of the primary areas of practice include; respiratory care for patients with acute or acute-on-chronic respiratory disease [e.g. chronic obstructive pulmonary disease (COPD), asthma, cystic fibrosis (CF) and bronchiectasis], pre- and post-surgical care (e.g. thoracic, cardiac and abdominal surgery), critical care (e.g. intensive care and tracheostomy care), general medicine and outpatient pulmonary and cardiac rehabilitation [5]. Respiratory physiotherapists work with patients across diverse settings including inpatient hospital wards and critical care units, patients’ homes, outpatient pulmonary rehabilitation units and outreach/community-based settings [6–8]. Physiotherapy treatment can improve functional ability and reduce intensive care and hospital stay, with savings in associated health-care costs [8].
In some countries, respiratory physiotherapy is still only emerging [9] as a core sub-discipline of physiotherapy, while in other countries, such as Ireland and the UK, competence must be demonstrated in this area in order to be awarded a physiotherapy qualification [5]. Accredited physiotherapy programmes on the island of Ireland are recognised by CORU (Health and Social Care Professionals) Registration/Irish Society of Chartered Physiotherapists (ISCP) in the Republic of Ireland and the Health Care Professions Council (HCPC)/Chartered Society of Physiotherapists (CSP) in Northern Ireland.
CORU standards of proficiency [10] are set out under five domains including (i) professional autonomy and accountability, (ii) communication, collaborative practice and teamwork, (iii) safety and quality, (iv) professional development, (v) professional knowledge and skills. These standards of proficiency are applied to each core area of physiotherapy including respiratory. HCPC outlines 15 standards of proficiency for physiotherapists including “registered physiotherapists must practice safely and effectively within their scope of practice” and “be able to draw on appropriate knowledge and skills to inform practice”. Graduates are equipped to manage a standard in and out-patient paediatric and adult respiratory physiotherapy caseload. The Faculty of Intensive Care Medicine Guidelines for the Provision of Intensive Care Services [11] recommends that physiotherapy be an integral part of any respiratory team providing effective and practical management for the benefit of patients with respiratory compromise [2].
In most acute hospitals, physiotherapy for critically ill patients is available 24 hours a day, seven days per week [11] through the provision of out-of-hours on-call services/emergency cover and rostered weekend work. Additional training to become ‘on-call competent’ is usually provided on-site, [12] building on a knowledge base and basic level of competency from the pre-qualification physiotherapy curriculum. Extended scope and specialist physiotherapy roles have also become a feature of many physiotherapy sub-specialist areas including respiratory physiotherapy [13].
Respiratory physiotherapists employ a variety of treatment strategies with the aim of enhancing sputum clearance, reducing and minimising the experience of dyspnoea, improving ventilation and cough efficacy, increasing global muscle strength, physical fitness and function [3] This may include positioning to maximise ventilation, dyspnoea management techniques, whole-body exercises to improve strength and function, and the application of active breathing techniques and adjuncts to maximise secretion clearance and lung function [2, 7], with treatment generally directed towards the underlying pathological problem [14]. There are no standardized or ‘conventional’ respiratory physiotherapy treatment protocols [14].Treatment is diverse due to individual patient presentation, ongoing development of evidence-based practice [3, 13] and collation of clinical data [8]. Respiratory physiotherapists therefore provide treatment based on individualised assessment, clinical reasoning [15] and best available evidence [16].
A proposed core syllabus for postgraduate training in respiratory physiotherapy has been developed, as part of the Harmonised Education in Respiratory Medicine for European Specialists (HERMES) initiative [17]. However, uncertainty remains in relation to pre-qualification respiratory physiotherapy training as there are no curricular guidance documents and there is a lack of knowledge of essential elements and content for pre-qualification respiratory training.
The overall aim of this study was to identify and categorise respiratory physiotherapy curricula for physiotherapy pre-qualification programmes across the island of Ireland.
Specific objectives were to: Identify the educational content relating to respiratory physiotherapy-across pre-qualification programmes Describe the main respiratory physiotherapy topics covered in the curriculum and categorise as ‘foundation’, ‘core’, ‘additional’ or broadly relevant’ Allocate individual topics into defined broader topic areas Identify and describe respiratory physiotherapy assessment practices between curricula
Methods
Respiratory module coordinators/teaching leads with primary responsibility for respiratory physiotherapy content from all higher education institutions (HEIs) across the island of Ireland (n = 8 staff) identified the need to examine core respiratory physiotherapy curricular content which was the catalyst for the development of this study. This cross-sectional study was conducted remotely and took place between June 2020 and June 2021. An All-Ireland approach was taken as students access physiotherapy courses and employment in both countries and professional bodies work closely together. Ethical approval for this study was granted from the School of Medicine Research Ethics Committee in Trinity College Dublin.
Procedure
To capture curricular content a specifically designed excel template was generated by two content experts (OOS, BF) with significant undergraduate experience and involvement in respiratory physiotherapy curricula. Data captured included; modes and hours of delivery (lectures, practical laboratory classes, tutorials) module aims, learning outcomes, topic area covered (in any depth), assessment methods, number of students per year, European Credit Transfer and Accumulation System (ECTS) [18] assigned to the modules and year of delivery. Module titles were already publicly available in respective course prospectuses and all institutions were willing to share details of their respiratory curriculum as it related to the 2018–19 (pre-COVID) academic year. The excel template was shared on a secure cloud storage system with respiratory academic coordinators/teaching leads across the island of Ireland. All information was collated without institutional identifiers.
Each respiratory module coordinator/teaching lead then categorised their own curricular content to reflect whether in their programme it was considered foundation, core, additional or broadly relevant according to the Table 1 below.
Identification of curriculum content as Foundation, Core, Additional or Broadly Relevant
Identification of curriculum content as Foundation, Core, Additional or Broadly Relevant
Data were collated in an excel document and descriptive statistics were conducted to profile and summarise the variables of interest. Two members of the group (RC & CH) extracted the curricular data and collapsed individual topics areas into discrete broad categories. This allocation was then reviewed by the wider group during a collaborative discussion to agree the number and allocation of categories. Each category was operationally defined with examples and/or key words by pairs of team members and reviewed by the entire team. In the case of disagreement, or when items were subject to multiple interpretations, detailed discussion provided clarity and resolution.
Results
Participants of this study were respiratory module coordinators/teaching leads from all six HEIs on the island of Ireland offering physiotherapy programmes; Republic of Ireland (n = 5), Northern Ireland (n = 1). Currently BSc Physiotherapy programmes are offered in Royal College of Surgeons in Ireland (RCSI), Trinity College Dublin (TCD), University College Dublin (UCD), University of Limerick (UL), Ulster University (UU), and MSc Physiotherapy Pre-Registration Programmes in University College Cork (UCC), UCD and UL. Two HEIs (n = 2) offered more than one physiotherapy pre-qualification programmes (BSc and pre-registration MSc), therefore details from a total of eight pre-registration courses were included in this study. Programmes varied in length as pre-registration MSc programmes were two years in duration, one BSc programme was three years in duration while the rem-aining BSc programmes were four years in duration.
In five programmes, all respiratory curriculum content was delivered within one academic year while three programmes delivered content over two academic years. For four year BSc programmes, the majority (n = 3) delivered all respiratory curricular content in year two, while one programme delivered this content across year two and three. In the 3-year BSc programme respiratory curriculum content was delivered in year one and year three. In two of the MSc pre-registration programmes the respiratory curriculum was delivered in year one, while the other MSc programme delivered this content over both years of the course.
ECTS credit value assigned to the respiratory curriculum and contact hours varied between programmes. The majority of programmes (n = 4) were 10 ECTS. Two programmes were 6 ECTS, and two programmes were 20 ECTS. Timetabled teaching hours for the respiratory content varied; 42–104 hours on BSc programmes and 48–94 hours on MSc programmes.
From an initial list of 246 individual topics covered in all respiratory physiotherapy programmes seven broad category areas were generated: (i) fundamentals of CR physiotherapy, (ii) common respiratory diseases, (iii) respiratory assessment and measurement, (iv) respiratory treatment and management, (v) respiratory management for specific populations, (vi) physical activity and exercise and (vii) critical care. Operational definitions and corresponding content for each area was agreed. A curriculum map of additional broader category areas, operational definitions and content rated by respiratory module coordinators/teaching leads was developed (Tables 2A to 2G).
Fundamentals of cardiorespiratory physiotherapy
Fundamentals of cardiorespiratory physiotherapy

Common respiratory diseases

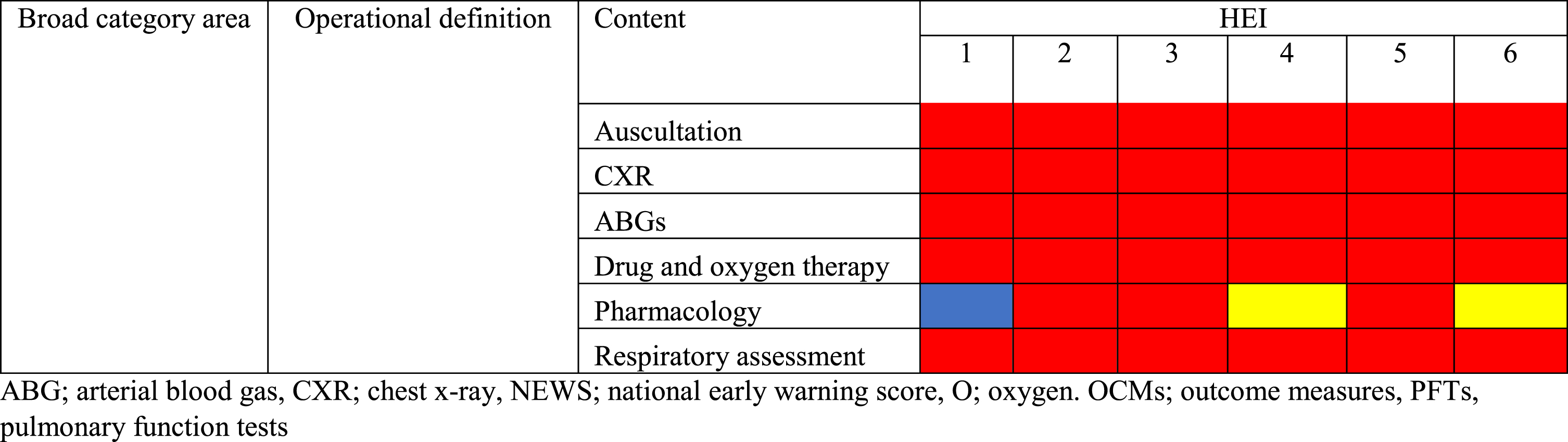
Respiratory assessment and measurement
Respiratory treatment and management

Respiratory management for specific populations

Physical activity and exercise

Critical care
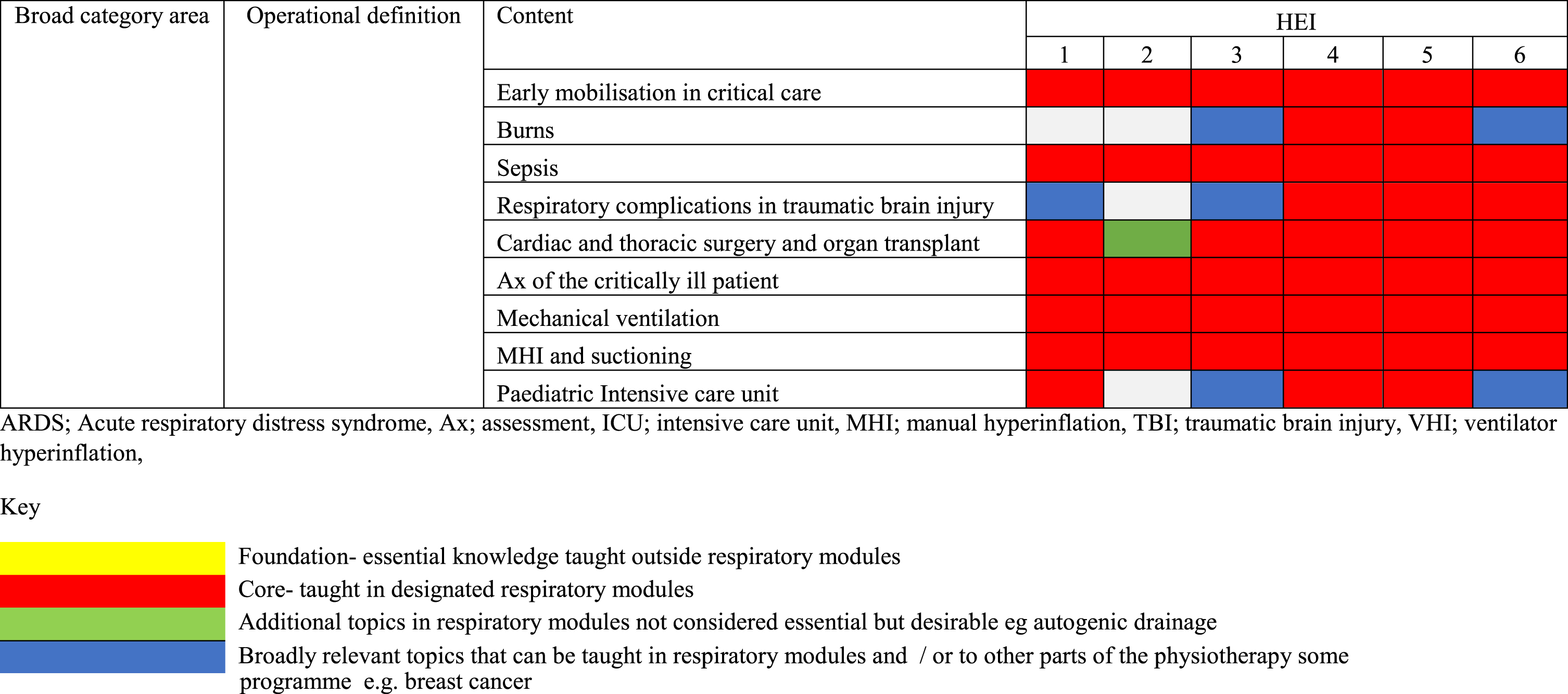
In the topic area of ‘Fundamentals of cardiorespiratory physiotherapy’ (Table 2A), anatomy and physiology were considered fundamental to the respiratory module in 50% of programmes (n = 3). Gas transport and control of ventilation was covered as a fundamental area of practice in all programmes and there was a variety of responses for ‘exercise physiology and adaptations to training’. For the topic area of ‘Common respiratory diseases, (Table 2B), there was a high degree of consistency for common respiratory diseases, lung cancer and acute respiratory distress syndrome (ARDS). Paediatric cystic fibrosis was covered in another module in one programme and one programme considered pathology a core topic taught in another module. In the broad topic area of ‘respiratory assessment and measurement’ (Table 2C) there was a high degree of consistency in core topics covered within the respiratory module such as auscultation, chest x-rays, arterial blood bases, drug and oxygen therapy and respiratory assessment. Half of programmes included pharmacology within the core respiratory modules. In the area of ‘respiratory treatment and management’ (Table 2D), 100% (n = 6) considered the active cycle of breathing, positioning and manual techniques, adjuncts (including non-invasive ventilation) core to the respiratory module. On the other hand, autogenic draining was considered core in 50% of programmes, this was considered desirable but not essential in 33% of programmes (n = 2), and was not covered in one programme. In the area of ‘Respiratory management for specific populations’ (Table 2E), the only fully consistent area was surgery (n = 6, 100%), followed by heart failure and pre-operative optimisation (n = 5, 83%). There was a mixed rating for the remaining topics of end-of-life care, breast cancer, neuromuscular weakness and enhanced recovery after surgery. In the area of physical activity and exercise (Table 2F), there was no consistency across topics in terms of what was considered core to the respiratory module. In the final area of “Critical care” (Table 2G), there was consistency (n = 6, 100%) in the topics of early mobilisation in critical care, sepsis, assessment of the critically ill patient, mechanical ventilation and suctioning.
Overall, there was a fair degree of consistency in terms of topics taught between programmes within or outside of the core respiratory module. In terms of content, 18/41 (44%) of topics were unanimously rated as considered core to the respiratory module in each programme (Table 3). Less relevant topics not considered essential but desirable by at least two programmes were the following topics; exercise physiology and adaptation to training, autogenic drainage, neuromuscular weakness, enhanced recovery after surgery and pre-participation exercise screening.
Summary of core topics taught in respiratory modules
A range of assessment strategies were applied to assess knowledge, skills and depth of understanding of key concepts (Table 4). Nine of the 11 assessment strategies included more than one component. These included practical components [(objective structured clinical examinations OSCEs,) simulation scenarios, practical skills] and a written component (written examination, multiple choice exams, case study, assignments and open book exams) and one HEI included a group presentation. As part of the module assessment one HEI included the HSE Early Warning Sign (EWS) online certification. The weighting of the practical component varied from 10% to 80% and the weighting of the written assignment was from 45% to 100%.
Assessment type and weighting
OSCE: objective structured clinical examination, MCQ: multiple choice questionnaire, EWS: early warning sign *Some programmes delivered respiratory content over two years, so there are two columns for those programmes.
To the authors knowledge this is the first paper to comprehensively evaluate and categorise the respiratory physiotherapy content of pre-qualification programmes. This paper explored content across the six HEIs (offering eight prequalification Physiotherapy programmes) on the island of Ireland. Overall, broad consistency was found relating to the content of the respiratory curricula within and outside the core respiratory module. Overall, findings provide reassurance regarding the consistency of programme content and contribute comprehensively to the preparedness of graduates for practice in this area.
Forty four percent of topics were unanimously rated as considered core to the respiratory module by each programme. These broad category and content topics (Table 3) may be a useful starting point for basing the design of future respiratory modules within physiotherapy programmes. Regardless of whether topics are included within a core respiratory module –the important point is that topics are covered somewhere within the curriculum as this will vary in different institutions. For example some HEIs included anatomy and physiology as topics within a core respiratory module, while others covered these topics within dedicated anatomy or physiology modules. Similarly, pharmacology was covered outside the core respiratory modules in 50% of HSEs. This likely explains the diversity of contact hours and ECTS allocation of the respiratory modules between programmes.
Overall, there was consistency in terms of topics taught between programmes within or outside of the core respiratory module. In terms of content, greater divergence among programmes in “additional topics in respiratory modules not considered essential but desirable”, which may partly reflect research interests and clinical background of teaching staff, specialities in local placement sites and other factors. This finding is to expected and can be viewed positively and a degree of diversity in curriculum content enhances the individual course content [19].
Programmes commenced respiratory teaching at different time points e.g. year one versus year two. It is unclear at what time points during the programmes respiratory teaching is best placed and a future study could further explore this with staff, clinicians and students.
The broad range of assessments employed by HEIs indicates diversity in module objectives. All programmes included some form of practical assessment and some form of written (high and low stake) assessment, with weighting of each varying between programmes. This facilitates broad assessment of learning [20] although future works needs to determine the best assessment method in the area of respiratory physiotherapy.
Respiratory physiotherapy is a diverse subspecialty containing a wide range of topics. While we found consistency across programmes surveyed in this study, there were a number of confounding factors to consider. Firstly, this study included programmes across the Republic of Ireland and one in Northern Ireland. Despite a difference in the delivery of Health Service provision across these countries, we found that the educational content across the topic of respiratory physiotherapy was similar. As students access core learning in physiotherapy educational programmes and similarly graduates obtain post-graduate career opportunities on both sides of the border it was decided to include both countries in this research project. This draws upon best practice so that education is involved in transformation of service delivery across countries surveyed in this study. Also, an acknowledged challenge is lack of clarity as to what constitutes ‘conventional’ respiratory physiotherapy [21], partly due to the lack of a strong evidence base for many respiratory physiotherapy treatments [3, 22], resulting in a varied approach [21, 23], based on available evidence and clinical judgement. This makes choice of curricular topics more challenging. Despite these factors, we found that foundation and core topics were largely harmonised between programmes. This is aligned to the need identified at a postgraduate level to harmonise respiratory physiotherapy content [7], and uniquely we evaluated this at a pre-qualification level. The breadth of topics included ensure graduates have core competencies to work as independent practitioners in areas of prevention, early intervention and chronic disease management as outlined in the Irish Governments Health and Social Care Delivery Plan [24].
There are a number of points for consideration with this work. Firstly, within physiotherapy education and practice, the areas of cardiology and respiratory are often merged into the broader area of ‘cardio-respiratory’. Some educational institutions delivered respiratory as part of the broader topic area of ‘cardio-respiratory’ while some delivered respiratory in isolation. The area of respiratory physiotherapy can be taught across the life-span including paediatric and adult respiratory or it can be delivered as part of a separate paediatrics module. The aim of this study only related to the sub-speciality of respiratory physiotherapy but some overlap was unavoidable due to the integrated nature of some curricula. Replicating this work in the topic area of cardiology would be a useful follow-on study. Secondly, this paper was based on the pre-COVID curriculum but the dynamic nature of curricula should be acknowledged. It is likely that many curricula may have added this topic to their suite of education content since the emergence of the COVID-19 pandemic in 2020 which was not captured in this work. It is possible that other topics may have been added or removed as a result of keeping evidence and current practice under review. It is highly likely that differences in assessment have emerged in response to the move online since data collection for this work. Thirdly, efforts have been made at a postgraduate level [1] but not at pre-qualification level to develop a consensus on learning objectives or instructional methods and no curriculum guidance documents exist to benchmark the content against which is available in other areas [25]. Therefore, we did not map content the above documents or to credentialing requirements in Ireland or the UK as they are not specific to the pre-qualification respiratory physiotherapy area.
There were a number of limitations to this study. A formal process to seek agreement of division of curricular topics was not undertaken. Teaching methods (lectures, small groups, simulation and inter-professional learning) and discipline of the lecturer were not explored Also dedicated contact hours for each topic were not included as this does not quantify the depth of material covered, and hours would naturally vary in the two year pre-registration, three year and four-year programmes included in this work. A further limitation was that while we evaluated respiratory syllabus items, we did not evaluate consolidation and revisiting of knowledge to develop higher order knowledge, skills or competencies which should be explored in future studies as well as tracking curricular content over time. Finally, we did not include feedback from students or teaching leads or evaluate ‘workplace readiness’ of students. It must be acknowledged that the level of preparedness of graduates for practice in this area is based on those who design the respiratory curriculum. While this study evaluates the curricular content of pre-qualification respiratory physiotherapy, it is acknowledged that clinical placement is where students consolidate knowledge and build on critical hands-on skills in the real-world setting. The contribution of clinical placement to respiratory physiotherapy education was not evaluated in the present study.
A strength of this study was the inclusion of both the Republic of Ireland and Northern Ireland to form a complete All-Ireland picture which increases the relevance of results and gives an accurate contemporary picture of respiratory pre-qualification physiotherapy programmes. This is also important for work force mobility as students may study in one country and work in another and results should be transferable to wider UK settings. Transferability of results to settings beyond Ireland and the UK is not fully known.
In conclusion, despite diversity in contact hours, ECTS credit and assessment weighting, this study provides evidence that largely consistent respiratory physiotherapy content is delivered across physiotherapy programmes on the island of Ireland. It matters little whether content is covered within a specialist respiratory module or within broader modules as long as core material relevant to respiratory physiotherapy is included within programmes. This study was a useful first step in the evaluation of respiratory physiotherapy within pre-qualification programmes and may inform future curriculum development in this key area of physiotherapy practice.
Conflict of interest
The authors have no conflict of interest to report.